File - Michael E. Carey`s Portfolio

Austin Chute
Michael Carey
Drugs & Human Behavior/ Dr. Jarcho
12/05/2013/ Fall 2013
Research Paper Final Draft
“Krokodil (Desomorphine)”
Krokodil: Exploring the Deadly Designer Drug
What is Krokodil? Upon first hearing the word “Krokodil,” one may be inclined to conjure up thoughts regarding those four legged, green, scaly aquatic creatures that live in and around rivers and swamps; however this term has become street slang for a vicious designer drug ravaging countries throughout Eurasia (Grund, Latypov, & Harris, 2013). While the more commonly known pharmaceutical equivalent form of krokodil (Desomorphine) is not a new drug; krokodil itself is part of a category of drugs (designer drugs) of which very little is known.
As both the production and use of synthetic variants to pure illicit drugs has dramatically increased over the past decade, one of the biggest issues that has arisen out of this “innovative approach” to creating more accessible ways of using drugs is the fact that there is a huge absence of scientific information pertaining to the use of these types of drugs. This lack of readily available knowledge includes such factors as the current trends pertaining to who
(demographics) uses these types of drugs and to what extent (how often the drug is used, as well as how much of the drug is used). And moreover, what the driving factors are behind choosing these designer drugs over the use of the more common street drugs that they are typically substituted for. With that being said, since little research exist on the topic of synthetic drugs, little is known about the true effects and consequences associated with the use of these types of drugs.
This lack of readily available knowledge concerning the use of synthetic drugs, in turn becomes especially problematic for exploring krokodil usage, because krokodil is relatively new,
1
and as result has just recently begun to be studied (Steenholdt, 2012). To better illustrate this issue, take for instance the scenario in which after conducting a thorough search for information pertaining to krokodil, Grund, Latypov, and Harris discovered that there was a significant lack of published academic material pertaining to this topic. Moreover, out of a search yield of 60
“articles,” only 11 were relevant (Grund, Latypov, Harris, 2013). With that said, the objective is to review the relatively scarce information that exists about the new designer drug krokodil. In addition, this paper will discuss the, at best, “rough estimates,” concerning the usage, risk factors, and yet to be fully understood consequences of the drug krokodil.
Setting the Stage: Background Information Concerning Russia’s Drug Scene
Eurasian countries such as the Ukraine, Russia, Georgia, and other former Soviet Union countries bare a long engrained history of producing “homemade” opioid injectable drugs predating the fall of the Soviet Union (Grund et al., 2013). This obsession with the production of
“homemade” opioid injectables has included such drugs as heroin, Methamphetamine, and methcathinone. While homemade drug production predates the fall of the Soviet Union, both the strict drug policies, as well as the unique approaches to narcology (Russian term for the treatment of drug addiction/addicts) that existed during the Soviet era dramatically limited both the production and usage of homemade drugs during this period (Grund et al., 2013). In essence, an element of control that was derived largely from the rather extreme penalties, medical treatments, and social stigmas, that were associated with the socially deemed “deviant” behaviors of drug usage (Heimer, 2013). However, the political changes that occurred in many post-Soviet countries spanning the 1990’s brought with it, the rapid, sweeping return of such previously limited homemade drug production to a scale of new proportions (Grund et al., 2013).
2
This resurrection in the homemade drug production trend lasted until the late 90’s when porous borders allowed imported heroin from Afghanistan, Kazakhstan, and other Central Asian states to flood the illicit drug market. In turn, the new surplus in mass produced heroin effectively replaced, and thereby curbed the production of homemade opioids in this region.
Specifically, imported heroin stomped out the production of homemade opioids in Russian cites, as well as towns/cities that were directly on, or adjacent to, the heroin trafficking routes from exporting countries previously mentioned (United Nations Office on Drugs & Crime, 2008).
While the flood of imported heroin nearly crushed the home based production of opioids in Russia during the late 90’s, it did not have as significant an effect on the home produced drug market in other areas (Grund et al., 2013). Specifically in regions of the Ukraine, and other countries where the flow of imported drugs was not as strong or widely available as it was in
Russia, home based production of opioids remained relatively constant. It was not until the early
2000’s, when new drug policies specifically targeting heroin trafficking, and other opioids, such as poppy straw and raw opium, that an opium “drought” occurred. This drought in turn brought on a revival in home based productions (of opioids) in Russia to the levels seen prior to the flood of imported heroin during the late 90’s (Grund et al., 2013). However, while home based production returned to a relatively high level, the most drastic explosion in the volume of home manufactured opioids did not occur until the European economic crises reached its tipping point in 2008 (Booth, 2013).
Understandably, one of the reasons for this drastic increase in the production of homemade opioids, specifically the “birth” of homemade heroin (krokodil), is in large part due to the fact that the relatively inexpensive products required for the production of homemade drugs results in more economically accessible “scores” for drug users/addicts (Grund et al., 2013).
3
In terms of the production of krokodil, the inexpensive household type products required for its production result in “scores” (an injection of the drug required for a single high) that cost roughly between 4 to 5 euros (about 6 to 7 U.S. dollars) (Booth, 2013). This price is significantly cheaper than a gram of brown heroin which has a street price of roughly 35-40 euros (roughly
48-55 U.S. dollars) (the street price of pure heroin in European countries varies from 27 to 110 euros, depending on both supply and market saturation)( (United Nations Office on Drugs &
Crime, 2010). From 2008, use of homemade opioids, specifically krokodil, is thought to have reached its peak throughout these post-Soviet Union countries in 2011 (Grund et al., 2013)
Desomorphine & Krokodil
Desomorphine is an opiate analogue that was first synthesized by Dr. Lyndon Small in the U.S. in 1932 (Grund et al., 2013). Dr. Small was appointed director in charge of Chemical
Research for the Drug Addiction Laboratory at the University of Virginia in
1929. During a 10 year period, Dr. Small and his research group consisting of
Ph.Ds. and graduate students were tasked with a long series of masterly and painstaking studies on morphine and allied compounds
(Mosettig, 1959).
The synthesis of desomorphine occurred while Dr.
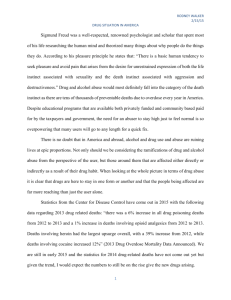
Figure 1: The molecular structure of
Desomorphine: Its IUPAC name is 4, 5-a-epoxy-
17 methylmorphinan-3-ol and its formula is
C17H21N02. As previously mentioned,
Desomorphine (dihydrodesoxymorphine,
Permonid) is an opioid analogue that is a derivative of morphine, except the 6-hydroxl group has been removed and the 7, 8 double bond has been reduced.
Small and his research group were exploring methods to solve the problem of finding non-habituating drugs to treat chronic pain (Mosettig, 1959). The approach consisted of two avenues. The first approach utilized a hypothesis that proper modification of the functional groups of the morphine molecule compounds could
4
diminish undesirable effects such as nausea and respiratory depression, while at the same time enhancing the drug’s analgesic effects. The second approach was to introduce functional groups of morphine into simpler ring systems and stepwise build up synthetics resembling in one or more ways the morphine molecule (Mosettig, 1959). After it’s synthesis in 1932, desomorphine was used as an alternative to morphine for several reasons.
Specifically, desomorphine was associated with decreased likelihood of side effects like nausea, and an elimination of the reduced respiratory rates that were typically experienced with morphine use. In addition, desomorphine is 8 to 10 times more potent, and has a much more rapid onset than morphine. In fact, 1 mg of desomorphine was found to be roughly the equivalent of 10 mgs of morphine (Eddy, Halbach, & Braenden, 1957). All of these factors made it an attractive alternative to regular morphine. However, further studies revealed several drawbacks with the two most important factors concerning:
1) Its drastically shorter durations of desired sedative effects, thus requiring more administered doses to achieve the desired target response.
2) Drastically higher tendencies for the development of substance dependence, compared to regular morphine.
With that said, it is easy to see the inherent problems associated with a medical sedative/pain reliever that possesses a high opportunity for the development of substance dependency, combined with the fact that desomorphine requires more frequent dose administrations to be effective, compared to its earlier counterparts. That is, desomorphine was extremely problematic, because it led users to become rapidly addicted, on a scale that was much faster and far greater than morphine.
5
Since desomorphine is a derivative of morphine, and given the fact krokodil is typically substituted for heroin, it is than believed that krokodil—once administered—works within the body much the same way as morphine and/or heroin. The exceptions are that desomorphine/krokodil has a 10 time’s stronger analgesic effect and 3 time’s greater toxicity than morphine/heroin.
Opioid receptors consist of several subtype receptors and are widely distributed throughout the central nervous system; with each subtype of opioid receptor being differentially distributed (Julien, 2001). That is, some regions of the central nervous system contain all three subtypes of receptors (the spinal cord), while other regions consist of predominantly one type of receptor. Since morphine and heroin are classified as pure agonist opioids, primary focus is centered on their interactions with mu receptors (Julien, 2001). This is because agonism of mu receptors invariably results in both the analgesia and euphoria associated with administration of these drugs. In addition, agonism of mu receptors is also largely responsible for the propensity of these drugs to cause substance dependence (Julien, 2001). This is because morphine and heroin modify the action of dopamine in the nucleus accumbens and the ventral tegmental area of the brain – which are areas that form part of the brain’s “reward pathway” ( Katzung, 2001).
Specifically, once administered, heroin crosses the blood-brain barrier rather quickly
(unlike other molecules or one hundred times faster than other opiates like morphine). Once across the blood-brain barrier, heroin hydrolyzes into 6-monoacetylmorphine which in turn hydrolyzes into morphine (Zovko, 2009). Once converted to morphine, the opiate attaches and binds to open mu receptors located in the central nervous system. This binding inhibits the release of GABA from the nerve terminal, reducing the inhibitory effect of GABA on dopaminergic neurons (Katzung, 2001). In turn, both the increased activation of dopaminergic
6
neurons and the release of dopamine into the synapse results in sustained activation of the postsynaptic membrane (Zovko, 2009). Continued activation of the dopaminergic reward pathway leads to the feelings of euphoria and the ‘high’ associated with heroin use (Katzung, 2001).
Furthermore, while the use of heroin does not always lead to death, long-term continued use wreaks havoc on the body (Zovko, 2009). These long-term effects include collapsed veins, liver disease, pulmonary complications, kidney disease, heart problems, and respiratory complications (Zovko, 2009). With that being said, krokodil is believed to act upon its users in the previously mentioned fashion, merely quicker and with greater affinity.
With a 10 times stronger analgesic effect, desomorpine is vastly stronger and more addictive than heroin (Grund et al., 2013). These are all important factors to consider for several reasons. One of the reasons it is important to have a relatively firm understanding of the nature of desomorphine is due to the fact that the designer drug Krokodil is essentially a “bootleg” version of the pharmaceutical drug desomorphine (Grund et al. 2013). In essence, krokodil is derived from a two-step conversion process in which codeine is transformed into desomorphine.
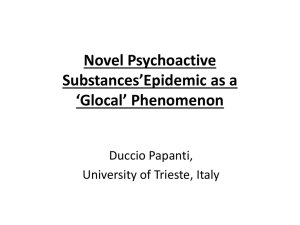
The process of manufacturing Krokodil first begins with the extraction of codeine from over-the-counter medications. Once the codeine has been extracted, codeine molecules are reconstructed into what is believed to be a crude version of desomorphine (Grund et al., 2013).
This processes is illustrated in figure 2, in which Thlonyl chloride acts as a catalyst in the reconstruction of
7
Figure 2: Conversion Diagram.
codeine to the crude, often unpredictable form of desomorphine commonly referred to as krokodil (under this context, unpredictable referrers to both the variations in deomorphine that are actually achieved, in terms of its yield and exact composition, as well as presences of other contaminates/residual substances that may be contained within the resulting concoction). Thus, granted that krokodil is essentially a crude version of desomorphine, taken into consideration with the previously discussed powerfully addictive quality, it is easy to understand why krokodil possesses such a powerfully addictive nature.
Production of Krokodil
As previously discussed, the homemade production of krokodil involves a two-step transformation of codeine into desomorphine (Grund et al., 2013). This transformation is carried out in a process that is very similar to the manufacturing process of homemade methamphetamine in the United States. The manufacturing of desomorphine typically involves small quantities of over-the-counter precursor drugs (generally codeine based painkillers), combined with low cost household/commercially available chemicals (Grund et al., 2013). These chemicals include such products as iodine, strong alkalis (that are obtained from batteries or industrial solvents) (“Mr. Muscle or Krot”), hydrochloric acid, red phosphorus (obtained from match heads), and organic solvents (such as gasoline, ethyl acetate, or paint thinner) (Grund et al., 2013).
Similar to the homemade production of meth, the process of manufacturing homemade krokodil begins when codeine pain relievers (in the form of tablets or syrup) are mixed with gasoline, or another strong alkali in some sort of sealable bottle—most commonly an empty plastic beverage container. Following the combination of codeine with an alkali, the solution is then mixed with acidified water and then given a chance to rest. After some time, the solution
8
separates into two parts—the aqueous part containing the codeine, and gasoline which is assumed to contain all other chemicals and ingredients. From there, the aqueous part is poured into another container—at which point some “cooks” may dry out the codeine, while others simply use the codeine solution.
After the extraction of codeine has taken place, the extracted codeine is then mixed with iodine, red phosphorous, and hydrochloric acid—usually in some sort of glass container or enamel pot—which allows the final reaction to occur. Once the final reaction has taken place, the
“cook” is left with a crude form of desomorphine (Grund et al., 2013). This manufacturing of krokodil all occurs in a process that takes anywhere between 45 minutes to 2 hours to preform— with the duration in time depending largely upon the skill of the individual manufacturing it.
The process of manufacturing krokodil is almost the identical process employed in the production of homemade meth, with the exception being that in the production of meth, pseudoephedrine is the precursor drug transformed instead of codeine (Grund et al., 2013). In addition, this process parallels the manufacturing of homemade meth in terms of the duration of time it takes to produce the resulting drug (Haupert, McClimon, Pregler, 2012). Just as there are numerous variations in the techniques used to manufacture homemade meth, there are too numerous variations employed in the production of krokodil. However, the above described process appears to be the most simplistic avenue for manufacturing krokodil, and thus appears to be the most commonly employed avenue for production. Furthermore, when all is said and done, the process of manufacturing krokodil results in an amount of desomorphine that is roughly the equivalent to around 12 euros of heroin (Grund et. al, 2013).
As one may assume, this process results in a crude concoction that also contains many other residual ingredients in addition to the desired desomorphine. For instance, concoctions of
9
krokodil have often been found to contain residual contaminates such as those found in the chemical solvents used to create the exothermic reaction. In addition, other residual contaminates include compounds such as paracetamol, caffeine, and/or terpinhdrate, which are left over from the codeine that was originally broken down. With that being said, one of the main debates surrounding the drug krokodil centers on the question as to whether the individuals manufacturing it are actually successful in their attempts to transform codeine into desomorphine in the first place. However, samples that were tested did in fact show the presence of desomorphine ranging from trace amounts all the way up to 75% conversion (Grund et al.,
2013). Thus, the actual psychoactive content of krokodil varies greatly depending on the avenue employed in its production, as well as the medications used, and the reagents/chemicals that are available to manufactures from local markets (Grund et al., 2013).
Risk Factors & Complications
Given the context of the manufacturing process employed in the production of krokodil, there are numerous physical complications associated with its injected use. While there have always been physical complications that result when injectable street drugs are used, those associated with the use of krokodil appear to be extreme and unprecedented. For instance, one of the most pronounced physical complications that arise out of the use of krokodil is its rapid, extreme destruction of skin, soft tissue, and venous damage (Grund et al., 2013). At first, the skin surrounding injection sites begins to change to a greenish, brownish color, as well as become scaly in texture and appearance. Hence one of the reasons for its street name “krokodil” is derived from the fact that it turns its user’s skin into something that resembles the greenish/brown scales of a crocodile (Grund et al., 2013). Other reasons for the street reference
“krokodil” are derived from the devastating physical complications that result from its use, in a
10
manner such that the user’s body is literally eaten alive from infection and the drug’s toxicity, as well as the fact that one of the substances that occur during the conversion process is chlorocodide (Grund et al., 2013).
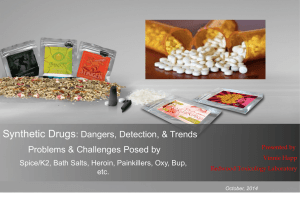
In a short time after the skin surround injection sites has changed color, large ulcers begin to from on soft tissues and limbs elsewhere on the body. From there, as skin and veins begin to rot, gangrene begins to set in (Booth, 2013). At this point, gangrene further eats
Figure 3: Damage to arm caused by gangrene and infection. Soft tissue and muscle destroyed to the bone. away tissues, muscles, and veins—in most cases all the way to the bone. If left unchecked— which it often is, as several experts have stated that more often than not, the scenario involves individuals only seeking medical attention after their body has reached a point in which it is no longer repairable—rampant infections and tissue/muscle/venous damage typically result in the amputation of limbs (Grund et al., 2013).
Other observed complications include, thrombosis of the major vessels and arrosive bleedings, veins that ulcer and rot away from the inside requiring surgical removal of the main veins in arms or legs, including the surrounding soft tissue and muscles, pneumonia, blood poisoning, coronary artery bursts,
Figure 4: Decaying facial structure. meningitis, rotting gums resulting in tooth loss, and bone infection, decayed structure of the jaw and other facial bones (Grund et al., 2013). In addition, still others include, sores and ulcers on the forehead and skull, rotting ears, noses and lips, sever liver and kidney damage, speech impediments, motor
11
skill impairments, affected memory and concentration problems, personality changes, and lastly, with extended usage, death (Grund et al., 2013).
Two issues that are most worrisome to health officials regard the fact that:
1) These extremely severe complications appear to manifest in an accelerated
2) manner, within a short period of time after use of krokodil is initiated.
These sever physiological complications are typically left untended, to the point that medical treatment is unsuccessful in halting and/or repairing the damage.
This in turn results in the almost assured probability that a user will die within 2 to 3 years after initial usage begins (Grund et al., 2013). There is some debate as to whether this reduced life expectancy of 2-3 years after initial usage is entirely true, or rather a grisly scare tactic employed by the Russian government in an attempt to reduce beginning usage of krokodil
(Grund et al., 2013). Much of this debate is derived from the fact that few studies have actually covered this “new Russian epidemic” in enough detail (Heimer, 2013). However, based on the observed complications that result from its usage, it is not unreasonable to assume that this 2-3 year life expectancy is realistic (Grund et al., 2013). Consider for a moment the drastic, accelerated physical damage and change that has been documented and observed in meth addicts, in addition to their documented reduction in life expectancy. Thus, with a drug that appears to elicit far more drastic complications, both in their terms of seriousness, as well as accelerated onset of complications, this claim appears to be relatively accurate (Booth, 2013).
Another aspect of interest to health officials/care provides are that several of the observed complications have manifested in areas that are not typically used as, or associated with drug injection sites. This seems to importantly suggest that the adverse effects of krokodil are not
12
contained to the typical localized injuries that result from the injection and infection associated with the use of other injectable drugs. Moreover, these observations seem to suggest that krokodil possesses a rather remarkable ability to rapidly spread throughout the body manifesting itself in neurological, endocrine, and organ damage that has never been observed in the use of other street drugs (Heimer, 2013). This remarkable ability to rapidly spread seems to be associated with the chemicals and heavy metals that are common residual components krokodil’s bootleg production (Grund et al., 2013).
Further exacerbating the health complications associated with the use of krokodil is the relatively extreme environmental risk factors in which the use of the drug occurs. These factors include not only the manner in which krokodil is dispensed from dealers/distributed amongst friends who produce it, but also to Russia’s HIV/Aids and Hepatitis C rich environment, and to the ostracism from medical care for people who use drugs.
For starters, krokodil use appears to exist within a relatively exacerbated risk environment in terms of a large populace with infectious diseases. According the Russian
Federal Ministry of Health and Social Development, it is estimated that there are at least 1 million HIV cases in Russia (United Nations, 2008). In addition, the use of krokodil occurs in a society (Russia and other former Soviet countries) with a strong preference for injecting drugs over other forms of drug administration (Grund et al., 2013). While the use of injectable drugs is extremely risky behavior by itself, the situation seems to be further exacerbated by the commonly employed dispensing methods by dealers. Krokodil is typically dispensed in one of two methods:
1) Front loading syringes—a method in which a large volume of the drug containing the equivalent of several doses is loaded into a syringe, and then
13
2) subsequently passed around a group, where each member injects his/her desired “hit.”
Container/vial sharing—a method is which krokodil is contained within one container/vial, from which each party loads their syringe, simultaneously, or subsequently passed around.
Either way, both methods place users at an elevated level of risk in terms of contracting and/or spreading infectious diseases like HIV/AIDs/Hepatices C, that are widely abundant in this populace.
Furthermore, according to the official statistics of the Russian Federal Ministry of Health and Social Development, the number of registered users of illicit drugs is more than half-amillion individuals. Of that half million registered users; more than 67% of them are registered as drug dependent individuals. In addition, the vast majority of those registered as drug dependents are classified as opioid abusers (United Nations, 2008).
Finally, Soviet era narcology (Soviet approach to the treatment of drug addiction and addicts) has garnered a society in which the social stigma attached to drug usage vastly limited both the number of treatment facilities available for drug addicts, as well as the ease to which access is granted to these few institutions (Grund et al., 2013). In addition to a lack of available treatment facilities, the social stigma has often lead to a vilification of drug users within this society. That is once admitted to a treatment/care facility, drug users are often treated in inhumane ways, as to somehow be further punished for bringing such “disgrace and destruction” upon themselves from their decision to use drugs (Grund et al., 2013). For instance, while researching krokodil, Grund et al. found numerous stories in which individuals who entered
14
treatment facilities, received medical attention that was considered rather “barbaric,” and without the use of pain-relievers/analgesics (Grund et al., 2013).
One of the most graphic examples pertained to an individual whose leg had dissolved to the bone, with only the foot consisting of flesh, below the kneecap. Upon entering the hospital, the individual was sat in a wheel chair in the facility’s waiting room and a bucket lined with a trash bag placed under his leg. At that time, the medical staff than proceeded to cut off the individual’s leg, at a spot of exposed bone,
Figure 5: Real picture of described leg amputation. just below the kneecap, without the use of any sedative or analgesics (Grund et al., 2013).
As mentioned earlier, this often inhumane treatment of drug addicts prevents individuals from seeking timely medical help for the complications/consequences that arise with the use of krokodil. And again, because of this fear, if and when medical treatment is sought out, the damage is almost always beyond repair (Grund et al., 2013).
Taken all together, it is easy to see how the use of a highly destructive drug being used in a populace that possesses large numbers of infected individuals (HIV/AIDs/Hep. C), large numbers of individuals addicted to opiates, and a populace that receives substandard medical/substance treatment has exacerbated the consequences of using krokodil.
Conclusion
While relatively little information exist on the relatively new designer drug krokodil, one thing that seems to be abundantly evident in the observations made to date is that it is a drug with far more destructive consequences than any other illicit street drug. Since research was initiated, krokodil has crossed over into the United States and has resulted in a handful of documented
15
cases. While krokodil is obviously a highly destructive drug by itself, it is unclear to what extent the consequences observed with its use in former Soviet Union countries will be observed in those who use it in the United States. It is true that the United States has a slightly higher incidence of HIV/AIDs cases, at roughly 1.1 million infected individuals; however unlike former
Soviet Union countries, the U.S. possesses far better treatment/medical options (needle exchange programs, and more drug treatment facilities/clinics—with easier access) (CDC, 2013). Thus, this fact may help to at least slightly diminish the horrific consequences that are currently being observed in Russia, as a result of the exacerbated risk environment in which krokodil usage has occurred.
16
References
Booth, R. (2013). ‘krokodil’ and other home-produced drugs for injection: A perspective from ukraine . Retrieved from http://www.ijdp.org/article/S0955-3959(13)00083-2/fulltext
Centers for Disease Control and Prevention, (2013). Hiv in the united states: At a glance.
Retrieved from website: http://www.cdc.gov/hiv/pdf/statistics_basics_factsheet.pdf
Eddy NB, Halbach H, Braenden OJ. "Synthetic Substances with Morphine-Like Effect".
Synthetic Substances with Morphine-Like Effect 1957; 17:569-863
Grund, J. -P. C., et al. Breaking worse: The emergence of krokodil and excessive injuries among people who inject drugs in Eurasia. International Journal of Drug Policy (2013), http://dx.doi.org/10.1016/j.drugpo.2013.04.007
Harris, M. (2012). The ‘do-it-yourself’ new zealand injecting scene: Implications for harm reduction. Retrieved from http://www.ijdp.org/article/S0955-3959(12)00102-8/fulltext
Haupert, D., McClimon, T., Pregler, T., (2012). Narcotics Investigations [Dubuque Citizen’s
Police Academy]. Dubuque Police Department February 2012., 13-week Law
Enforcement Training Session.
Heimer, R. (2013). Patterns of new drug emergence: A comment in light of ‘krokodil’. Retrieved from http://www.ijdp.org/article/S0955-3959(13)00096-0/fulltext
Julien, R. (2001). A primer of drug action: A concise, nontechnical guide to the actions, uses and side effects of psychoactive drugs. New York, New York: Henry Holt and Company,
LLC.
Katzung, BG. 2001). Opioid analgesics and antagonists. In: Basic and clinical pharmacology, 8th edition. USA: The McGraw Hill Companies, Inc, 2001:512–531
17
Mosettig, E. (1959). Lyndon Fredrick Small 1897—1957 a biographical memoir . Retrieved from http://www.nasonline.org/publications/biographical-memoirs/memoir-pdfs/smalllyndon.pdf
Sikharulidze, Z. (2013). Desomorphine (“crocodile”) injection among in-treatment drug users in tbilisi, georgia. Retrieved from http://www.drugabuse.gov/international/abstracts/desomorphine-crocodile-injectionamong-in-treatment-drug-users-in-tbilisi-georgia
Steenholdt, D. (2012, 09 01). Drugs by design-legal highs? n.p.s overview. Retrieved from http://50.87.55.75/~dalgarno/images/resources/pdf/research-documents/DRR-Legal-
Highs.pdf
The neurobiology of drug addiction. National Institute on drug abuse, National Institutes of
Health. http://www.nida.nih.gov/Teaching2/teaching5.html
United Nations Office on Drugs and Crime, (2010). cocaine retail prices (street prices), us$ per gram cocaine. Retrieved from website: http://www.unodc.org/unodc/secured/wdr/Cocaine_Heroin_Prices.pdf
United Nations Office on Drugs and Crime Regional Office for Central Asia, THE PARIS PACT
INITIATIVE A partnership to counter traffic in and consumption of Afghan opiates.
(2008). Illicit drug trends in the russian federation. Retrieved from Korovy Val str.,
Office 103, UNODC RORB, Moscow, 119049, Russian Federation website: http://www.unodc.org/documents/regional/central-asia/Illicit Drug Trends
Report_Russia.pdf
18
Zovko, A. (2009). The pharmacological effects of diacetylmorphine (heroin) after diffusion through the blood-brain barrier. Retrieved from http://review-of-currentresearch.stsd.wikispaces.net/file/view/The Pharmacological Effects of Diacetylmorphine
(Heroin) After Diffusion Through the Blood-Brain Barrier.pdf
19