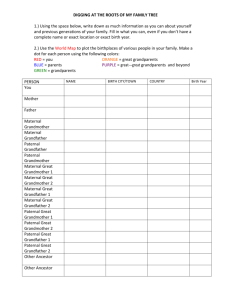
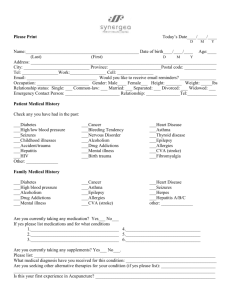
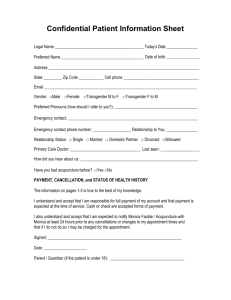
Health history questionnaire
advertisement

Original Date: Spokane Psychiatric Clinic, P.S. Dates Revised: HEALTH HISTORY QUESTIONNAIRE All questions contained in this questionnaire are strictly confidential and will become part of your medical record. Name M (Last, First, M.I.): Marital status: Single Partnered Married Separated Previous or referring doctor: Divorced F DOB: Widowed Date of last physical exam: PERSONAL HEALTH HISTORY List any medical problems that other doctors have diagnosed Surgeries Year Reason Hospital Other hospitalizations Year Reason Hospital Have you ever had a blood transfusion? List your prescribed drugs and over-the-counter drugs, such as vitamins and inhalers Name the Drug Strength Allergies to medications Name the Drug Reaction You Had Frequency Taken Yes No HEALTH HABITS AND PERSONAL SAFETY ALL QUESTIONS CONTAINED IN THIS QUESTIONNAIRE WILL BE KEPT STRICTLY CONFIDENTIAL. Exercise Sedentary (No exercise) Mild exercise (i.e., climb stairs, walk 3 blocks, golf) Occasional vigorous exercise (i.e., work or recreation, less than 4x/week for 30 min.) Regular vigorous exercise (i.e., work or recreation 4x/week for 30 minutes) Caffeine None Coffee Tea Cola # of cups/cans per day? Alcohol Do you drink alcohol? Yes No Are you concerned about the amount you drink? Yes No Have you considered stopping? Yes No Have you ever experienced blackouts? Yes No Are you prone to “binge” drinking? Yes No Do you drive after drinking? Yes No Do you use tobacco? Yes No If yes, what kind? How many drinks per week? Tobacco Cigarettes – pks./day # of years Drugs Personal Safety Chew - #/day Pipe - #/day Cigars - #/day Or year quit Do you currently use recreational or street drugs? Yes No Have you ever given yourself street drugs with a needle? Yes No Do you live alone? Yes No Do you have frequent falls? Yes No Do you have vision or hearing loss? Yes No Do you have an Advance Directive or Living Will? Yes No Would you like information on the preparation of these? Yes No Physical and/or mental abuse have also become major public health issues in this country. This often takes the form of verbally threatening behavior or actual physical or sexual abuse. Would you like to discuss this issue with your provider? Yes No Family Health History AGE SIGNIFICANT HEALTH PROBLEMS AGE Children Father Mother Sibling M F M F M F M F M F M F Grandmother Maternal Grandfather Maternal Grandmother Paternal Grandfather Paternal M F M F M F M F SIGNIFICANT HEALTH PROBLEMS MENTAL HEALTH Is stress a major problem for you? Yes No Yes No Do you panic when stressed? Yes No Do you have problems with eating or your appetite? Yes No Do you cry frequently? Yes No Have you ever attempted suicide? Yes No Have you ever seriously thought about hurting yourself? Yes No Do you have trouble sleeping? Yes No Have you ever been to a counselor? Yes No Do you feel depressed? Please rate your depression - on a scale of 1-10 - with 0 being none and 10 being worst ever/couldn’t be worse __________ REVIEW OF SYSTEMS Circle those items you currently have problems with, and describe: GENERAL Recent Weight Change Increased Thirst or Urination Night Sweats/Hot Flashes Always Hot/Always Cold Rashes or Skin Problems Do you have chronic pain problems? Yes No Significant Fatigue BREASTS: Men & Women Lumps/Tenderness EYE, EAR, NOSE, AND THROAT Glaucoma Blurred or Double Vision- Ever Use Glasses or Contact Lenses Hearing Loss Brief Loss of Vision- Ever Use Dentures (Partial or Total) History of Radiation Therapy to Head or Neck Teeth or Gum Problems CARDIOPULMONARY Shortness of Breath With Activity Dizziness Chest Pain Daily Sputum (Phlegm) Production Coughing Up Blood Heart Palpitations Difficulty Breathing While Lying Flat Leg Cramps While Walking Wheezing Waking Up Short of Breath Daily Cough Ankle Swelling GASTROINTESTINAL Change of Appetite Abdominal Pain Blood in Stool/Black Stool Difficulty Swallowing Diarrhea/Constipation Heartburn Indigestion From Fatty Foods Frequent Nausea/Vomiting NEUROPSYCHIATRIC Frequent Disabling Headaches Difficulty Sleeping Tremors Frequent Anxiety or Anxiety Attacks Memory Loss Passing Out/Fainting Treated in Past for Emotional or Psychological Problems: please describe _____________ Often Feel Sad or Depressed MUSCULOSKELETAL & SKIN Frequent Neck or Back Pain Muscle Pain Disabling Night Leg Cramps Joint Problems Use a Brace or a Splint Mole that has changed color, size, shape, or won’t heal? Yes No GENITOURINARY: MEN & WOMEN Urinary Tract Infections Sores in the Genital Area Difficult or Painful Urination Blood in Urine History of Kidney or Bladder Stones Urination More Than Once a Night GENITOURINARY: MEN ONLY Pain or Lump in Testicles/Scrotum GENITOURINARY: WOMEN ONLY Number of Pregnancies: ____________ Number of Children: ________ Disabling Menstrual Cramps PMS Symptoms