PDSA Cycle Summary. - BMJ Quality Improvement Reports
advertisement

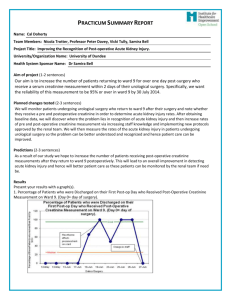
PDSA Cycle 1 Aim: what are you trying to accomplish? The aim is to collect data around patients undergoing urological surgeries from Monday to Friday of the week beginning 12/5/2014. This data will show how many patients receive a post-operative creatinine after their urological operation and when this blood test occurs. Plan: what will your test be? In order to collect this data a table has been devised which will be filled in with the correct information. Data will be collected on a daily basis so it can be reviewed at the end of each day to assess whether the data collection tool worked effectively. Prediction: what do you think will happen as a result of your test? 1. The majority of patients will receive a pre-operative serum creatinine. 2. Only a minority of patients will receive a post-operative serum creatinine. 3. The majority of patients will not receive gentamicin prophylaxis due to risk of renal failure. 4. The data required will all be stored in the patient's notes. Do: what happened when you carried out your test? Post-operative creatinine does not occur routinely and is not recorded in patients' notes. In order to find out whether this measurement has been taken, we needed to access the ICE data base to search for blood results using the patient's CHI number. The original plan was time consuming and did not allow for us to collect the data we needed. Firstly, as stated above the patients' notes did not contain all the information we needed so we had to start using ICE. Furthermore, following each patient and finding their notes was very time consuming. To increase our efficiency we attended the anaesthetic meetings in the morning to find out what antibiotic prophylaxis the patients were on. More over, we discovered we could use clinical portal to access the pre-assessment form and so did not need to obtain this from the patient's notes either. BMJ Quality Improvement Programme PDSA Template Study: how did the results of your test compare with predictions? The majority of patients did receive a pre-operative serum creatinine, however a great disparity over the length of time before patients’ operations and when they last received a creatinine measurement was noted. Only a minority of patients received a post-operative serum creatinine. After analyzing the results distinct correlations between the percentage of patients receiving a creatinine measurements with how long they remained in hospital for was observed. The majority of patients did receive gentamicin prophylaxis. A previous study carried out in NHS Tayside had shown gentamicin did not show an associated increased risk of acute kidney injury but it also raised concerns about background risk of acute kidney injury and its lack of recognition in Ninewells Hospital. This was echoed in our results as no correlation could be made between gentamicin and AKI as there was not enough post-operative serum creatinine measurements being carried out. Hence it was decided to focus on increasing the awareness of postoperative acute kidney injury and to increase the number of postoperative serum creatinine measurements carried out instead of focusing on gentamicin use. We found that results and forms are not reliably stored in patients' paper records and results such as blood tests are stored more reliably on the ICE computer system and this is the most efficient way to access these results. This realisation increased our time efficiency as well as result accuracy and is a lesson that will be very useful in the future. Act: how will you change your previous test in light of what you have learned? It was clear there is a major problem with patients receiving a post-operative creatinine measurement. Therefore, several changes need to occur. We would like to raise awareness of post-operative AKI in order to increase clinicians knowledge and culture surrounding this condition as this will provide an increase in U+Es being carried out. Moreover, in order to maintain a sustained increase in postoperative creatinine measurements we are going to work with the team to create a new protocol outlining which patients should be receiving a postoperative creatinine. In order to do this we will need cooperation from all members of the team; blood scientists, phlebotomists, urological consultants, FYs and the charge nurse etc. Continued data collection should also continue, to note any changes from the first week of data as well as having data from a larger group of patients to further prove our prediction and increase our evidence base. BMJ Quality Improvement Programme PDSA Template PDSA Cycle 2 Aim: what are you trying to accomplish? The aim is to raise awareness of the problem, identified by the data collected, amongst key stakeholders and members of staffs. To increase knowledge of AKI on the ward and gain approval and cooperation to implement a change in protocol. Inclusion of enthusiastic members of staff who could play an active role in the project, is an additional aim. Due to the limited time frame, this should be achieved in one week. Plan: what will your test be? The findings of the project will be explained and the call for a change in protocol suggested to specific individuals whose cooperation would be vital in implementing a change. This includes key members of the urology, phlebotomy and blood science team. This would be done through arranging meetings with these individuals. The project and its findings so far will also be explained on the ward, to raise awareness of the problem and identify enthusiastic members of staff. Prediction: what do you think will happen as a result of your test? 1. There will be a varying response and enthusiasm from staff member, which will include some resistance to change. 2. Members of staff will be identified, on ward 9, who could play an active role in implementing further change 3. Cooperation and approval will be achieved from key stakeholders 4. This will be achieved in a short amount of time BMJ Quality Improvement Programme PDSA Template Do: what happened when you carried out your test? Engaging and raising awareness with staff on ward 9 was successful. Paticularly amongst the junior doctors and specific nurses. Due to our presence on ward 9, we were able to build relationships with the staff, which made it easier and more effect to discuss our project with them. Unfortunetly we faced a lot more resistance from key stakeholders than expected. Although there was understanding of the problem, several barriers were raised to implementing a change in protocol. Although agreement was eventually reached, the process of contacting individual and arranging meetings was much more difficult and took a lot more time than expected, around 4-5 weeks. Through this time, however, a significant change was noted from our data collected. There was a huge increase of patients receiving a post-operative creatinine within 48 hours, in patients who discharged the day after their surgery as well as patients who remained in hospital for more than the day after their day of surgery. Study: how did the results of your test compare with predictions? An increase of postoperative creatinine measurements, from 38% in the baseline to an average of 98% over the 4 week period, was observed in patients who stayed 2 or more days beyond their day of surgery. patients who were discharged the day after their day of surgery also showed an improvement; from 0% to an average of 40%. We believe this is due to the “Hawthorn Effect”. Our presence on ward 9 and the staff being aware of what were doing, meant that they tried to improve the system themselves. This is a much greater improvement than we imagined when planning the test. The unpredicted difficulty in both getting in contact and arranging discussions with stakeholders as well as gaining approval and cooperation had a significant impact on the project as a whole. Although agreement and cooperation was eventually substantial enough to move the project on, successful implementation became less likely as we were coming to an end of the projects allocated time. This unexpected setback also had an effect on being able to include enthusiastic team members in the project. Although junior doctors, were identified, who seemed willing to play an active role, their placement on urology was also coming to an end and therefore would not be able to assist in the implementation of the change in protocol. BMJ Quality Improvement Programme PDSA Template Act: how will you change your previous test in light of what you have learned? Our next test is to attempt to implement a change in protocol with the time avaliable. Successive junior doctors will be engaged. Data will continue to be analysed to test whether the improvement has been sustainable. BMJ Quality Improvement Programme PDSA Template PDSA Cycle 3 Aim: what are you trying to accomplish? Increase the percentage of patients who return to ward 9 for one or more days after a urological surgery who receive a postoperative creatinine measurement. Specifically, we want the reliability of this measurement to be 95% by the end of our project 14 July 2014 Plan: what will your test be? A change in protocol will be implemented that all patients undergoing urological surgical procedures who stay in hospital for more than 1 day after their day of surgery receive a post-operative creatinine measurement. This will be implemented for 4-6 weeks to test whether an increased number of patients are found to have developed AKI. Prediction: what do you think will happen as a result of your test? 5. AKI will be found in a greater percentage of patients. 6. Some pressure may be put on the systems affected which will require additional changes. 7. The intervention may be delayed and/or passed on, as the project came to a close. Do: what happened when you carried out your test? Despite the approval and agreement from key stakeholders for the intervention, further delay in organisation of multidisciplinary meetings and mutual understanding was not achieved. This led to it not being possible in the time left to implement a formal change in protocol on ward 9. During this time, the improvement originally observed in the number of patients receiving a post-operative creatinine measurement decreased. BMJ Quality Improvement Programme PDSA Template Study: how did the results of your test compare with predictions? During the last 2 weeks of the project not only was our presence on ward 9 less, but there was also a change in junior doctors on the ward. This most likely explains the reduction in percentage patients receiving post-operative creatinine measurements. Unfortunetly the improvement we made through raising awareness was not sustainable. The time taken to engage with all important groups and individuals was underestimated, possibly due to resistance but also other commitments. Act: how will you change your previous test in light of what you have learned? Our assessment of patients undergoing urological surgical procedures in the pre-operative and post-operative setting will be taken up by various members we brought together in a hope to do the test for change in ward 9 and if it works attempt it on other wards where there may be a problem with AKI. There will also be continued advice provided on the test for change. BMJ Quality Improvement Programme PDSA Template