Heartworms in Dogs - South Anderson Veterinary Clinic
advertisement

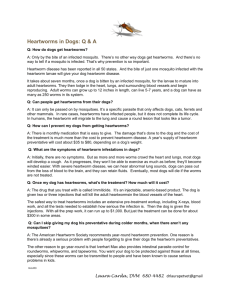
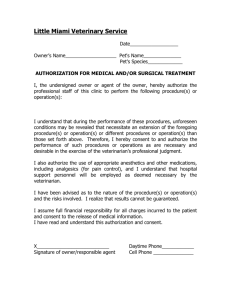
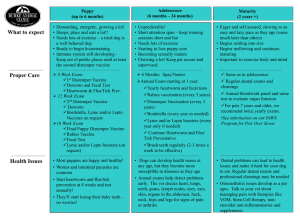
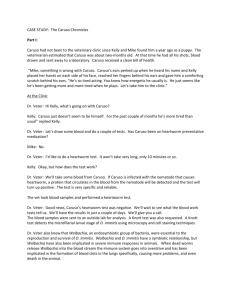
Heartworms in Dogs CAPC Recommendations: Heartworm (Dirofilaria immitis) Life Cycle and Stages Dog Life Cycle The heartworm life cycle is demonstrated in the figure below: Microfilariae reside in the blood of most, but not all, infected canids. L3 larvae (1,000 µm by 40 µm) are deposited on the skin during subsequent feeding and migrate through the bite wound into the host. Most L3 molt to L4 in subcutaneous tissue within 1 to 3 days after infection. L4 larvae migrate through tissues for several weeks. Juvenile worms (1 to 3 cm in length) enter the vascular system and are carried to the heart and pulmonary arteries, arriving as early as 70 days after infection. Final maturation to adult and mating occurs in the pulmonary vessels. Mature adults range in length from 15 to 18 cm (males) and from 25 to 30 cm (females). Canine hosts typically demonstrate microfilariae 6 to 7 months after infection. Microfilariae (307 to 322 µm by 6.8 to 7.0 µm) are ingested by feeding female mosquitoes. After two molts (approximately 2 weeks), infective L3 larvae are present in mosquito mouth parts. Development may require a longer period at cooler temperatures and ceases at temperatures below 57ºF. Development progresses in the mosquito relative to ambient temperature; if ambient temperature increases, development will resume. A final molt to the juvenile worm (sexually immature adult) occurs approximately 2 months (50 to 70 days) after infection www.SouthAndersonVet.com 109 W 53rd St * Anderson, IN 46013 * (765) 642-8117 * Fax: (765) 642-0519 Microfilariae ingested by feeding mosquitoes complete the life cycle. Heartworms live approximately 5 to 7 years in the dog. Disease Heartworm infection in the dog induces or may induce pulmonary endothelial damage, villous proliferation, and activation and attraction of leukocytes and platelets due to live worms as well as thrombosis, granulomatous, and villous inflammation due to dead and/or dying worms. Pulmonary vessels may become thickened and tortuous. Heartworm may induce glomerulonephritis and proteinuria secondary to antigen-antibody complexes. Rarely, ectopic infections of the eye, central nervous system, peritoneal cavity, systemic circulation, or skin have been reported. Caval syndrome has been reported. Associated findings include: pallor, weak pulses, tachycardia, and sudden collapse hemoglobinemia and hemoglobinuria disseminated intravascular coagulopathy (DIC) murmur caused by tricuspid regurgitation auscultated best on right side of thorax Cardiac output may be reduced. Pulmonary hypertension may lead to compensatory right heart enlargement and right heart failure. Clinical signs include cough, dyspnea, weight loss, ascites and jugular venous distension, exercise intolerance, and arrhythmias. In a small number of cases; worms may be found in the post cava and right atrium, causing interference of tricuspid valve function. This results in a peracute life-threatening hemolytic anemia and right heart failure. Prevalence Surveys indicate that heartworm infections continue to increase in numbers and geographic distribution. The American Heartworm Society conducted nationwide surveys of heartworm test results from veterinary clinics in calendar years 2001, 2004, and 2007. Results of these surveys indicated that heartworm infections now occur in areas where they were not previously recognized and some endemic areas are reporting higher numbers of heartworm-positive dogs. The greatest numbers of cases are seen in the southeastern U.S. and the Mississippi River Valley. www.SouthAndersonVet.com 109 W 53rd St * Anderson, IN 46013 * (765) 642-8117 * Fax: (765) 642-0519 Host Associations and Transmission Between Hosts Mosquito species capable of transmitting heartworm disease can be found in most geographical areas. More than 70 species of mosquitoes are capable of transmitting the disease. Transmission can occur anytime infected mosquitoes are active and feeding. Although the domestic dog is the primary host for heartworm, other species have been infected, including the following: o wild canidae, such as coyotes, wolves, foxes, etc. o ferrets o domestic cats o wild felidae, such as mountain lions, bobcats, tigers, etc. o marine mammals o humans Rare instances of transmission of microfilaria from infected bitches to fetuses via the placenta and from dog to dog via blood transfusion can occur. However, these microfilariae will not develop into adult worms. Presence of these microfilariae can confound a diagnosis and may serve as a potential source of microfilaria that could be transmitted by feeding mosquitoes. Prepatent Period and Environmental Factors Microfilariae appear in circulation 6 to 7 months after introduction of infective larvae (L3). Infection and successful development of heartworm larvae in mosquitoes is dependent on mosquito feeding habits, mosquito longevity, and ambient temperatures. Diagnosis Heartworm infection and/or disease is confirmed or ruled out using laboratory tests, radiography, echocardiography, and/or electrocardiography. These tests may also be used to identify appropriate therapies, monitor the course of the infection or disease, and determine the success of any treatment. Laboratory tests o Serological testing Antigen tests Antigen tests detect a glycoprotein found predominantly in the reproductive tract of the female worm. Only mature infections (older than 6 months) with at least one female worm are detected. Low worm burdens (fewer than two adult females) may not be detected. A number of commercial antigen tests are available. Formats include well enzyme-linked immunosorbent assay (ELISA) tests, solid substratum ELISA tests, and immunochromatograhic (immunomigratory) tests. Due to high specificity (98 to 100%) of the available tests, it is better to accept than reject a positive test result. Because no test is 100% accurate, it is prudent to repeat a positive test in animals from hypoendemic areas or animals on preventives. Similarly, a negative test in an animal exhibiting clinical signs of heartworm disease should be repeated. Repeat tests should be submitted to a reference laboratory. Clinical pathological parameters Abnormal clinical pathology results are not uniquely diagnostic for heartworms. www.SouthAndersonVet.com 109 W 53rd St * Anderson, IN 46013 * (765) 642-8117 * Fax: (765) 642-0519 Hematological changes associated with heartworm infection include eosinophilia, basophilia, neutrophilia, nonregenerative anemia, and thrombocytopenia. Chemical results may show elevated liver enzymes, azotemia, and hyperbilirubinemia. Urinalysis may indicate proteinuria and albuminuria. Detection of microfilaria Microfilariae are not present in all heartworm-infected dogs. Dogs may be microfilariae negative (“occult”) for several reasons: single sex adult infections frequent elimination of microfilaria by preventives host immune responses presence of antigen prior to microfilariae production. (In rare cases, the appearance of microfilariae may precede antigenemia.) Microfilariae may be identified microscopically by several methods: direct examination of fresh blood or blood treated with an anticoagulant examination of liquid-cell interface (buffy coat) in a microhematocrit tube concentration using a stained or unstained millipore filter concentration by centrifugation using the modified Knott procedure Microfilariae of D. immitis must be differentiated from those of Acanthocheilonema reconditum. The following table compares characteristics of the two species; these guidelines are useful only with fresh blood samples. o Number in blood Motion Shape Length (modified Knott test) Acanthocheilonema reconditum Usually few Progressive Curved body, blunt head, curved or “button-hook” tail 250 to 288 µm Dirofilaria immitis Usually many Stationary Straight body and 307 to 322 µm tail, tapered head Microfilariae of D. immitis (bottom) and A. (Dipetalonema) reconditum o Radiography Radiographic evidence of heartworm infections consists of increased size of pulmonary arteries, increased arterial tortuosity, and pruning. Right-sided cardiomegaly gives the heart the shape of a reverse “D.” www.SouthAndersonVet.com 109 W 53rd St * Anderson, IN 46013 * (765) 642-8117 * Fax: (765) 642-0519 Pulmonary parenchyma should be evaluated for infiltrates and nodules. Additional radiographic findings may include lymphadenopathy and pleural effusion. Radiographic lesions are more pronounced in the caudal lung lobes Treatment The goals of treatment are to address the clinical condition of the animal and eliminate adult heartworms and microfilariae. Stabilize the animal with clinical heartworm disease. Any or all of the following may be medically indicated: o corticosteroid therapy o fluid therapy o diuretics o vasodilators o positive inotropic agents Many clinicians recommend starting the animal on macrocyclic lactone (preventive) at time of diagnosis or keeping on macrocyclic lactone if it is already being administered. Administration of macrocylcic lactone as a heartworm preventive is an extra-label use of this product. Remove adult worms. o Melarsomine dihydrochloride (2.5 mg/kg) can be administered intramuscularly once, followed in 1 month (or longer if the dog’s condition dictates) by two intramuscular injections (2.5 mg/kg) 24 hours apart. Any excitement or exercise beyond slow walking for bathroom breaks should be restricted for at least 1 month following each set of injections. This option eliminates 98% of the worm burden and is the treatment of choice. o Melarsomine dihydrochloride (2.5 mg/kg) can be administered intramuscularly twice over a 24-hour period, followed by at least 1 month of strict exercise restriction. This option eliminates only 90% of the worm burden. o Melarsomine is not proven effective against heartworms younger than 4 months of age. Dogs may be infected with heartworms of various ages. For this reason, www.SouthAndersonVet.com 109 W 53rd St * Anderson, IN 46013 * (765) 642-8117 * Fax: (765) 642-0519 o o treatment may not be completely effective in all situations. This may necessitate additional therapy or alternate therapeutic strategies. Adulticidal therapy using long-term macrocyclic lactone administration is not recommended for the following reasons: Published efficacy has been confirmed only against worms 8 months old or younger. Long-term presence of worms continues to induce pulmonary vascular disease. Exercise during long-term therapy has resulted in increased severity of pulmonary radiographic lesions in 30% of cases. Presence of microfilariae has continued for a year or longer in approximately 20% of dogs with patent heartworm infections placed on monthly preventive therapy. These microfilariae are living after exposure to the drug in the bloodstream or within the uterus of the female worm. It should be noted that long-term continuous administration of heartworm preventives generally is not a substitute for conventional arsenical adulticide treatment. If arsenical therapy is declined (i.e., because of cost, geriatric patient, concurrent disease), a lengthy course of prophylactic doses of a macrocyclic lactone will gradually reduce the number of adult heartworms. However, in chronic mature infections, this may not be clinically beneficial. Exercise should be restricted in dogs treated with prophylactic doses of macrocyclic lactones as the adulticide. (Information excerpted from the American Heartworm Society guidelines with some modifications.) Microfilaricidal treatment If present, circulating microfilariae are eliminated with macrocyclic lactone therapy. All products have some microfilaricidal effects at standard labeled doses; however, complete clearance can take 9 to12 months. More rapid clearance can be achieved with: ivermectin at 50 µg/kg milbemycin oxime at 500 ug/kg When this method is employed, it may be necessary to observe a patient with very high microfilaremia , e.g., > 10/hpf (high power field microscopy), for potential adverse reaction or pretreat the animal with steroids and/or antihistamines. Test 6 months after melarsomine therapy with an antigen test to determine if infection has been cleared. Exercise restriction should continue for 1 to 3 months following adulticidal therapy. Additional considerations for adulticide therapy o Wolbachia Most filarial nematodes, including D. immitis, harbor obligate, intracellular, gram-negative bacteria belonging to the genus Wolbachia (Rickettsiales). It is hypothesized that Wolbachia contribute to pulmonary and renal inflammation through the Wolbachia surface protein (WSP), independent of the endotoxin component. A recent study suggests that suppressing Wolbachia populations with doxycycline prior to adulticide therapy may reduce the gross pulmonary pathology that occurs as a result of thromboembolic shower of dead worm fragments. Control and Prevention Heartworm infection can be easily prevented with a number of macrocyclic lactone preventives. www.SouthAndersonVet.com 109 W 53rd St * Anderson, IN 46013 * (765) 642-8117 * Fax: (765) 642-0519 These preventives vary in their claims against other internal and external parasites and are available in different formulations (tablets, chewable tablets, flavored tablets, and topical and injectable preparations). Macrocyclic lactone preventives currently available include: o ivermectin o milbemycin oxime o moxidectin o selamectin Public Health Considerations Dirofilaria immitis is of public health concern even though the number of reported cases is not large. More than 100 human cases of pulmonary dirofilariasis have been reported in the United States in last fifty years. Infections have also been recorded in the eye, skin, testicle, and elsewhere. Prevention is best accomplished through mosquito abatement programs and by using mosquito repellents, wearing protective clothing, and remaining indoors during mosquito feeding periods. Human dirofilariasis results in nodular inflammation of the lungs. o Pulmonary nodules are usually solitary and form around dead immature heartworms. o Nodules are often mistaken for lung tumors or tuberculosis, resulting in unnecessary surgery. www.SouthAndersonVet.com 109 W 53rd St * Anderson, IN 46013 * (765) 642-8117 * Fax: (765) 642-0519