Ministry of Education and Science of Ukraine
Sumy State University
3727 LEANER’S GUIDE
in Medical Terminology
for Full-Time Students
Speciality 7.110101
Term 4
Sumy
Sumy State University
2014
Learner’s Guide in Medical Terminology for Full-Time
Students, Speciality 7.110101, Term 4/ compilers: I. M. Terletska,
V. S. Kurochkina, N. G. Gorobchenko. – Sumy: Sumy State
University, 2014. – 115 p.
The Department of Foreign Languages
CONTENTS
P.
UNIT 1 ................................................................................................................ 4
UNIT 2 ................................................................................................................ 7
UNIT 3 .............................................................................................................. 12
UNIT 4 .............................................................................................................. 16
UNIT 5 .............................................................................................................. 20
UNIT 6 .............................................................................................................. 25
UNIT 7 .............................................................................................................. 29
UNIT 8 .............................................................................................................. 33
UNIT 9 .............................................................................................................. 38
UNIT 10 ............................................................................................................ 43
UNIT 11 ............................................................................................................ 48
UNIT 12 ............................................................................................................ 51
UNIT 13 ............................................................................................................ 55
UNIT 14 ............................................................................................................ 61
UNIT 15 ............................................................................................................ 66
UNIT 16 ............................................................................................................ 73
UNIT 17 ............................................................................................................ 87
UNIT 18 ............................................................................................................ 97
UNIT 19 .......................................................................................................... 105
UNIT 20 .......................................................................................................... 109
REFERENCES ............................................................................................... 114
Unit 1
Pre-text assignment
Learn the key words and phrases:
Kidney, metabolic wastes, ureters, urinary bladder, ureterovesical
valves, sac-like hollow organ, urethra, urea.
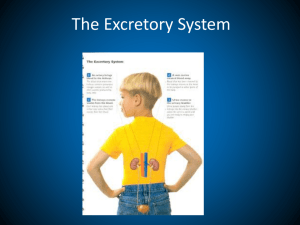
Urinary System Anatomy
Kidneys
The kidneys are a pair of bean-shaped organs found along the
posterior wall of the abdominal cavity. The left kidney is located
slightly higher than the right kidney because the right side of
the liver is much larger than the left side. The kidneys, unlike the
other organs of the abdominal cavity, are located posterior to the
peritoneum and touch the muscles of the back. The kidneys are
surrounded by a layer of adipose that holds them in place and
protects them from physical damage. The kidneys filter metabolic
wastes, excess ions, and chemicals from the blood to form urine.
Ureters
The ureters are a pair of tubes that carry urine from the kidneys to
the urinary bladder. The ureters are about 10 to 12 inches long and
run on the left and right sides of the body parallel to the vertebral
column. Gravity and peristalsis of smooth muscle tissue in the walls
of the ureters move urine toward the urinary bladder. The ends of the
ureters extend slightly into the urinary bladder and are sealed at the
point of entry to the bladder by the ureterovesical valves. These
valves prevent urine from flowing back towards the kidneys.
Urinary Bladder
The urinary bladder is a sac-like hollow organ used for the storage
of urine. The urinary bladder is located along the body’s midline at
the inferior end of the pelvis. Urine entering the urinary bladder from
the ureters slowly fills the hollow space of the bladder and stretches
its elastic walls. The walls of the bladder allow it to stretch to hold
anywhere from 600 to 800 milliliters of urine.
Urethra
The urethra is the tube through which urine passes from the
bladder to the exterior of the body. The female urethra is around 2
inches long and ends inferior to the clitoris and superior to the
vaginal opening. In males, the urethra is around 8 to 10 inches long
and ends at the tip of the penis. The urethra is also an organ of the
male reproductive system as it carries sperm out of the body through
the penis.
The flow of urine through the urethra is controlled by the internal
and external urethral sphincter muscles. The internal urethral
sphincter is made of smooth muscle and opens involuntarily when the
bladder reaches a certain set level of distention. The opening of the
internal sphincter results in the sensation of needing to urinate. The
external urethral sphincter is made of skeletal muscle and may be
opened to allow urine to pass through the urethra or may be held
closed to delay urination.
How do the kidneys and urinary system work?
The kidney and urinary systems keep chemicals, such as
potassium and sodium, and water in balance and remove a type of
waste, called urea, from the blood. Urea is produced when foods
containing protein, such as meat, poultry, and certain vegetables, are
broken down in the body. Urea is carried in the bloodstream to the
kidneys, where it is removed.
Other important functions of the kidneys include blood
pressure regulation and the production of erythropoietin, which
controls red blood cell production in the bone marrow.
Two ureters - narrow tubes that carry urine from the kidneys
to the bladder. Muscles in the ureter walls continually tighten and
relax forcing urine downward, away from the kidneys. If urine backs
up, or is allowed to stand still, a kidney infection can develop. About
every 10 to 15 seconds, small amounts of urine are emptied into the
bladder from the ureters.
Bladder – a triangle-shaped, hollow organ located in the lower
abdomen. It is held in place by ligaments that are attached to other
organs and the pelvic bones. The bladder's walls relax and expand to
store urine, and contract and flatten to empty urine through the
urethra. The typical healthy adult bladder can store up to two cups of
urine for two to five hours.
Two sphincter muscles - circular muscles that help keep urine
from leaking by closing tightly like a rubber band around the opening
of the bladder.
Nerves in the bladder - alert a person when it is time to
urinate, or empty the bladder.
Urethra - the tube that allows urine to pass outside the body.
The brain signals the bladder muscles to tighten, which squeezes
urine out of the bladder. At the same time, the brain signals the
sphincter muscles to relax to let urine exit the bladder through the
urethra. When all the signals occur in the correct order, normal
urination occurs.
Facts about urine:
Adults pass about a quart and a half of urine each day,
depending on the fluids and foods consumed.
The volume of urine formed at night is about half that formed
in the daytime.
Normal urine is sterile. It contains fluids, salts and waste
products, but it is free of bacteria, viruses and fungi.
The tissues of the bladder are isolated from urine and toxic
substances by a coating that discourages bacteria from attaching and
growing on the bladder wall.
Post-text assignments
1 Match the definition of the part of the urinary system in
column I with the name of the organ in column II:
I
II
1 These organs are about 10
to 12 inches long and run on
the left and right sides of the
body parallel to the vertebral
a) kidney
column.
2 Tube-formed organ
b) ureters
through which urine passes
from the bladder to the
exterior of the body.
3 A pair of bean-shaped
organs found along the
posterior wall of the
abdominal cavity.
4 A sac-like hollow organ
used for the storage of urine.
c) urinary bladder
d) urethra
2 Answer the questions
1 What parts does urinary system consist of?
2 What kind of tissue are kidneys surrounded with?
3 Where is the urinary bladder located?
4 When does a kidney infection can develop?
5 What is the length of ureters?
6 What muscles control the flow of urine through the urethra?
7 When is urea produced?
8 How often is small amount of urine emptied into the bladder
from the ureters?
9 How much urine can the typical healthy adult bladder store?
10 What is the difference between male and female urethra?
Unit 2
Pre-text assignment
Learn the key words and phrases:
conserve, excretion, elimination, pH buffers, glomerulus
Urinary System Physiology
Maintenance of Homeostasis
The kidneys maintain the homeostasis of several important
internal conditions by controlling the excretion of substances out of
the body.
Ions. The kidney can control the excretion of potassium, sodium,
calcium, magnesium, phosphate, and chloride ions into urine. In
cases where these ions reach a higher than normal concentration, the
kidneys can increase their excretion out of the body to return them to
a normal level. Conversely, the kidneys can conserve these ions when
they are present in lower than normal levels by allowing the ions to
be reabsorbed into the blood during filtration.
pH. The kidneys monitor and regulate the levels of hydrogen ions
(H+) and bicarbonate ions in the blood to control blood pH. H+ ions
are produced as a natural byproduct of the metabolism of dietary
proteins and accumulate in the blood over time. The kidneys excrete
excess H+ ions into urine for elimination from the body. The kidneys
also conserve bicarbonate ions, which act as important pH buffers in
the
blood.
Osmolarity. The cells of the body need to grow in an isotonic
environment in order to maintain their fluid and electrolyte balance.
The kidneys maintain the body’s osmotic balance by controlling the
amount of water that is filtered out of the blood and excreted into
urine. When a person consumes a large amount of water, the kidneys
reduce their reabsorption of water to allow the excess water to be
excreted in urine. This results in the production of dilute, watery
urine. In the case of the body being dehydrated, the kidneys reabsorb
as much water as possible back into the blood to produce highly
concentrated urine full of excreted ions and wastes. The changes in
excretion of water are controlled by antidiuretic hormone (ADH).
ADH is produced in the hypothalamus and released by the
posterior pituitary gland to help the body retain water.
Blood Pressure. The kidneys monitor the body’s blood pressure to
help maintain homeostasis. When blood pressure is elevated, the
kidneys can help to reduce blood pressure by reducing the volume of
blood in the body. The kidneys are able to reduce blood volume by
reducing the reabsorption of water into the blood and producing
watery, dilute urine. When blood pressure becomes too low, the
kidneys can produce the enzyme renin to constrict blood vessels and
produce concentrated urine, which allows more water to remain in
the blood.
Filtration
Inside each kidney are around a million tiny structures called
nephrons. The nephron is the functional unit of the kidney that filters
blood to produce urine. Arterioles in the kidneys deliver blood to a
bundle of capillaries surrounded by a capsule called a glomerulus. As
blood flows through the glomerulus, much of the blood’s plasma is
pushed out of the capillaries and into the capsule, leaving the blood
cells and a small amount of plasma to continue flowing through the
capillaries. The liquid filtrate in the capsule flows through a series of
tubules lined with filtering cells and surrounded by capillaries. The
cells surrounding the tubules selectively absorb water and substances
from the filtrate in the tubule and return it to the blood in the
capillaries. At the same time, waste products present in the blood are
secreted into the filtrate. By the end of this process, the filtrate in the
tubule has become urine containing only water, waste products, and
excess ions. The blood exiting the capillaries has reabsorbed all of
the nutrients along with most of the water and ions that the body
needs to function.
Storage and Excretion of Wastes
After urine has been produced by the kidneys, it is transported
through the ureters to the urinary bladder. The urinary bladder fills
with urine and stores it until the body is ready for its excretion. When
the volume of the urinary bladder reaches anywhere from 150 to 400
milliliters, its walls begin to stretch and stretch receptors in its walls
send signals to the brain and spinal cord. These signals result in the
relaxation of the involuntary internal urethral sphincter and the
sensation of needing to urinate. Urination may be delayed as long as
the bladder does not exceed its maximum volume, but increasing
nerve signals lead to greater discomfort and desire to urinate.
Urination is the process of releasing urine from the urinary bladder
through the urethra and out of the body. The process of urination
begins when the muscles of the urethral sphincters relax, allowing
urine to pass through the urethra. At the same time that the sphincters
relax, the smooth muscle in the walls of the urinary bladder contract
to expel urine from the bladder.
Production of Hormones
The kidneys produce and interact with several hormones that are
involved in the control of systems outside of the urinary system.
Calcitriol. Calcitriol is the active form of vitamin D in the human
body. It is produced by the kidneys from precursor molecules
produced by UV radiation striking the skin. Calcitriol works together
with parathyroid hormone (PTH) to raise the level of calcium ions in
the bloodstream. When the level of calcium ions in the blood drops
below a threshold level, the parathyroid glands release PTH, which in
turn stimulates the kidneys to release calcitriol. Calcitriol promotes
the small intestine to absorb calcium from food and deposit it into the
bloodstream. It also stimulates the osteoclasts of the skeletal system
to break down bone matrix to release calcium ions into the blood.
Erythropoietin. Erythropoietin, also known as EPO, is a hormone
that is produced by the kidneys to stimulate the production of red
blood cells. The kidneys monitor the condition of the blood that
passes through their capillaries, including the oxygen-carrying
capacity of the blood. When the blood becomes hypoxic, meaning
that it is carrying deficient levels of oxygen, cells lining the
capillaries begin producing EPO and release it into the bloodstream.
EPO travels through the blood to the red bone marrow, where it
stimulates hematopoietic cells to increase their rate of red blood cell
production. Red blood cells contain hemoglobin, which greatly
increases the blood’s oxygen-carrying capacity and effectively ends
the
hypoxic
conditions.
Renin. Renin is not a hormone itself, but an enzyme that the
kidneys produce to start the renin-angiotensin system (RAS). The
RAS increases blood volume and blood pressure in response to low
blood pressure, blood loss, or dehydration. Renin is released into the
blood where it catalyzes angiotensinogen from the liver into
angiotensin I. Angiotensin I is further catalyzed by another enzyme
into Angiotensin II.
Angiotensin II stimulates several processes, including stimulating
the adrenal cortex to produce the hormone aldosterone. Aldosterone
then changes the function of the kidneys to increase the reabsorption
of water and sodium ions into the blood, increasing blood volume
and raising blood pressure. Negative feedback from increased blood
pressure finally turns off the RAS to maintain healthy blood pressure
levels.
Post-text assignments
1 Answer the questions:
1 What kind of hormones do kidneys produce?
2 When does the process of urination begin?
3 What kind of ions do kidneys also conserve?
4 Which parts does nephron consist of?
5 How do the kidneys maintain the body’s osmotic balance?
6 What is the role of calcitriol in our organism?
7 Which processes does Angiotensin II stimulate?
8 What is erythropoietin produced for?
2 Look at the statements ad say whether they are true or false:
1 The kidneys also conserve dihydrate ions, which act as
important pH buffers in the blood.
2 The kidneys maintain the body’s osmotic balance by
controlling the amount of water that is filtered out of the blood and
excreted into urine.
3 When blood pressure is reduced, the kidneys can help to
elevate blood pressure by reducing the volume of blood in the body.
4 When blood pressure becomes too low, the kidneys can
produce the enzyme calcitriol to constrict blood vessels and produce
concentrated urine, which allows more water to remain in the blood.
5 Inside each kidney are around a million tiny structures called
osteons.
6 Renin is the active form of vitamin D in the human body.
7 When the level of calcium ions in the blood drops below a
threshold level, the parathyroid glands release PTH, which in turn
stimulates the kidneys to release calcitriol.
8 The blood exiting the capillaries has reabsorbed all of the
nutrients along with most of the water and ions that the body needs to
function.
9 Urination is the process of releasing urine from the
gallbladder through the ureters and out of the body.
10 The kidneys monitor the condition of the blood that passes
through their capillaries, including the oxygen-carrying capacity of
the blood.
Unit 3
Pre-text assignment
1 Learn the key words and phrases:
metabolic waste matter, kidney colic, oedema, dialysis.
2 Translate the following:
1 Stones can partly block the flow of urine and this may result
in infections as well as accumulation of waste matter in the blood.
2 If the condition continues to deteriorate, uraemia or renal
failure develops.
3 The conventional medical treatment is the removal of these
waste materials by filtering the blood through an external membrane,
a dialysis machine or artificial kidney.
4 The disadvantages and dangers are that dialysis takes a long
time; 4 - 12 hours twice a week, and beneficial ingredients, such as
zinc may be lowered while harmful ones, such as aluminium may
accumulate.
5 With a severe restriction of protein and phosphate intake, tests
showed a 10 to 40 fold decrease in the progression of kidney disease
and patients who would normally have required immediate
commencement of dialysis could postpone this for about seven
months.
6 A high protein and phosphate intake imposes a greatly
increased workload on the kidneys.
Kidney Disease
The main functions of the kidneys are the removal of metabolic
waste matter, of any toxic material and excess of water, minerals, and
bio-chemicals in order to keep their blood levels within on optimal
range. This is done by filtering the blood and concentrating the waste
in the form of urine. In addition, the kidneys produce hormones,
which affect the salt balance and red blood cell production.
A common kidney disorder is the formation of kidney stones.
These are mostly composed of calcium salts and to a lesser degree of
uric acid. Stones can partly block the flow of urine and this may
result in infections as well as accumulation of waste matter in the
blood. The passing of large stones through the urethra can be
extremely painful and is called kidney colic.
Stone formation as well as bacterial infections or accumulation of
toxic material may lead to acute or chronic inflammation of the
kidneys, also called nephritis or Bright's disease. Symptoms are a rise
in blood pressure, back pain, fatigue, being listless and loss of
appetite. Later oedema may develop; one may feel dizzy and
nauseated. Albumin, a protein compound, will be passed in
increasing quantities with the urine.
If the condition continues to deteriorate, uraemia or renal failure
develops. High concentrations of waste matter accumulate in the
blood and all of the mentioned symptoms become more severe. If
nothing is done about it, death will eventually occur. The
conventional medical treatment is the removal of these waste
materials by filtering the blood through an external membrane, a
dialysis machine or artificial kidney. When the condition deteriorates
still further, a kidney transplant is attempted.
The disadvantages and dangers are that dialysis takes a long time;
4 - 12 hours twice a week, and beneficial ingredients, such as zinc
may be lowered while harmful ones, such as aluminium may
accumulate. Kidney transplants have the major disadvantage, apart
from the risk of the operation itself, that the lifelong requirement to
take immune-suppressive drugs weakens the immune system and
predisposes to chronic and severe infections as well as cancer.
Nephritis or Bright's Disease
Further important nutritional factors in the development of kidney
disease are a high intake of protein, phosphate and calcium, a low
intake of magnesium and vitamin B6, and finally, chronic
inflammation due to food allergy.
Proteins are generally high in phosphorus. Therefore, by
restricting the protein intake the amount of phosphate ingested or
formed in the body is reduced at the same time. With a severe
restriction of protein and phosphate intake, tests showed a 10 to 40
fold decrease in the progression of kidney disease and patients who
would normally have required immediate commencement of dialysis
could postpone this for about seven months.
A high protein and phosphate intake imposes a greatly increased
workload on the kidneys. If their functions are already impaired by
stone formation or inflammation, then the individual filtering units
become more and more sclerotic, which means they calcify and
harden through overgrowth with tough, fibrous tissue. This causes
large amounts of protein to be lost with the urine while other
chemicals, such as salt and uric acid remain in the body.
High phosphate levels also cause an overactivity of the
parathyroid glands with a resultant rise in calcium blood levels. This
may lead to decalcification of bones and to the formation of calcium
deposits as with kidney stones, arteriosclerosis and arthritic
deformations. It raises the blood pressure and damages the kidneys
still further, in particular through calcification of the kidneys with
calcium phosphate.
In addition to a high phosphate intake, a diet high in protein
produces much more waste products than any other class of nutrients,
especially in the form of urea, uric acid and sulphates. Compared to
proteins there is hardly any residue in a properly metabolised
carbohydrate or fat diet. Both produce carbon dioxide and water as
end products. Therefore, with these foods there is hardly any need for
dialysis.
Patients with severe renal failure should restrict their protein
intake to less than 20 g and phosphorus to less than 400 mg. For
children and as a maintenance diet amino acid supplements may be
necessary with severe protein restrictions.
Post-text assignments
1 Describe the symptoms of the Nephritis or Bright's Disease.
What other kidney disease do you know?
2 Complete the following sentences
1 The main functions of the kidneys are…
2 Stone formation as well as bacterial infections or
accumulation of toxic material may lead to…
3 The conventional medical treatment is…
4 Further important nutritional factors in the development of
kidney disease are…
5 Kidney transplants have the major disadvantage…
6 Patients with severe renal failure should…
Unit 4
Pre-text assignment
Learn the key words and phrases:
tuberculosis, waste away, consumption, multiple medications, spit,
unpasteurized milk, susceptibility, coughing up of sputum,
resurgence.
Tuberculosis
What is tuberculosis?
Tuberculosis (TB) is an infectious disease caused by bacteria
whose scientific name is Mycobacterium tuberculosis. It was first
isolated in 1882 by a German physician named Robert Koch who
received the Nobel Prize for this discovery. TB most commonly
affects the lungs but also can involve almost any organ of the body.
Many years ago, this disease was referred to as "consumption"
because without effective treatment, these patients often would waste
away. Today, of course, tuberculosis usually can be treated
successfully with antibiotics.
There is also a group of organisms referred to as atypical
tuberculosis. These involve other types of bacteria that are in the
Mycobacterium family. Often, these organisms do not cause disease
and are referred to as "colonizers" because they simply live alongside
other bacteria in our bodies without causing damage. At times, these
bacteria can cause an infection that is sometimes clinically like
typical tuberculosis. When these atypical mycobacteria cause
infection, they are often very difficult to cure. Often, drug therapy for
these organisms must be administered for one and a half to two years
and requires multiple medications.
How does a person get TB?
A person can become infected with tuberculosis bacteria when he
or she inhales minute particles of infected sputum from the air. The
bacteria get into the air when someone who has a tuberculosis lung
infection coughs, sneezes, shouts, or spits (which is common in some
cultures). People who are nearby can then possibly breathe the
bacteria into their lungs. You don't get TB by just touching the
clothes or shaking the hands of someone who is infected.
Tuberculosis is spread (transmitted) primarily from person to person
by breathing infected air during close contact.
There is a form of atypical tuberculosis, however, that is
transmitted by drinking unpasteurized milk. Related bacteria, called
Mycobacterium bovis, cause this form of TB. Previously, this type of
bacteria was a major cause of TB in children, but it rarely causes TB
now since most milk is pasteurized (undergoes a heating process that
kills the bacteria).
How common is TB, and who gets it?
Over 8 million new cases of TB occur each year worldwide. In the
United States, it is estimated that 10-15 million people are infected
with the TB bacteria, and 22,000 new cases of TB occur each year.
Anyone can get TB, but certain people are at higher risk, including
people who live with individuals who have an active TB
infection,
poor or homeless people,
foreign-born people from countries that have a high
prevalence of TB,
nursing-home residents and prison inmates,
alcoholics and intravenous drug users,
people with diabetes, certain cancers, and HIV infection (the
AIDS virus),
health-care workers.
There is no strong evidence for a genetically determined
(inherited) susceptibility for TB.
What are the symptoms and signs of tuberculosis?
As previously mentioned, TB infection usually occurs initially in
the upper part (lobe) of the lungs. The body's immune system,
however, can stop the bacteria from continuing to reproduce. Thus,
the immune system can make the lung infection inactive (dormant).
On the other hand, if the body's immune system cannot contain the
TB bacteria, the bacteria will reproduce (become active or reactivate)
in the lungs and spread elsewhere in the body.
It may take many months from the time the infection initially gets
into the lungs until symptoms develop. The usual symptoms that
occur with an active TB infection are a generalized tiredness or
weakness, weight loss, fever, and night sweats. If the infection in the
lung worsens, then further symptoms can include coughing, chest
pain, coughing up of sputum (material from the lungs) and/or blood,
and shortness of breath. If the infection spreads beyond the lungs, the
symptoms will depend upon the organs involved.
What's in the future for TB?
Conceivably, TB could have been eliminated by effective
treatment, vaccinations, and public-health measures by the year 2000.
However, the emergence of HIV changed the whole picture. Because
of HIV, a tremendous increase in the frequency (incidence) of TB
occurred in the '80s and throughout the '90s. This increase in TB
happened because suppression of the body's immune (defense)
system by HIV allowed TB to occur as a so-called opportunistic
infection.
With the increasing HIV epidemic in Africa, serious concerns are
being raised about the development of MDR-TB and XDR-TB in this
population. Hopefully, control of HIV in the future will check this
resurgence of tuberculosis.
The epidemic of HIV and TB has been a deadly combination
especially on the African continent. A recent study comparing
prophylactic regimens for prevention of active TB in HIV-infected
individuals has shown effectiveness, however, the distribution of
medication for both of this disease in the third world remains
problematic.
Post-text assignments
1 Answer the questions:
1 Who discovered Mycobacterium tuberculosis?
2 What kinds of people are at higher risk of getting TB?
3 How can a person become infected with tuberculosis bacteria?
4 What are the usual symptoms that occur with an active TB
infection?
5 Where does TB infection usually occur?
6 How many new cases of TB do occur each year worldwide?
7 What will happen if the body's immune system cannot contain
the TB bacteria?
8 What are the symptoms of TB if the infection in the lung
worsens?
2 Respond to the following tasks:
1 Describe how a person can become infected with tuberculosis
bacteria.
2 Describe the symptoms of TB infection.
3 Explain how the emergence of HIV increased the level of
tuberculosis.
4 List people who are at higher risk of getting TB.
Unit 5
Pre-text assignment
Learn the key words and phrases:
control and prevention, smallpox, poliomyelitis, miasmas,
chemotherapy, implementation, haemorrhagic fevers, nipah virus.
Infectious diseases – past, present, and future
In 1962 Sir McFarland Burnett stated, “By the end of the Second
World War it was possible to say that almost all of the major
practical problems of dealing with infectious disease had been
solved”. At that time, his statement was logical. Control and
prevention measures had decreased the incidence of many infectious
diseases, and with the ability to continue to identify new antibiotics,
to handle new problems, and the ongoing development of appropriate
vaccines, his statement appeared to be appropriate.
The history of the world is intertwined with the impact that
infectious diseases have had on populations. Evidence of smallpox
has been found in 3000-year-old Egyptian mummies. Egyptian
papyrus paintings depict infectious diseases such as poliomyelitis.
Hippocrates wrote about the spread of disease by means of airs,
water, and places, and made an association between climate, diet, and
living conditions. Investigators described miasmas as the source of
infections. Fracastoro discussed the germ theory in the 1500s and
three routes of contagion were proposed—direct contact, fomites, and
contagion from a distance (airborne). Epidemics of leprosy, plague,
syphilis, smallpox, cholera, yellow fever, typhoid fever, and other
infectious diseases were the norm.
The development of the microscope by Leeuwenhoek in the 1600s
allowed scientists to visualize microorganisms for the first time. The
1800s brought knowledge of the cultivation and identification of
micro-organisms. Vaccines were developed and used which
introduced specific methods to our storehouse of measures for control
and prevention. Pasteurization was another important contribution to
disease control. An appreciation of the environment and its
relationship to infectious diseases resulted in implementation of
broad control measures such as community sanitation, personal
hygiene, and public health education. The importance of nutrition
was appreciated for its impact on infectious diseases.
The 20th century brought chemotherapy and antibiotics into our
infectious disease armamentarium. Greater dependency upon
vaccination programmes and health education became important
allies in our efforts at reducing the occurrence of infectious disease.
So Sir McFarland’s statement was not an off hand remark.
But we are now aware that emerging and re-emerging infections
have become a significant worldwide problem. In 1991, the Institute
of Medicine of the National Research Council in the US appointed a
19-member multidisciplinary expert committee to study the
emergence of microbial threats to health. Their report published in
1992 was entitled, ‘Emerging Infections —Microbial Threats to
Health in the United States’ but the concepts that they discussed
certainly have worldwide application. They concluded that six
categories of factors could explain the emergence or re-emergence of
infectious diseases. These factors are: Human demographics and
behavior; Technology and industry; Economic development and land
use; International travel and commerce; Microbial adaptation and
change; and Breakdown of public health measures.
There have been other groupings of causative factors proposed
related to re-emerging infections and in some instances we do not yet
have a clue as to how new agents have appeared in animal and human
populations. The problem of emerging infections is well exemplified
by the many examples of new and emerging infectious diseases that
have impacted upon localized populations and/or geographical areas
over the past several decades. Human immunodeficiency virus
(HIV)/AIDS, first identified in 1981, portrays the significant impact
that an infectious disease can have on the world. Presently HIV/AIDS
is the fourth leading cause of death in the world and it remains the
leading cause of death in Africa. The economic havoc it has created
worldwide is frightening and its impact upon all peoples will remain
embedded on mankind for decades. More geographically localized,
but still creating worldwide concern, have been the haemorrhagic
fevers, Nipah virus, and monkeypox. And more recently sudden
acute respiratory syndrome (SARS) exemplifies how the occurrence
of a new and dangerous infectious disease can monopolize
governmental activities, cause fear and hysteria, have a significant
impact on the economy throughout the world and on the freedom of
movement of people.
We are bold in our attempts to control infectious diseases. We
have eradicated one disease (smallpox) and two other diseases are in
the final stages of eradication (poliomyelitis and dracunculiasis).
These eradication programmes demonstrate how international
collaboration and co-operation can significantly benefit the world.
However, our goals must be realistic, that is, initiation of an
eradication programme must be limited to the few diseases for which
this is a valid goal. Control and prevention should be our main
emphasis as we plan our ongoing commitment in our approach to
infectious diseases.
The events of the last several decades demonstrate that our
infectious disease guard cannot be reduced. We are making progress
in controlling and preventing infectious diseases but we must not
become complacent. The infectious disease papers in this edition of
the Journal amply portray the continuing impact that infectious
disease has on the world. They also demonstrate how new research
can be important in defining new methods of control and prevention.
As we focus on the problems of emerging and re-emerging
infectious diseases, we must not underplay other diseases and health
conditions that also significantly impact on all of us. With finite
limits on our resources for disease control and prevention, we must
learn how to better use these resources. Better planning, more
attention to training, improved efficiency, and strengthening the
collaboration and co-operation between countries will help in our
efforts to reduce the burden of disease.
Post-text assignments
1 Look at the statements ad say whether they are true or false:
1 Evidence of smallpox has been found in 3000-year-old
Chinese mummies.
2 The 1700s brought knowledge of the cultivation and
identification of micro-organisms.
3 An appreciation of the environment and its relationship to
infectious diseases resulted in implementation of broad control
measures such as community sanitation, personal hygiene, and public
health education.
4 Presently HIV/AIDS is the fourth leading cause of death in
the world and it remains the leading cause of death in Asia.
5 The 20th century brought chemotherapy and antibiotics into
our infectious disease armamentarium.
6 The development of the microscope by Louis Pasteur in the
1600s allowed scientists to visualize micro-organisms for the first
time.
7 Egyptian papyrus paintings depict infectious diseases such as
tuberculosis.
8 Investigators described miasmas as the source of infections.
2 Give the explanation of following terms:
infectious diseases, miasmas, epidemic, antibiotics, pasteurization,
microorganisms.
3 Render the text Endocrine System Disorders. Use some of the
following expressions:
The main idea of the text is...
The text is about...
The text is devoted to...
The text deals with...
The purpose of the text is to give the reader some information on...
The aim of the text is to provide the reader with some material
(data) on...
Much attention is given to...
It should be stressed that...
Special attention is paid to...
(Your opinion on the text)
I found the text interesting (important, of no value, informative,
useful).
It gives the reader some information on...
We have come to know and understand a lot of things.
Unit 6
Pre-text assignment
Learn the key words and phrases:
tetanus, background, infectant, fungi, typhoid fever.
Infectious Diseases
Infection and Immunity
There are two basic types of disease: ones that are infectious, or
extrinsic, meaning that they are contagious or communicable and can
be spread by contact between people, and ones that are intrinsic, or
not infectious. Diseases in general and noninfectious diseases in
particular are discussed in essays devoted to those subjects. So, too,
is infection itself, a subject separate from infectious diseases: a
person can get an infection, such as tetanus or salmonella, without
necessarily having a disease that can be passed on through contact
with others in the same way that colds, malaria, or syphilis is spread.
The background on scientists' progressive understanding of the
microorganisms that cause disease and the means of fighting these
microorganisms are discussed in Infection. Among the leading
figures in that history were the French chemist and microbiologist
Louis Pasteur (1822-1895) and the German bacteriologist Robert
Koch (1843-1910), who contributed greatly to what is known today
as germ theory—the idea that infection and infectious diseases are
brought about by microorganisms. In most cases, the organisms are
too small to be seen with the naked eye. They include varieties of
amoeba and worm, discussed in the essay Parasites and Parasitology,
as well as viruses and some forms of bacteria and fungi, which
together are known as pathogens, or disease-carrying parasites. Other
terms related to infectious diseases, their agents, and the prevention
and study of them are defined in the essay Infection.
Immune Mechanisms
The human body has numerous mechanisms for protecting itself
from infectious disease, the first line of defense being the skin. Skin
shields us all the time from unseen attackers and generally is able to
prevent pathogens from entering the body; however, any break in the
skin, such as a cut or scrape, provides an opening for microorganisms
to invade the body. Germs that normally would be prevented from
entering the body are able to invade the bloodstream through such
openings. This is why it is so very important, in any situation
involving potential contact with infection, to protect the skin. With
the advent of AIDS, doctors and members of other professions who
are likely to touch people carrying diseases—including officers
arresting addicts or prostitutes—are much more likely to do their
work wearing heavy plastic gloves.
Suppose that a microorganism makes it through the barrier of skin,
thanks to a cut or other opening; if so, the body puts into action a
second defensive mechanism, the immune system. This system is a
network of organs, glands, and tissues that protects the body from
foreign substances. Without a properly functioning immune system, a
person could die simply by walking out the door in the morning and
coming into contact with an airborne infectant. Even in relatively
healthy people, the immune system may be unable to react
adequately to an invasion of microorganisms. In such cases, disease
develops.
Transmission of Diseases
Infectious diseases, by definition, are transmitted easily from one
person to another. We have all been told, for instance, not to drink
after someone who has a cold. On a much more serious level, persons
who are sexually active or potentially sexually active, but not settled
in a monogamous (one-partner) relationship, are advised to avoid
unprotected sexual contact so as not to contract AIDS or some other
sexually transmitted disease (STD). In these and many other cases,
microorganisms travel from the carrier of the disease to the
uninfected person. (Actually, in the case of AIDS, the pathogen is a
virus, which is not, strictly speaking, an organism or even a living
thing; however, viruses usually are lumped in with bacteria, amoeba,
and some fungi as microorganisms.)
Pathogens can be spread by many methods other than direct
contact, including through water, food, air, and bodily fluids—blood,
semen, saliva, and so on. For instance, any time a person with an
infection coughs or sneezes, they may be transmitting illness. This is
how diseases such as measles and tuberculosis are passed from
person to person. AIDS and various STDs, as well as many other
conditions, such as hepatitis, are transferred when one person comes
into contact with the bodily fluids of another. This is the case not
only with sexual intercourse but also with blood transfusions and any
number of other interactions, including possibly drinking after
someone. (Contrary to rumors that circulated in the early 1980s,
when AIDS first made itself known, that particular syndrome cannot
be transferred by saliva, but the common cold and other viral
infections can be.)
Cholera, caused by a bacterium found in dirty wells and rivers
from India to England (in the 1800s, at least), is an example of a
waterborne disease. Many foodborne pathogens tend to bring about
what would be more commonly thought of as an illness than a
disease, since in everyday language the latter term implies a longterm affliction, whereas food poisoning usually lasts for a week or so.
(Still, some forms of food poisoning can be fatal.) Bacterial
contamination may occur when food is not cooked thoroughly, is left
unrefrigerated, is prepared by an infected food handler, or otherwise
is handled in an unsanitary or improper fashion. (The case of
Typhoid Mary, discussed near the conclusion of this essay, is an
extreme example of this form of transmission.)
Additionally, diseases may be transferred by vectors—animals
(usually insects) that carry microorganisms from one person to
another. Vectors may spread a disease either by mechanical or by
biological means. Mechanical transmission occurs, for example,
when flies transfer the germs for typhoid fever from the feces (stool)
of infected people to food eaten by healthy people. Biological
transmission takes place when an insect bites a person and takes
infected blood into its own system. Once inside the insect's gut, the
disease-causing organisms may reproduce, increasing the number of
parasites that can be transmitted to the next victim. This is how the
Anopheles mosquito vector, for instance, transfers malaria.
Post-text assignments
1 Respond to the given assignments:
1 Describe two main types of disease.
2 How does a non-infectious disease differ from an infectious
disease?
3 Name the leading figures in history of microbiology.
4 Explain the immune mechanism of the skin.
5 What other immune mechanisms do you know?
6 How can infection disease transmit from one to another?
2 Imagine you have received the task to make an open lecture
entitled “Infectious Diseases”. What problems can you discuss in
it?
Unit 7
Pre-text assignment
Learn the key words and phrases:
pulmonary TB, health visitor, supervision, extrapulmonary TB,
scarring, immunosuppressant medication.
Treating tuberculosis
Treatment for tuberculosis (TB) depends on which type you have,
although a long course of antibiotics is most often used.
While TB is a serious condition that can be fatal if left untreated,
deaths are rare if treatment is completed.
For most people, hospital admission during treatment is not
necessary.
Pulmonary TB
If you are diagnosed with active pulmonary TB (TB that affects
your lungs and causes symptoms), you will be referred to a specialist
TB treatment team. This is a team of healthcare professionals with
experience in treating TB.
Treatment team
Your TB treatment team may include:
a respiratory physician - a doctor who specialises in
conditions that affect the lungs and breathing
an infectious disease specialist
a TB nurse
a health visitor - a qualified nurse with extra training who
helps families with babies and young children to stay healthy
a paediatrician (if necessary) - a doctor who specialises in
conditions that affect children
It is also likely that you will be assigned a key worker. This is
usually a nurse, health visitor or social care support worker who will
be the point of contact between you and the rest of the team and will
help co-ordinate your care.
Antibiotics
Pulmonary TB is treated using a six-month course of a
combination of antibiotics. The usual course of treatment is:
two antibiotics - isoniazid and rifampicin - every day for six
months
two additional antibiotics - pyrazinamide and ethambutol every day for the first two months
However, you may only need to take these antibiotics three times
a week if you need supervision (see below).
It may be several weeks or months before you start to feel better.
The exact length of time will depend on your overall health and the
severity of your TB.
After taking the medicine for two weeks, most people are no
longer infectious and feel much better. However, it is important to
continue taking your medicine exactly as prescribed and to complete
the whole course of antibiotics.
Taking medication for six months is the most effective method of
ensuring that the TB bacteria are killed. If you stop taking your
antibiotics before you complete the course, or if you skip a dose, the
TB infection may become resistant to the antibiotics (see below).
This is potentially serious, as it can be difficult to treat and will
require a longer course of treatment.
If treatment is completed correctly, you should not need any
further checks by a TB specialist afterwards. However, you may be
given advice about spotting signs that the illness has returned although this is rare.
In rare cases, TB can be fatal even with treatment. Death can
occur if the lungs become too damaged to work properly.
Extrapulmonary TB
Extrapulmonary TB (TB that occurs outside the lungs) can be
treated using the same combination of antibiotics as those used to
treat pulmonary TB. However, you may need to take them for 12
months.
If you have TB that affects your brain, you may also be prescribed
a corticosteroid, such as prednisolone, for several weeks to take at the
same time as your antibiotics. This will help reduce any swelling in
the affected areas.
As with pulmonary TB, it is important to take your medicines
exactly as prescribed and to finish the course.
Latent TB
Latent TB is where you have been infected with the TB bacteria
but do not have any symptoms of active disease. Treatment for latent
TB is usually recommended for:
people 35 years of age or under
people with HIV, regardless of their age
healthcare workers, regardless of their age
people with evidence of scarring caused by TB, as shown on a
chest X-ray, but who were never treated
Treatment is not recommended for people who have latent
tuberculosis and are over 35 years of age (and do not have HIV and
are not healthcare workers). This is because the risk of liver damage
increases with age and the risks of treatment outweigh the benefits
for some people.
Latent TB is also not always treated if it is suspected to be drugresistant (see below). If this is the case, you may be regularly
monitored to check the infection does not become active.
In some cases, treatment for latent TB may be recommended for
people requiring immunosuppressant medication. This medication
suppresses the immune system (the body’s natural defence against
illness and infection) and can allow latent TB to develop into an
active form of the disease. This may include people taking long-term
corticosteroids or people receiving chemotherapy.
In these cases, the TB infection should be treated before
immunosuppressant medication begins.
Treatment for latent TB involves either taking a combination of
rifampicin and isoniazid for three months, or isoniazid on its own for
six months.
Post-text assignments
1 Fill in the blanks and translate:
1 If you are diagnosed with …, you will be referred to a
specialist TB treatment team.
2 The exact length of time will depend on … and the severity of
your TB.
3 Taking medication … is the most effective method of
ensuring that the TB bacteria are killed.
4 If treatment is … , you should not need any further checks by
a TB specialist afterwards.
5 … is where you have been infected with the TB bacteria but
do not have any symptoms of active disease.
6 Treatment is not recommended for people who … and are
over 35 years of age (and do not have HIV and are not healthcare
workers).
7 In some cases, treatment for latent TB may be recommended
for people … medication.
2 Match the type of TB in column I with proper treatment in
column II:
Extrapulmonary TB
Isoniazid and rifampicin - every
day for six months
Latent TB
Isoniazid and rifampicin - every
day for twelve month
Pulmonary TB
Combination of rifampicin and
isoniazid for three months, or
isoniazid on its own for six
months
Unit 8
Pre-text assignment
Learn the key words and phrases:
influenza, strain, stuffy nose, seizure, precautions.
Influenza
What is Influenza?
Influenza, or flu, is a highly contagious respiratory illness caused
by influenza viruses. There are three main types of influenza virus
that cause infection in humans - types A, B and C - and many subtypes or strains. Influenza can occur throughout the year but
influenza activity usually peaks in winter.
Influenza is a vaccine-preventable illness but a new vaccine needs
to be given each year because influenza viruses change (mutate)
constantly. A new influenza vaccine is prepared each year to best
match the strains predicted for the coming influenza season.
What are the symptoms?
People with influenza typically experience some or all of the
following symptoms:
fever and chills
cough, sore throat and runny or stuffy nose
muscle aches, joint pains , headaches and fatigue (feeling very
tired)
nausea, vomiting and diarrhoea (more common in children
than adults).
Some symptoms may last for more than a week. Some people may
also experience very mild symptoms, particularly if they have some
immunity from a previous infection or vaccination.
Seek immediate medical advice if the illness quickly becomes
worse or if any of the following occurs:
shortness of breath or rapid breathing
chest pain
confusion or sudden dizziness
persistent vomiting.
How is it spread?
Influenza viruses are mainly spread by droplets made when an
infected person coughs or sneezes. Influenza can also be spread
through touching surfaces where infected droplets have landed.
People with influenza can be infectious from the day before their
symptoms start. Adults are most infectious in the first 3-5 days of
their illness, while children remain infectious for 7-10 days, and
people with weakened immune systems may be infectious for longer.
Who is at risk?
While anyone can get influenza, the following people are at higher
risk of complications from influenza infection (and are eligible for
free annual influenza vaccine):
All individuals aged 65 years or older
Pregnant women
Individuals aged 6 months and over with medical conditions
predisposing to severe influenza, namely:
o Cardiac disease, including cyanotic congenital heart disease,
coronary artery disease and congestive heart failure.
o Chronic respiratory conditions, including suppurative lung
disease, chronic obstructive pulmonary disease and severe asthma.
o Other chronic illnesses requiring regular medical follow up or
hospitalisation in the previous year, including diabetes mellitus,
chronic metabolic diseases, chronic renal failure, and
haemoglobinopathies.
o Chronic neurological conditions that impact on respiratory
function, including multiple sclerosis, spinal cord injuries, and
seizure disorders.
o Impaired immunity, including HIV, malignancy and chronic
steroid use.
o Children aged 6 months to 10 years on long term aspirin
therapy.
How is it prevented?
Influenza vaccination each year before winter arrives is the best
way to prevent influenza.
Seasonal influenza vaccination is available for anyone aged 6
months and over to protect against influenza, provided they do not
have a medical reason that precludes them from receiving influenza
vaccines.
People at higher risk of influenza complications (see "Who is at
risk") are strongly recommended to have an annual influenza
vaccination, and are eligible for free influenza vaccine under the
National Influenza Vaccination Program.
In addition to people eligible for free vaccine, annual influenza
vaccination is also recommended for those who frequently come in to
close contact with other people at higher risk of influenza
complications (such as health care workers, and family members), to
help protect vulnerable people from infection.
Take action to stop the spread of influenza by remembering to:
Cover your face when you cough or sneeze and throw used
tissues in a rubbish bin.
Wash your hands thoroughly and often. Wash hands for at
least 10 seconds, especially after coughing, sneezing or blowing your
nose, or use an alcohol-based hand rub.
Stay at home until you're well. Wait at least 24 hours after
your fever resolves so you that you are unlikely to infect other
people. Keep sick children away from school and other activities.
Call ahead to see a doctor. If you think you may have
influenza and you need to see a doctor, call first so the clinic can take
precautions to reduce the risk to other people.
How is it diagnosed?
Doctors usually diagnose influenza based on symptoms. The
diagnosis can be confirmed by testing a sample of fluid taken from
the back of the nose and throat or a blood sample. These tests are
usually only needed if the illness is severe or if there is an increased
risk of complications.
How is it treated?
The symptoms of influenza are usually managed by bed rest and
taking simple analgesics for muscle aches and pains.
Children under 16 years of age must not be given aspirincontaining medications while ill with influenza. This is due to the
increased risk of children developing Reye syndrome, a form of
encephalitis and liver degeneration.
Specific influenza antiviral medicines can reduce the severity and
the duration of influenza but need to be taken within 48 hours of the
first symptoms. These medicines need to be prescribed by a doctor,
and are usually considered for people at higher risk of complications
from influenza infection.
Post-text assignments
1 Topics for discussion
1 Symptoms of the influenza.
2 Describe ways of spreading influenza.
3 Speak of those people who at the risk of getting flu.
Prophylaxis of the influenza.
4 Treatment for the flu.
2 Look at the statements and say whether they are true or false.
1 There are three main types of influenza virus that cause
infection in humans - types I, II and III.
2 Influenza can occur throughout the year but influenza activity
usually peaks in spring.
3 Cough, sore throat and runny or stuffy nose are symptoms of
influenza.
4 Adults are most infectious in the first 10-15 days of their
illness, while children remain infectious for 30-40 days, and people
with weakened immune systems may be infectious for longer.
5 All individuals aged 40 years are at higher risk of
complications from influenza infection.
6 Influenza vaccination each year before winter arrives is the
best way to prevent influenza.
7 Seasonal influenza vaccination is available for anyone aged 7
years and over to protect against influenza, provided they do not have
a medical reason that precludes them from receiving influenza
vaccines.
8 Wait at least 12 hours after your fever resolves so you that
you are unlikely to infect other people.
Unit 9
Pre-text assignment
Learn the key words and phrases:
chickenpox, blister, varicella zoster virus, calamine lotion, preschool booster, 'fifth' disease, red specks, miscarriage.
Common childhood diseases
Chickenpox
Symptoms
Red, quite itchy, spots or blisters are typically scattered over the
entire body, spreading to the arms, legs and face.
The condition, caused by the varicella zoster virus, most
commonly occurs during the first decade of life.
The child has a moderate fever and mild flu-like symptoms prior
to the rash becoming apparent.
It's possible for some children to have these early symptoms and
to develop little or no rash, yet still to acquire long-term immunity
from the condition.
As a rule, the older the infected child is, the more severe the
disease.
Treatment
Symptomatic treatment with calamine lotion and/or
antihistamines, eg Piriton to reduce itching.
To reduce fever give paracetamol, eg Calpol and/or ibuprofen, eg
Junifen.
Should the spots become secondarily infected with bacteria, an
antibiotic may be necessary. Antiviral medicine is sometimes
prescribed in severe cases.
Incubation period
Between 10 to 20 days from being exposed to the infection and
showing symptoms.
Infectious period
Chickenpox is highly contagious from a few days before the
disease breaks out until the last blister has crusted over, which
usually occurs within a week of the first spots appearing.
The child should be excluded from school during this time and
avoid contact especially with pregnant women who have not
previously had the condition and anyone who is known to have a
compromised immune system, eg receiving chemotherapy.
The condition is transmitted through droplet infection from
coughing or sneezing and from the fluid within the blistering rash.
Whooping cough
Symptoms
Whooping cough is a bacterial infection affecting the respiratory
system, caused by the bacterium Bordetella pertussis.
The condition is characterised by fever, nasal discharge and long
fits of coughing followed by wheezy breathing and possibly
vomiting. Symptoms are typically worse at night.
Treatment
Antibiotic treatment is usually successful leading to a full
recovery. Fresh air is important.
Because of the risk of vomiting, the child should be given small
meals more often, instead of a few large ones.
Incubation period
This begins from seven days after exposure to the condition.
Infectious period
The disease is especially contagious during the first week, while
the child still has a trace of a cold.
Although the irritating cough has been known to go on for up to 3
months, the infectiousness wears off within five to seven weeks.
It is important to keep the child away from other children under
the age of one year.
Children should be excluded from school until they have
completed five days of antibiotic treatment.
Prevention
In the UK, children are vaccinated against the condition with a
series of three injections, one month apart starting at 2 months; and
again with a 'pre-school booster' injection aged between 3 and 4
years.
'Fifth' disease (erythema infectiosum)
Symptoms
The condition is due to infection with Parvovirus B19. The child
will sometimes initially develop mild flu-like symptoms.
All will eventually have red specks, firstly on the cheeks, and later
spreading to involve the arms, thighs and buttocks.
These are often blurred which makes it look like the child has
been slapped.
For this reason, fifth disease is often known as 'slapped cheek'
syndrome. It can last up to 14 days and is mostly seen in children
between the ages of 4 and 12.
Treatment
It cannot be treated, but disappears by itself. It is usually quite a
mild illness.
Incubation period
Two weeks between being exposed to the infection and showing
symptoms.
Infectious period
Once the rash appears, the disease is no longer infectious.
Complications
Pregnant women should avoid being in contact with children with
fifth disease as it may cause a miscarriage.
Pregnant women with a child who contracts fifth disease should
contact their doctor. The incubation period is a couple of weeks.
Three-day-fever (roseola infantum)
Symptoms
A child with three-day-fever has a high fever for three days.
The fever then drops and the child develops a rash consisting of
pale, reddish spots, perhaps with small heads. It affects the body and
spreads to the arms and legs, lasting for about 12-14 hours. Then its
over. It is mostly seen in children under the age of three years.
Treatment
Undress the child to ensure they aren't too warm.
Give the child fever reducing medication (such as paracetamol (eg
Calpol) and ibuprofen (eg Junifen)) to control their temperature and
plenty of fluids to avoid dehydration.
Incubation period
Between 10 to 15 days from being exposed to the infection and
showing symptoms.
Infectiousness
It is contagious during the whole period of the disease and up to
two to three days after.
Avoid contact with other children less than three years of age
during the whole period. Children may go back to childcare when
their temperature has returned to normal.
Post-text assignments
1 Match the name of disease in column I with proper symptoms in
column II:
Three-day-fever
Whooping cough is a bacterial
infection affecting the respiratory
system, caused by the bacterium
Bordetella pertussis.
Whooping cough
Red, quite itchy, spots or
blisters are typically scattered
over the entire body, spreading to
the arms, legs and face.
Chickenpox
The condition is due to
infection with Parvovirus B19.
The child will sometimes initially
develop mild flu-like symptoms.
'Fifth' disease
This disease affects the body
and spreads to the arms and legs,
lasting for about 12-14 hours.
Then it’s over.
2 Answer the questions:
1 Which common children diseases have a rush as a symptom?
2 What medicine is best for chickenpox?
3 Which disease is caused by Bordetella pertussis?
4 Why should the child be excluded from school during the
chickenpox?
5 How can chickenpox be transmitted?
6 What is the treatment for Whooping cough?
7 When is Whooping cough especially contagious?
8 How can 'Fifth' disease be treated?
9 What complications can 'Fifth' disease cause?
10 What is the treatment for Three-day-fever?
Unit 10
Pre-text assignment
Learn the key words and phrases:
pertussis, low-grade fever, coughing spell, gasp, regardless,
booster dose
Whooping cough
Whooping cough (pertussis) is an infection of the respiratory
system caused by the bacterium Bordetella pertussis (or B. pertussis).
It's characterized by severe coughing spells, which can sometimes
end in a "whooping" sound when the person breathes in.
It mainly affects infants younger than 6 months old before they're
adequately protected by immunizations, and kids 11 to 18 years old
whose immunity has started to fade.
Signs & Symptoms
The first symptoms of whooping cough are similar to those of a
common cold:
runny nose
sneezing
mild cough
low-grade fever
After about 1 to 2 weeks, the dry, irritating cough evolves into
coughing spells. During a coughing spell, which can last for more
than a minute, the child may turn red or purple. At the end of a spell,
the child may make a characteristic whooping sound when breathing
in or may vomit. Between spells, the child usually feels well.
Although many infants and younger children who become infected
with B. pertussis will develop the characteristic coughing episodes
and accompanying whoop, not all will. And sometimes infants don't
cough or whoop as older kids do. Infants may look as if they're
gasping for air with a reddened face and may actually stop breathing
(called apnea) for a few seconds during particularly bad spells.
Adults and teens with whooping cough may have milder or
atypical symptoms, such as a prolonged cough (rather than coughing
spells) or coughing without the whoop.
Contagiousness
Pertussis is highly contagious. The bacteria spread from person to
person through tiny drops of fluid from an infected person's nose or
mouth. These may become airborne when the person sneezes,
coughs, or laughs. Others then can become infected by inhaling the
drops or getting the drops on their hands and then touching their
mouths or noses.
Infected people are most contagious during the earliest stages of
the illness for up to about 2 weeks after the cough begins. Antibiotics
shorten the period of contagiousness to 5 days following the start of
antibiotic treatment.
Prevention
Whooping cough can be prevented with the pertussis vaccine,
which is part of the DTaP (diphtheria, tetanus, acellular pertussis)
immunization. DTaP immunizations are routinely given in five doses
before a child's sixth birthday. To give additional protection in case
immunity fades, the American Academy of Pediatrics (AAP) now
recommends that kids ages 11-18 get a booster shot of the new
combination vaccine (called Tdap), ideally when they're 11 or 12
years old, instead of the Td booster routinely given at this age.
The Tdap vaccine is similar to DTaP but with lower
concentrations of diphtheria and tetanus toxoid. It also should be
given to adults who did not receive it as preteens or teens. Pregnant
women should also receive the vaccine with each pregnancy,
regardless of whether they've had the vaccine in the past.
Getting the vaccine is especially important for people who are in
close contact with infants, because babies can develop severe and
potentially life-threatening complications from whooping cough. An
adult’s immunity to whooping cough lessens over time, so getting
vaccinated and protecting yourself against the infection also helps
protect your infant or child from getting it.
As is the case with all immunization schedules, there are important
exceptions and special circumstances. Your doctor will have the most
current information.
Experts believe that up to 80% of nonimmunized family members
will develop whooping cough if they live in the same house as
someone who has the infection. For this reason, anyone who comes
into close contact with someone who has pertussis should receive
antibiotics to prevent spread of the disease. Young kids who have not
received all five doses of the vaccine may require a booster dose if
exposed to an infected family member.
Professional Treatment
Call the doctor if you suspect that your child has whooping cough.
To make a diagnosis, the doctor will take a medical history, do a
thorough physical exam, and take nose and throat mucus samples that
will be examined and cultured for B. pertussis bacteria. Blood tests
and a chest X-ray also might be done.
A confirmed case of whooping cough will be treated with
antibiotics, usually for 2 weeks. Many experts believe that the
medication is most effective in shortening the duration of the
infection when given in the first stage of the illness, before coughing
spells begin. But even if antibiotics are started later, they're still
important because they can stop the spread of the pertussis infection
to others. Ask your doctor whether preventive antibiotics or vaccine
boosters for other family members are needed.
Some kids with whooping cough need to be treated in a hospital.
Infants and younger children are more likely to be hospitalized
because they're at greater risk for complications such as pneumonia,
which occurs in about 1 in 5 children under the age of 1 year who
have pertussis. Up to 75% of infants younger than 6 months old with
whooping cough will receive hospital treatment. In infants younger
than 6 months of age, whooping cough can even be life threatening.
Other potential complications include difficulty breathing, periods
of apnea, needing oxygen particularly during a coughing spell, and
dehydration due to poor oral intake.
While in the hospital, a child may need suctioning of thick
respiratory secretions. Breathing will be monitored and oxygen
given, if needed. Intravenous (IV) fluids might be required if a child
shows signs of dehydration or has difficulty eating. Precautions will
be taken to prevent the infection from spreading to other patients,
hospital staff, and visitors.
Home Treatment
If your child is being treated for pertussis at home, follow the
schedule for giving antibiotics exactly as your doctor prescribed.
Giving cough medicine probably will not help, as even the strongest
usually can't relieve the coughing spells of whooping cough. The
cough is actually the body’s way of trying to clear respiratory
secretions. (Due to potential side effects, cough medicines are never
recommended for children under age 6.)
During recovery, let your child rest in bed and use a cool-mist
vaporizer to help loosen respiratory secretions and soothe irritated
lungs and breathing passages. (Be sure to follow directions for
keeping it clean and mold-free.) In addition, keep your home free of
irritants that can trigger coughing spells, such as aerosol sprays;
tobacco smoke; and smoke from cooking, fireplaces, and woodburning stoves.
Kids with whooping cough may vomit or not eat or drink much
because of the coughing. So offer smaller, more frequent meals and
encourage your child to drink lots of fluids. Watch for signs of
dehydration, too, including thirst, irritability, restlessness, lethargy,
sunken eyes, a dry mouth and tongue, dry skin, crying without tears,
and fewer trips to the bathroom to pee (or in infants, fewer wet
diapers).
Post-text assignments
1 Answer the questions:
1 Which bacterium causes whooping cough?
2 How can pertussis be transmitted?
3 When people infected with pertussis are mostly contagious?
4 What are the symptoms of whooping cough?
5 How can whooping cough be prevented? What vaccines do
you know?
6 What tests can be done to confirm whooping cough?
2 Render the text Whooping cough
Use some of the following expressions:
The main idea of the text is...
The text is about...
The text is devoted to...
The text deals with...
The purpose of the text is to give the reader some information on...
The aim of the text is to provide the reader with some material
(data) on...
Much attention is given to...
It should be stressed that...
Special attention is paid to...
(Your opinion on the text)
I found the text interesting (important, of no value, informative,
useful).
It gives the reader some information on...
We have come to know and understand a lot of things.
Unit 11
Pre-text assignment
Learn the key words and phrases:
scarlet fever, scarlet-colored rash, underarms, specks of pus,
peeling, impetigo, soothing teas.
Scarlet Fever
About Scarlet Fever
Scarlet fever is caused by an infection with group A streptococcus
bacteria. The bacteria make a toxin (poison) that can cause the
scarlet-colored rash from which this illness gets its name.
Not all streptococci bacteria make this toxin and not all kids are
sensitive to it. Two kids in the same family may both have strep
infections, but one child (who is sensitive to the toxin) may develop
the rash of scarlet fever while the other may not. Usually, if a child
has this scarlet rash and other symptoms of strep throat, it can be
treated with antibiotics. So if your child has these symptoms, it's
important to call your doctor.
Symptoms of Scarlet Fever
The rash is the most striking sign of scarlet fever. It usually begins
looking like a bad sunburn with tiny bumps and it may itch. The rash
usually appears first on the neck and face, often leaving a clear
unaffected area around the mouth. It spreads to the chest and back,
then to the rest of the body. In body creases, especially around the
underarms and elbows, the rash forms classic red streaks. Areas of
rash usually turn white when you press on them. By the sixth day of
the infection the rash usually fades, but the affected skin may begin
to peel.
Aside from the rash, there are usually other symptoms that help to
confirm a diagnosis of scarlet fever, including a reddened sore throat,
a fever above 101°F (38.3°C), and swollen glands in the neck. The
tonsils and back of the throat may be covered with a whitish coating,
or appear red, swollen, and dotted with whitish or yellowish specks
of pus. Early in the infection, the tongue may have a whitish or
yellowish coating. A child with scarlet fever also may have chills,
body aches, nausea, vomiting, and loss of appetite.
When scarlet fever occurs because of a throat infection, the fever
typically stops within 3 to 5 days, and the sore throat passes soon
afterward. The scarlet fever rash usually fades on the sixth day after
sore throat symptoms began, but skin that was covered by rash may
begin to peel. This peeling may last 10 days. With antibiotic
treatment, the infection itself is usually cured with a 10-day course of
antibiotics, but it may take a few weeks for tonsils and swollen
glands to return to normal.
In rare cases, scarlet fever may develop from a streptococcal skin
infection like impetigo. In these cases, the child may not get a sore
throat.
Preventing Scarlet Fever
The bacterial infection that causes scarlet fever is contagious. A
child who has scarlet fever can spread the bacteria to others through
nasal and throat fluids by sneezing and coughing. If a child has a skin
infection caused by strep bacteria, like impetigo, it can be passed
through contact with the skin.
In everyday life, there is no perfect way to avoid the infections
that cause scarlet fever. When a child is sick at home, it's always
safest to keep that child's drinking glasses and eating utensils separate
from those of other family members, and to wash these items
thoroughly in hot soapy water. Wash your own hands frequently as
you care for a child with a strep infection.
Treating Scarlet Fever
If your child has a rash and the doctor suspects scarlet fever, he or
she will usually take a throat culture (a painless swab of throat
secretions) to see if the bacteria grow in the laboratory. Once a strep
infection is confirmed, the doctor will likely prescribe an antibiotic
for your child to be taken for about 10 days.
Caring for a Child With Scarlet Fever
A child with severe strep throat may find that eating is painful, so
providing soft foods or a liquid diet may be necessary. Include
soothing teas and warm nutritious soups, or cool soft drinks,
milkshakes, and ice cream. Make sure that the child drinks plenty of
fluids.
Use a cool-mist humidifier to add moisture to the air, since this
will help soothe the sore throat. A moist warm towel may help to
soothe swollen glands around your child's neck.
If the rash itches, make sure that your child's fingernails are
trimmed short so skin isn't damaged through scratching.
When to Call the Doctor
Call the doctor whenever your child suddenly develops a rash,
especially if it is accompanied by a fever, sore throat, or swollen
glands. This is especially important if your child has any of the
symptoms of strep throat, or if someone in your family or in your
child's school has recently had a strep infection.
Post-text assignments
1 Respond to the following tasks:
1 What do you know about scarlet disease?
2 Describe the symptoms of the scarlet fever.
3 Explain, how you can prevent scarlet fever.
4 How should parents caring for a Child With Scarlet Fever?
5 When should parents call the doctor?
2 Imagine you have received the task to make an open lecture
for parents entitled “Scarlet Fever”. What problems can you
discuss in it?
Unit 12
Pre-text assignment
Learn the key words and phrases:
raw materials, vitamin deficiency, scurvy, bleeding gums, rickets,
trace element
Vitamins and minerals
Every day, your body produces skin, muscle, and bone. It churns
out rich red blood that carries nutrients and oxygen to remote
outposts, and it sends nerve signals skipping along thousands of miles
of brain and body pathways. It also formulates chemical messengers
that shuttle from one organ to another, issuing the instructions that
help sustain your life.
But to do all this, your body requires some raw materials. These
include at least 30 vitamins, minerals, and dietary components that
your body needs but cannot manufacture on its own in sufficient
amounts.
Vitamins and minerals are considered essential nutrients—because
acting in concert, they perform hundreds of roles in the body. They
help shore up bones, heal wounds, and bolster your immune system.
They also convert food into energy, and repair cellular damage.
Micronutrients with a big role in the body
Vitamins and minerals are often called micronutrients because
your body needs only tiny amounts of them. Yet failing to get even
those small quantities virtually guarantees disease. Here are a few
examples of diseases that can result from vitamin deficiencies:
Scurvy. Old-time sailors learned that living for months
without fresh fruits or vegetables — the main sources of vitamin C
— causes the bleeding gums and listlessness of scurvy.
Blindness. In some developing countries, people still become
blind from vitamin A deficiency.
Rickets. A deficiency in vitamin D can cause rickets, a
condition marked by soft, weak bones that can lead to skeletal
deformities such as bowed legs. Partly to combat rickets, the U.S. has
fortified milk with vitamin D since the 1930s.
Just as a lack of key micronutrients can cause substantial harm to
your body, getting sufficient quantities can provide a substantial
benefit. Some examples of these benefits:
Strong bones. A combination of calcium, vitamin D, vitamin
K, magnesium, and phosphorus protects your bones against fractures.
Prevents birth defects. Taking folic acid supplements early
in pregnancy helps prevent brain and spinal birth defects in offspring.
Healthy teeth. The mineral fluoride not only helps bone
formation but also keeps dental cavities from starting or worsening.
There are two types of vitamins: fat-soluble and water-soluble.
Fat-soluble vitamins
Fat-soluble vitamins are found mainly in fatty foods such as
animal fats, including butter and lard, vegetable oils, dairy foods,
liver and oily fish.
While your body needs these vitamins every day to work properly,
you do not need to eat foods containing them every day.
This is because your body stores these vitamins in your liver and
fatty tissues for future use. These stores can build up so they are there
when you need them. However, if you have much more than you
need, fat-soluble vitamins can be harmful.
Fat-soluble vitamins are:
vitamin A
vitamin D
vitamin E
vitamin K
Water-soluble vitamins
Water-soluble vitamins are not stored in the body, so you need to
have them more frequently.
If you have more than you need, your body gets rid of the extra
vitamins when you urinate. As the body does not store water-soluble
vitamins, these vitamins are generally not harmful. However, this
does not mean that all large amounts are necessarily harmless.
Water-soluble vitamins are found in fruit, vegetables and grains.
Unlike fat-soluble vitamins, they can be destroyed by heat or by
being exposed to the air. They can also be lost in water used for
cooking.
This means that by cooking foods, especially boiling them, we
lose many of these vitamins. The best way to keep as many of the
water-soluble vitamins as possible is to steam or grill foods, rather
than boil them.
Water-soluble vitamins are vitamin C, the B vitamins and folic
acid.
Minerals are necessary for three main reasons:
building strong bones and teeth
controlling body fluids inside and outside cells
turning the food you eat into energy
Minerals are found in foods such as meat, cereals (including cereal
products such as bread), fish, milk and dairy foods, vegetables, fruit
(especially dried fruit) and nuts.
Essential minerals include calcium and iron, although there are
also many other types of minerals that are an important part of a
healthy diet.
What are trace elements?
Trace elements are also essential nutrients that your body needs to
work properly, but in much smaller amounts than vitamins and
minerals.
Trace elements are found in small amounts in a variety of foods
such as meat, fish, cereals, milk and dairy foods, vegetables and nuts.
Examples of trace elements are iodine and fluoride.
Post-text assignments
1 Answer the questions:
1 Why are vitamins important to us?
2 Why vitamins and minerals are considered essential nutrients?
3 Which diseases can result from vitamin deficiencies?
4 How many types of vitamins do you know?
5 What fat-soluble vitamins do you know?
6 Where are fat-soluble vitamins found?
7 What water-soluble vitamins do you know?
8 Where are water-soluble vitamins found?
9 Why are minerals necessary for the body?
10 What essential minerals do you know?
2 Fill in the blanks and translate:
1 Vitamins and minerals are considered … —because acting in
concert, they perform hundreds of roles in the body.
2 Vitamins and minerals are often called … because your body
needs only tiny amounts of them.
3 Old-time sailors learned that living for months without fresh
fruits or vegetables — the main sources of … — causes the … and
listlessness of scurvy.
4 A deficiency in vitamin D can cause … , a condition marked
by soft, weak bones that can lead to skeletal deformities such as
bowed legs.
5 … vitamins are found mainly in … such as animal fats,
including butter and lard, vegetable oils, dairy foods, liver and oily
fish.
6 Water-soluble vitamins are …, the … and … .
7 Essential minerals include … and …, although there are also
many other types of minerals that are an important part of a healthy
diet.
Unit 13
Pre-text assignment
Learn the key words and phrases:
antineoplastic, advent, to counteract the manifestations of disease,
dose-response relationship, magnitude, signal transduction,
pharmaceutical adverse effects, noxious
“Pharmacology is benefited by the
prepared mind. You need to know what
you are looking for”.
SIDDHARTHA MUKHERJEE, an
Indian-born American physician,
scientist and writer.
Introduction to Pharmacology
Pharmacology is the study of drugs and their effects on life
processes. This fundamental science is at the forefront of modern
medicine with demonstrated success in treating disease and saving
lives. It is also a discipline that drives the international
pharmaceutical industry to billion-dollar profits.
The goal of pharmacology is to understand the mechanisms by
which drugs interact with biological systems to enable the rational
use of effective agents in the diagnosis and treatment of disease. The
success of pharmacology in this task has led to an explosion of new
drug development, particularly in the past 50 years. Twentiethcentury developments include the isolation and use of insulin for
diabetes, the discovery of antimicrobial and antineoplastic drugs, and
the advent of modern psychopharmacology. Recent advances in
molecular biology, genetics, and drug design suggest that new drug
development and pharmacologic innovations will provide even
greater advances in the treatment of medical disorders in this century.
Pharmacology and Its Subdivisions
Pharmacology is the biomedical science related to the interaction
of chemical substances with living cells, tissues, and organisms. It is
particularly connected with the mechanisms by which drugs
counteract the manifestations of disease and affect fertility.
Pharmacology is divided into two main subdivisions,
pharmacokinetics and pharmacodynamics. The relationship between
these subdivisions is shown in Figure 1. Pharmacokinetics is
associated with the processes that determine the concentration of
drugs in body fluids and tissues over time, including drug absorption,
distribution, biotransformation (metabolism), and excretion.
Pharmacodynamics is the study of the actions of drugs on target
organs. A shorthand way of thinking about it is that
pharmacodynamics is what the drug does to the body, and
pharmacokinetics is what the body does to the drug. Modern
pharmacology is focused on the biochemical and molecular
mechanisms by which drugs produce their physiologic effects and
with the dose-response relationship, defined as the relationship
between the concentration of a drug in a tissue and the magnitude of
the tissue’s response to that drug. Most drugs produce their effects by
binding to protein receptors in target tissues, a process that activates a
cascade of events known as signal transduction.
Figure 1 - The relationship between pharmacokinetics and
pharmacodynamics
Toxicology
Toxicology is the study of poisons and organ toxicity. It focuses
on the harmful effects of drugs and other chemicals, and on the
mechanisms by which these agents produce pathologic changes,
disease, and death. As with pharmacology, toxicology is concerned
with the relationship between the dose of an agent and the resulting
tissue concentration and biologic effects that the agent produces.
Most drugs have toxic effects at high enough doses and may have
adverse effects related to toxicity at therapeutic doses.
Pharmacotherapeutics
Pharmacotherapeutics is the medical science concerned with the
use of drugs in the treatment of disease. Pharmacology provides a
rational basis for pharmacotherapeutics by explaining the
mechanisms and effects of drugs on the body and the relationship
between dose and drug response. Human studies known as clinical
trials are then used to determine the efficacy and safety of drug
therapy in human subjects.
Pharmacy and Related Sciences
Pharmacy is the science and profession concerned with the
preparation, storage, dispensing, and proper use of drug products.
Related sciences include pharmacognosy, medicinal chemistry, and
pharmaceutical chemistry. Pharmacognosy is the study of drugs
isolated from natural sources, including plants, microbes, animal
tissues, and minerals. Medicinal chemistry is a branch of organic
chemistry that specializes in the design and chemical synthesis of
drugs. Pharmaceutical chemistry, or pharmaceutics, is concerned
with the formulation and chemical properties of pharmaceutical
products, such as tablets, liquid solutions and suspensions, and
aerosols.
Post-text assignments
1 Complete the following definitions using the words in the box:
pharmacokinetics; pharmacognosy; excretion; distribution;
toxicity; molecular pharmacology; metabolism; pharmacodynamics;
ADR; dose-effect relationship; biotransformation; therapeutic;
overdose; pharmacology; synergism.
1 The study of the absorption, distribution, biotransformation
(metabolism), and excretion of drugs is known as … .
2 The biochemical and physiological effects of drugs and
mechanisms of drug action (the effects of a drug on the body or
organism) are defined as … .
3 … is the state of being noxious and refers to a drug’s ability to
poison the body.
4 The passage of an agent through blood or lymph to various
body sites is called … .
5 … stands for the last stage of pharmacokinetics that removes
drugs from the system.
6 The study of drugs derived from herbal and other natural
sources is referred to as… .
7 The abbreviated form of “adverse drug reaction” is … .
8 The process of conversion of drugs is known as … .
9 … is the sum of chemical and physical changes in the tissues,
consisting of anabolism and catabolism.
10 A toxic dose of the drug that causes harm is an… .
11 Study of how drugs interact with their target molecules is
defined as… .
12 The combined effect of two drugs is… .
13 The relationship between the dose of a drug (or other agent)
that produces therapeutic effects and the potency of the effects on the
person is defined as… .
14 … is the study of drugs, including their action and effects in
living body systems.
15 Effects meant to treat a disease or disorder are called …
effects.
2 Answer the following questions. Use them as a plan for
retelling the text:
1 What does pharmacology study?
2 What is the goal of pharmacology?
3 What new drugs have appeared in the past 50 years?
4 What are the main subdivisions of pharmacology?
5 What is pharmacodynamics / pharmacokinetics?
6 What is modern pharmacology focused on?
7 What is toxicology?
8 What is pharmacotherapeutics concerned with?
9 How does pharmacology provide a rational basis for
pharmacotherapeutics?
10 Which sciences are related to pharmacology?
3 Read SIDDHARTHA MUKHERJEE’S quotation, reflect on it
and say how you understand its meaning. Do you agree with it?
Why?
Unit 14
Pre-text assignment
Learn the key words and phrases:
intended for, derived from, derivative, alkaline reaction, quinine,
to yield, to enable, screening, to discern, structure-activity
relationship, three-dimensional conformation,
generic name, nonproprietary name, trademark, brand name
“In modern pharmacology it's so clear
that even if you have a fixed dose of a
drug, the individuals respond very
differently to one and the same dose".
ARVID CARLSSON, Swedish
pharmacologist, Nobel Prize laureate
Drug Sources
A drug can be defined as a natural product, chemical substance, or
pharmaceutical preparation intended for administration to a human or
animal to diagnose or treat a disease. The word drug is derived from
the French drogue, which originally meant dried herbs and was
applied to herbs in the marketplace used for cooking rather than for
any medicinal reason. Ironically, the medical use of the drug
marijuana, a dried herb, is hotly debated in many societies today.
Medication, and less frequently, medicament are terms that are
synonymous with the word drug.
Natural Sources of Drugs
Drugs have been obtained from plants, microbes, animal tissues,
and minerals. Among the various types of drugs derived from plants
are alkaloids, which are substances containing nitrogen groups and
give an alkaline reaction in aqueous solution. Examples of alkaloids
include morphine, cocaine, atropine, and quinine. Antibiotics have
been isolated from numerous microorganisms, including Penicillium
and Streptomyces species. Hormones are the most common type of
drug obtained from animals, whereas minerals have yielded a few
useful therapeutic agents, including the lithium compounds used to
treat bipolar mental illness.
Synthetic Drugs
Modern chemistry in the 19th century enabled scientists to
synthesize new compounds and to modify naturally occurring drugs.
Aspirin, barbiturates, and local anesthetics (e.g., procaine) were
among the first drugs to be synthesized in the laboratory.
Semisynthetic derivatives of naturally occurring compounds have led
to new drugs with different properties, such as the morphine
derivative oxycodone.
In some cases, new drug uses were discovered by accident when
drugs were used for another purpose, or by actively screening a huge
number of related molecules for a specific pharmacologic activity.
Medicinal chemists now use molecular modeling software to discern
the structure-activity relationship, which is the relationship between
the drug molecule, its target receptor, and the resulting
pharmacologic activity. In this way, a virtual model for the receptor
of a particular drug is created, and drug molecules that best fit the
three-dimensional conformation of the receptor are synthesized.
Drug Names
Chemical name describes chemical formula or molecular structure
of drug; for example, chemical name for ibuprofen is 2-pisobutylphenyl propionic acid.
Chemical names are usually very long, so shorter name are given
to drug; this is generic or nonproprietary name; recognized and
accepted as official name for drug; each drug has only one generic
name, such as ibuprofen.
Pharmaceutical company that originally developed drug has
exclusive rights to produce it for seventeen years; after that time, any
manufacturer may produce and sell drug.
When company manufactures drug for sale, it chooses brand, or
proprietary, name for product; company's trademark for drug; for
example, ibuprofen is known by several brand names, including
Motrin™, Advil™, and Nuprin™; all three contain same ibuprofen;
they are just marketed by different pharmaceutical companies.
Generic drugs are usually priced lower than brand name drugs;
physician can indicate on prescription if pharmacist may substitute
generic drug for brand name.
Chemical Name
2-/»-isobutylphenyl
propionic acid
Generic Name
ibuprofen
Acetylsalicylic acid
aspirin
Brand Names
Motrin™
Advil™
Nuprin™
Anacin™
Bufferin™
Excedrin™
Sudafed™
S-2- [1 -(methylamino) pseudoephedrine
ethyl]
Benzenemethanol
hydrochloride
Actifed™
hydrochloride
Nucofed™
Figure 2 - Examples of Different Drug Names
Post-text assignments
1 Match the pharmacology-related terms in the left column with
their definitions in the right column:
1 pharmacologist
2 antidote
3 cumulative effect
4 dissolution
5 generic name
6 side effects
7 excretion
8 opposition
9 pharmacist
10 absorption
11 adverse effects
12 toxicologist
13 trade (brand) name
14 anaphylactic shock
a) agent given to counteract harmful
effects of a drug
b) specialist (MD or PhD) who
studies the properties, uses, and
actions of drugs
c) professional who prepares and
dispenses drugs
d) harmful effects
e) effects not necessarily intended,
usually (but not always) undesirable
f) legal noncommercial name for a
drug
g) sudden and severe allergic
reaction that may be life threatening
h)
the
last
stage
of
pharmacokinetics that removes drugs
from the system
i) occurs when two drugs with
opposing actions interact, reducing the
effectiveness of one or both
j) the condition when poor
metabolism or excretion of a drug
leads to a build-up of the drug in the
body
k) complicated chemical formula
for a drug
l) the process of drug movement
into the systemic circulation
m) commercial name for a drug
n) specialist in the study of the
15 chemical name
harmful effects of drugs on the body
o) the process of dissolving
2 Scan the text and find English equivalents to the following
sentences:
1 Слово медикамент походить від французького слова
drogue, яке спочатку означало сушені трави стосовно трав на
ринку, які використовувалися для приготування їжі, а не з будьякою лікувальною метою.
2 Серед різних типів препаратів отриманих з рослин є
алкалоїди, які є речовинами, що містять азотовмісні групи і
дають лужну реакцію у водному розчині.
3 Гормони є найбільш поширеним типом ліків тваринного
походження, у той час як мінерали дали кілька корисних
терапевтичних речовин, в тому числі сполук літію, для
лікування біполярного психічного захворювання.
4 Сучасна хімія дозволила вченим 19 століття синтезувати
нові сполуки і модифікувати природні лікарські засоби.
5 Напівсинтетичні похідні природних сполук призвели до
появи нових лікарських препаратів з різними властивостями,
таких як замінник морфіну, оксикодон.
6 Таким чином, створюється віртуальна модель для
рецептора конкретного препарату і синтезуються молекули, які
найкращим чином відповідають тривимірній структурі
рецептора.
7 Фармацевтична компанія, яка першою розробила
препарат має ексклюзивні права на його виробництво протягом
сімнадцяти років; після чого, будь-який виробник може
виробляти і продавати лікарський засіб.
8 Немарочні лікарські препарати, як правило, за ціною
нижчі, ніж найменування патентованих ліків; лікар може вказати
на рецепті, чи може фармацевт замінити немарочний препарат
на марочну назву.
3 Take a look at Arvid Carlsson’s quotation and speculate on what
it is about. Choose the answer that corresponds to the meaning of
the quote. Correct the false statements:
a) individuals must always take a fixed dose of a drug;
b) physician must apply an individual approach to each patient
taking into account peculiarities of his / her organism;
c) patients respond to one and the same dose of a drug
identically.
Unit 15
Pre-text assignment
Learn the key words and phrases:
enteric-coated, gelatinous, pellet, to bring about, subcutaneous,
lozenge, formulation, to numb, anorectal, pessary, angina pectoris,
eruption, yeast infections, to dilate, buccal, potent, tedious
“Well, in pharmacology, if the effect is
local, it's of course absolutely awkward
to use it in any other way than as a
local treatment”.
ARVID CARLSSON, Swedish
pharmacologist, Nobel Prize laureate
The Different Types of Medicines and How They
Work
There are often questions asked regarding various aspects of
medicines. The effectiveness of dosing and administration of drugs:
what time of the day to take a drug, what route of administration is
the most effective (oral, injection, etc), how many times in the day
should a drug ideally be taken. Here are answers to some of these
frequently asked questions.
“Pharmacology” is the science that deals with the origin, nature,
chemistry, effects and uses of drugs. Medicines come in a variety of
different forms, including:
Pills, tablets – a small round or oval mass that contains medicine
and is swallowed. Some are “enteric-coated” with a substance which
only dissolves when it reaches the intestines. This ensures that the
active ingredient reaches the site of action or site of absorption.
Capsules – these are gelatinous containers containing powder or
tiny pellets (which are also often enteric-coated).
Injection – the administration of a liquid, into a part such as vein
or subcutaneous tissue. An injection usually brings about a quicker
effect, particularly if the drug is injected directly into the bloodstream
(IV – “intravenous”), rather than into a muscle (IM –
“intramuscular”); injections given just under the skin are called
“subcutaneous” injections.
Liquids/syrups – a concentrated solution of a sugar in water, with
medication dissolved in the liquid. Cough mixtures are commonly
sold in liquid form; liquid medicines are particularly useful in
children and the elderly, both of whom may struggle to swallow
tablets or capsules.
Lozenges – a medicated tablet, that is allowed to dissolve in the
mouth. Throat conditions are most commonly treated with lozenges,
which often have a mild anaesthetic effect to numb a sore throat.
Inhalants – a medication that is taken into the body through the
nose or respiratory system, through inhalation (breathing in). Asthma
medication, is available in inhaler formulations.
Creams, ointments – are semi-solid preparations, containing the
medicinal substance, to be used externally. They are applied directly
onto the skin or into the eyes or ears.
Suppositories – the medication is usually mixed with a suitable oil,
which is solid at room temperature, and is in the form of a large
“tablet shape” to be inserted anorectally, where the medication is
rapidly absorbed. Not the most pleasant form of medicine to
“administer”, but they are very useful in anorectal conditions, and if
the patient is vomiting or likely to vomit (medicines taken orally can
easily be ejected when vomiting).
Aerosol – same as inhalants
Pessary – the medication is usually mixed with a suitable oil,
which is solid at room temperature, and is in the form of a large
“tablet shape” to be inserted into the vagina, often used in vaginal
infections.
Routes of Drug Administration
Route of administration is the method by which drug is introduced
into body. To be effective, drugs must be administered by particular
route. In some cases, there may be a variety of routes; for instance,
female hormone estrogen can be administered orally in pill form or
by patch applied to skin.
Routes of administration are as follows:
Oral: drugs given by mouth; advantages are ease of administration
and slow rate of absorption via stomach and intestinal wall;
disadvantages include slowness of absorption and destruction of
some chemical compounds by gastric juices; some medications, such
as aspirin, can have a corrosive action on stomach lining.
Sublingual: drugs held under tongue and not swallowed; absorbed
by blood vessels on underside of tongue as saliva dissolves it; rate of
absorption is quicker than oral; nitroglycerin to treat angina pectoris
(chest pain) is administered by this route.
Inhalation: drugs inhaled directly into nose and mouth; aerosol
sprays are administered by this route.
Parenteral: invasive method of administering drugs; requires skin
to be punctured by needle; needle with syringe attached is introduced
either under skin or into muscle, vein, or body cavity.
Transdermal: medications coat underside of patch, which is
applied to skin where it is then absorbed; examples include birth
control patches, nicotine patches, and sea sickness patches.
Rectal: medications introduced directly into rectal cavity in form
of suppositories or solution; drugs may be administered by this route
if patient is unable to take by mouth due to nausea, vomiting, or
surgery.
Topical: medications applied directly to skin or mucous
membranes; in ointment, cream, or lotion form; used to treat skin
infections and eruptions.
Vaginal: tablets and suppositories inserted vaginally to treat
vaginal yeast infections and other irritations.
Eyedrops: drops used during eye examinations to dilate pupil of
eye for better examination of interior of eye; also placed into eye to
control eye pressure in glaucoma and treat infections.
Eardrops: drops placed directly into ear canal for purpose of
relieving pain or treating infection.
Buccal: drugs placed under lip or between cheek and gum.
Post-text assignments
1 Answer the multiple choice questions. Choose the best answer,
a, b, or c:
1 Vascular reaction of the skin characterized by a rash and severe
itching.
a) oxidation
b) ADR
c) uticaria
2 The drug name that means the same thing as generic name is
a) brand name
b) chemical name
c) nonproprietary
name
3 Use of drugs in the treatment of disease.
a) oxidation
b) chemotherapy
c) metabolism
4 The administration of a liquid, into a part such as vein or
subcutaneous tissue.
a) pellet
b) bloodstream
c) injection
5 How the body absorbs, distributes, metabolizes, or excretes a
drug.
a) alteration
b) absorption
c) biotransformation
6 The cell recipient, usually a specific protein, situated either in
cell membranes on cell surfaces or within the cellular cytoplasm.
a) reduction
b) excretion
c) receptor
7 A drug or another agent that blocks or antagonizes the effects of
another substance or function.
a) antagonist
b) capsule
c) tablet
8 Drugs mixed in a formulation with other ingredients to improve
the stability, taste, or physical form to allow appropriate
administration of the active drug.
a) toxicity
b) medicine (medication)
c) synergism
9 Study of new drug synthesis.
a) toxicologist
b) medicinal chemistry
c) chemotherapy
10 Agent given to counteract harmful effects of a drug.
a) antidote
b) chemical name
c) therapeutic
11 A medicated tablet, that is allowed to dissolve in the mouth.
a) inhalant
b) lozenge
c) liquid
12 The method by which drug is introduced into body.
a) oral
b) types of medicines
c) route of administration
13 Drugs inhaled directly into nose and mouth.
a) aerosol sprays b) ointments
c) eardrops
14 After the drug is in the liver, it is partly metabolized before
being sent to the body, where systemic effects occur.
a) first-pass effect b) adverse effects
c) cumulative effect
15 Commercial name for a drug.
a) chemical name b) generic name
c) trade (brand) name
2 Scan the texts and complete the sentences with missing words
or word combinations.
1 There are often questions asked regarding various aspects of
….
2 “Pharmacology” is the science that … the origin, nature,
chemistry, effects and uses of drugs.
3 Some pills are “enteric-coated” with a substance which only
dissolves when it … .
4 Capsules are … containers containing powder or tiny pellets.
5 An injection usually brings about a quicker effect, particularly
if the drug is injected directly into the … .
6 They are very useful in anorectal conditions, and if the patient
is … or likely to vomit.
7 To be effective, drugs must be … by particular route.
8 Needle with syringe attached is introduced either under skin
or into … .
9 Medications coat underside of … , which is applied to skin
where it is then absorbed.
10 Medications are introduced directly into rectal cavity in form
of … .
3 Choose the correct answer:
1 Which route of drug administration is used with potent and
lipophilic drugs in a patch formulation and avoids first-pass
metabolism?
a) topical
b) sublingual
c)rectal
d) oral
e) transdermal
2 Which one of the following routes of administration does not
have an absorption phase?
a) subcutaneous b) intramuscular
c) intravenous
d) sublingual
e) inhalation
3 Which of the following correctly describes the intramuscular
route of parenteral drug administration?
a) drug absorption is erratic and unpredictable
b) used to administer drug suspensions that are slowly absorbed
c) bypasses the process of drug absorption to give an immediate
effect
d) cannot be used for drugs that undergo a high degree of firstpass metabolism
e) poses more risks than intravenous administration
4 An elderly patient has problems remembering to take her
medication three times a day. Which one of the drug formulations
might be particularly useful in this case?
a) extended-release
b) suspension
c) suppository
d) skin-patch
e) enteric-coated
5 Which form of a drug name is most likely known by patients
from exposure to drug advertisements?
a) nonproprietary name b) British Approved Name
c) chemical name d) generic name
e) proprietary name
4 Take a look at Arvid Carlsson’s quotation, grasp the idea and
explain it.
Unit 16
Pretext Assignments
Learn the key words and phrases:
reproduction, fertilization, sex glands, menstrual cycle, ovaries,
gynecology
Female Reproductive System
Reproduction
Reproduction means the process by which a living entity or
organism produces a new individual of the same kind. The gonads, or
sex glands - the ovaries in the female and the testes in the male –
produce the germ cells (gametes) that unite and grow into a new
individual. Reproduction begins when the germ cells unite, that is a
process called fertilization.
The germ cells are the male spermatozoon and the female ovum,
or egg. These are specialized cells differing primarily from normal
body cells in one important way. Each sex cell contains exactly half
the number of chromosomes that a normal body cell contains. When
the ovum and spermatozoon unite, the cell produced receives half of
its genetic material from its female parent, and half from its male
parent; thus it contains a full, normal complement of hereditary
material.
Maturation of an ovum is a process controlled by hormones
secreted by the female's endocrine glands. An ovum, after leaving the
ovary, travels down a duct (uterine or fallopian tube) leading to the
uterus (womb). If coitus (copulation, sexual intercourse) has occurred
and sperm cells are present in the uterine tube, union of the ovum and
spermatozoon may take place. Ordinarily only one ovum matures
alternatively from each ovary during one menstrual cycle. However,
if by chance two eggs have been released and are fertilized by two
sperm, fraternal twins are formed. Identical twins are reproduced by a
single fertilized egg that divides into two eggs early in its
development.
Fertilization can occur only on the average of 4 days of every
menstrual cycle. The mature ovum lives only l or 2 days after
ovulation, and the sperm have about the same amount of time before
they perish in the female reproductive tract. The fertilized egg, which
is now called the embryo (and fetus after the second month) then
begins a 9-month period of development (gestation, pregnancy)
within the uterus.
The female reproductive system consists of organs that produce
ova and provide a place for the growth of the embryo. In addition, the
female reproductive organs supply important hormones that
contribute to the development of secondary sex characteristics (body
hair, breast development, structural changes in bones and fat).
Ova are produced by the ovary from the onset of puberty
(beginning of the fertile period when secondary sex characteristics
develop) to menopause (cessation of fertility and diminishing of
hormone production). If fertilization occurs at any time during the
years between puberty and menopause, the fertilized egg may grow
and develop within the uterus. Various hormones are secreted from
the ovary and from a blood-vessel-filled organ, placenta, that grows
in the wall of the uterus during pregnancy. If fertilization does not
occur, hormone changes result in the shedding of the uterine lining,
and bleeding, or menstruation, occurs.
Ovarian hormones that play important role in the process of
menstruation and pregnancy, and in the development of secondary
sex characteristics, are estrogen and progesterone. Other hormones
that arc responsible for the functions of the ovaries, breasts and
uterus, are secreted by the pituitary gland.
Gynecology is the study of the female reproductive system
(organs, hormones, and diseases); obstetrics is a specialty concerned
with pregnancy and delivery of the baby; and neonatology is the
study and treatment of the newborn child.
Major Organs of the Female Reproductive System
The female reproductive system consists of internal and external
organs of reproduction. The internal or essential organs for
reproduction are the ovaries, fallopian tubes, uterus, and vagina or
birth canal. The external genitalia include the labia majora, labia
minora, clitoris, vestibule of the vagina, and the greater vestibular
glands or Bartholin glands. The combined structures of the external
genitalia are known as the vulva.
Both the cervix of the uterus and vagina are lubricated by the
mucous secretions of Bartholin glands. A fold of membrane, the
hymen, is sometimes found partially covering the orifice of the
virginal vagina. A hymen may be ruptured at the first sexual
intercourse, even though there have been cases in which pregnancies
have occurred without any ruptures.
Ovaries
The reproductive system is linked to the body's system of
endocrine glands by the ovaries. Besides producing the ova, the
ovaries secrete the female sex hormones estrogen and progesterone.
These hormones influence the body's development and general
functioning as well as the sexual function.
The two ovaries, each about the size of a small plum, lie on each
side of the pear-shaped uterus at its wider upper part. Within each
ovary are thousands of small sacs called graafian follicles. Each
graafian follicle contains an ovum. When an ovum is mature, the
graafian follicle ruptures to the surface of the ovary, breaks through
its own outer covering, and is released. Release of an egg cell, called
ovulation, occurs about once in 28 days. The ruptured follicle fills
first with blood, and then with a yellow fatlike material. It is then
called the corpus luteum (yellow body).
Fallopian tubes
Fallopian tubes, oviducts, salpinges (sg. salpinx), or uterine tubes,
extend laterally from superior angles of the uterus. They transport the
ovum from the ovary to the uterus by rhythmic contractions of the
tube walls and by the cilia of the mucous membrane lining. The
opening of the tubes near the ovaries o pens directly into the uterus.
Each oviduct is a muscular tube and consists of the same three layers
found in the uterus: mucosa, serosa and a layer of smooth muscle. In
addition to conveying the ovum, an oviduct provides a passageway
through which sperm travel from the uterus toward the ovary. It is
within the uterine tube that fertilization takes place while the ovum is
moving through the tube. It usually takes the ovum about 5 days to
pass through the uterine tube. If coitus takes place near the time of
ovulation and no contraception is used, there is a likelihood that
sperm cells will be in the uterine tube when the egg cell is passing
through. If fertilization has not occurred, the ovum remains
unfertilized and, after a day or two, disintegrates.
Uterine tubes and ovaries are called the adnexa (accessory
structures) of the uterus.
Uterus and Vagina
Uterus is a hollow muscular pear-shaped organ, with muscular
walls and mucous membrane lining filled with a rich supply of blood
vessels. This organ is capable of stretching to contain a fertilized
ovum as it grows through the 9 months of pregnancy. The uterus is
located in the pelvic area between the bladder and rectum. The
rounded upper portion of the uterus is called the fundus, while the
larger central section is the corpus (body of the organ). The
specialized epithelial mucosa of the uterus is called the endometrium;
the middle, muscular layer is the myometrium; and the outer
membraneous tissue layer is the perimetrium. The uterus is also
adapted to hold the unborn infant securely and to nourish it. When
the ovum arrives, the hormones estrogen and progesterone produced
in the ovary have previously stimulated the uterus to prepare its
lining with extra blood. If the egg has not been fertilized it loses its
vitality, the hormone supply ceases, and the extra blood and tissues
are discharged from the body through the vagina in the menstrual
flow. The lower end of the uterus forms an opening called the cervix,
or neck, which protrudes into the birth canal or vagina.
Vagina is a muscular tube about seven and one-half cm long, and
its lining consists of a mucous membrane fold that gives the organ its
elastic quality. It extends from the cervix to the exterior of the body.
Besides serving as the organ of sexual intercourse, and receptor of
semen, the vagina discharges the menstrual flow. Like the uterus, the
vagina undergoes changes during pregnancy that enable it to stretch
to many times its usual size, allowing the infant to pass through it in
childbirth (parturition).
Breasts - Accessory Organ of Reproduction
The breasts or mammary glands are located in the upper anterior
aspect of the chest. During puberty the glands begin to develop as
they are exposed to periodic stimulation of two ovarian hormones,
estrogen and progesterone. Estrogen is responsible for the fatty
growth and increased size of the mammary glands as they reach full
maturity. The size of the breast is basically determined by the amount
of fat around the glandular tissue and is not indicative of its
functional ability. The other ovarian hormone progesterone forms the
lobules that are present in the breast. Each mammary gland has
approximately 20 lobes of glandular tissue. These lobes raise nipple.
Circling the nipple, there is a border of slightly darker skin referred to
as the areola.
Full development of the breasts is achieved by the time female
reaches the age of sixteen. The main purpose of the mammary glands
is secretion of milk for nourishment of the newborn infant. During
pregnancy, the hormones from the ovaries and the placenta stimulate
glandular tissue in the breasts to their full development. After
parturition (childbirth) hormones from the pituitary gland stimulate
the production of milk (lactation).
Menstrual Cycle and Menopause
The menstrual cycle consists of a series of events that are
associated with the maturation of the ovum. Approximately every 28
days the endometrium, the lining of the uterus, is prepared to receive
a fertilized egg. If no fertilization or conception occurs, the
endometrium along with the unfertilized ovum is released from the
body. The periodic discharge from the vagina of blood and tissues
from a nonpregnant uterus is called menstruation. Menstruation
occurs monthly, actually every 28 days or so from puberty to
menopause. If the mature egg is fertilized, menstruation will not take
place and the fertilized ovum implants itself upon the uterine wall
and continues to develop within the uterus.
Menopause is the span of time during which the menstrual cycle
diminishes and gradually stops. It is also called climacteric. During
this period the ovaries stop functioning and therefore menstruation
and childbearing cease. It is a natural physiologic process that results
from the normal aging of the ovaries and occurs when the ovaries can
no longer perform the function of ovulation and estrogen production.
It usually begins between 40 and 50 years of age and its duration
varies from 6 months to 3 years.
Pregnancy and Labour
If fertilization does occur in the uterine tube, the fertilized egg
begins to change immediately after. Soon the egg is dividing into a
cluster of two, then four, then more cells, as it makes its way down
the uterine tube toward the uterus for implantation. By the time the
egg reaches the uterus, in 3 to 5 days, the cells are formed in the
shape of a minute ball, hollow on the inside with an internal bump at
one side where the embryo will form. This aggregation of cells,
called a blastocyst, quickly buries itself in the lining of the uterus,
which is the process known as implantation.
As soon as the blastocyst is implanted, its wall begins to change
into a structure that eventually develops into the placenta. Through
the placenta the fetus secures nourishment from the mother and rids
itself of waste products. Essentially the placenta is a filtering
mechanism by which mother's blood is brought close to the fetal
blood without the actual mixing of blood cells.
The outermost membrane which surrounds the developing embryo
is called the chorion and the innermost is the amnion. The amnion
contains the fetus surrounded by the amniotic fluid. The amnion and
fluid are sometimes known as the "bag of water" which breaks to
signal the onset of labour.
The placenta, also known as the "afterbirth" because it becomes
detached from the uterus after delivery, produces its own hormone as
it develops in the uterus. This hormone is called human chorionic
gonadotropin – HCG, or pregnancy hormone, and it stimulates the
corpus luteum to continue producing hormones until about the third
month of pregnancy, when the placenta itself takes over the
endocrine function and releases estrogen and progesterone.
During the early stages of pregnancy, the future child grows at an
extremely rapid rate. The mother's body must undergo profound
changes to support this organism. The muscles of the uterus grow, the
blood volume expands, the work of the heart increases, the breasts
prepare for lactation and other adjustments are made throughout the
mother's body.
The average duration of pregnancy or the gestation period is about
280 days, or 9 calendar months, although it may vary considerably
from that average.
The events of menstruation and pregnancy are dependent not only
upon hormones from the ovary (estrogen and progesterone) but also
on hormones from the pituitary gland. These pituitary gland
hormones are follicle-stimulating hormone (FSH) and luteinizing
hormone (LH). These two hormones stimulate the development of
the ovum and ovulation. After ovulation, LH in particular influences
the maintenance of the corpus luteum and its production of estrogen
and progesterone.
Labour, or childbirth, is the physiologic process by which the fetus
is expelled from the uterus. It occurs in three stages: (l) opening or
dilation of the cervix is the time from the onset of labour to complete
dilation of the cervix (about 10 cm); (2) the second stage is called the
expulsion stage during which the baby must be pushed through and
out of the vagina; (3) the third stage is the stage of separation and
expulsion of the placenta; in this final stage the placenta detaches
itself from the uterine wall and is expelled.
Post text Assignments
1 Complete the sentence:
1 The main functions of the female reproductive system are …
2 The function of the breasts is …
3 Fertilization can occur only on the average of 4 days of every
4
5
6
7
The germ cells are the male … and the female …
Beside producing the ova, the ovaries secrete …
The study of female reproductive system is called …
Julius Cesar is said to have been born by …
2 Give the opposite of each term:
1 similar
2 resemble
3 young
4 male
5 health
6 include
7 complete
8 careful
9 give
10 wealth
3. Match the following terms with their meanings:
1. mastitis
a) muscular layer of the uterus
2. myometrium
b) release of egg from ovary
3. menorrhagia
e) union of egg and sperm cells
4. fertilization
d) inflammation of the breast
5. ovulation
e) excessive bleeding during menstruation
4 Give the meaning of the following terms:
1 ectopic pregnancy
2 placenta
3 breech presentation
4 C-section
5 areola
6 menopause
7 dystocia
8 amnion
9 salpingitis
10 perineum
5 Provide the plural form of the following nouns:
1 ovum
2 uterus
3 salpinx
4 fetus
5 cervix
6 placenta
7 corpus
8 endometrium
9 body
10 amnion
6 Provide the adjective forms of the following nouns:
1 l uterus
2 ovum
3 menstruation
4 breast
5 gamete
6 amnion
7 ovary
8 cervix
9 cortex
10 labium
7 Give appropriate medical word for the following:
1 Pregnancy sustaining hormone
2 Finger-like processes surrounding the abdominal opening of
each uterine tube
3 Removal of an ovary
4 Yellow body
5 Mongolism
6 Inflammation of an ovary
7 Innermost embryonic membrane
8 Accessory parts of the uterus
9 Cessation of a woman's reproductive function
10 The embryo from the beginning of the third month
8 Match the following terms with the most appropriate
definitions:
1. menstrual phase
2. premenstrual phase
3. postmenstrual phase
4. ovulatory phase
5. oligomenorrhea
6. amenorrhea
7. dysmenorrhea
8. metrorrhagia
9. menorrhagia
10. puberty
a. female reproductive organs are fully developed
b. absence of menstrual flow
c. days 1 to 5; lasts for approximately 3 to 5 days
d. abnormally light or infrequent menstruation
e. abnormally long or very heavy menstrual periods
f. graafian follicle ruptures, releasing the mature ovum
g. painful menstruation
h. interval between the menses and ovulation; days 6 to 12
i. days 15 to 28; if pregnancy does not occur, hormone level
drops—causing irritability, fluid retention, and breast tenderness
j. uterine bleeding at times other than the menstrual period
9 Read each definition carefully and identify the appropriate
word from the list that follows:
a) colposcopy
b) hysterosalpingography
c) conization
d) laparoscopy
e) culdocentesis
f) pap smear
g) mammography h) cryosurgery
i) pelvimetry
j) pelvic ultrasound
k) endometrial biopsy
Example: A diagnostic test for cervical cancer Pap smear
1. Visual examination of the vagina and cervix with a scope
2. Surgical removal of a cone-shaped segment of the cervix for
diagnosis or treatment
3. The destruction of tissue by rapid freezing with substances such
as liquid nitrogen
4. The surgical puncture through the posterior wall of the vagina
into the cul-de-sac to withdraw intraperitoneal fluid for examination
5. An invasive test for obtaining a sample of endometrial tissue
with a small curet for examination
6. The process of X-raying the uterus and the fallopian tubes
7. The process of viewing the abdominal cavity with a thin
flexible tube with a telescopic lens and light
8. The process of X-raying the soft tissue of the breast
9. The process of measuring the female pelvis manually or by Xray
10. A noninvasive procedure that uses high-frequency waves to
examine the abdomen and pelvis
10 The following is a discussion of secondary sex characteristic
changes experienced by the female during puberty, and instructions
for breast self-examination. Fill in the blanks with the most
appropriate word(s):
Puberty is the time during which the female experiences some
secondary sex characteristic changes. These changes include the
following: changes in the breast, which include (1) … deposition of
(2) … in the buttocks and thighs, creating a more (3) … appearance;
widening of the (4) … , making it more appropriate for childbirth;
and growth of (5) … and (6) … hair. The most evident change during
puberty is the onset of menstruation, with the first menstrual period
being called the (7) … . By the time a young woman reaches the age
of 20, she should perform the breast self-examination every month
about 7 to 10 days after the menstrual period. She should begin the
process by standing (8) … to observe the appearance of her breasts.
As she palpates her breasts for the presence of any lumps, she should
press firmly, moving in a circular motion, beginning at the armpit and
progressing toward (9) …. Each breast should be checked in the same
manner. After palpating the breasts for lumps, the female should then
check her breast while in the (10a) … and while (10b) ….
11 Match the terms with the appropriate descriptions:
1. lumpectomy
2. simple mastectomy
3. modified radical mastectomy
4. radical mastectomy
5. aspiration biopsy
6. colposcopy
7. cryosurgery
8. mammography
9. conization
10. culdocentesis
a. the surgical puncture through the posterior wall of the vagina
into the cul-de-sac to withdraw intraperitoneal fluid for examination
b. tissue or fluid sample is withdrawn for microscopic examination
and diagnosis
c. visual examination of the vagina and cervix with a colposcope
d. removal of only the tumor and a small margin of breast tissue
e. the process of examining with X-ray the soft tissue of the breast
to detect various benign and/or malignant growths before they can be
felt
f. removal of the breast, chest muscles, and lymph nodes on the
affected side
g. removal of the breast and lymph nodes on the affected side
h. the destruction of tissue by rapid freezing with substances such
as liquid nitrogen
i. surgical removal of a cone-shaped segment of the cervix for
diagnosis or treatment
j. only the breast is removed
12 The following medical scenario presents information on one
of the pathological conditions discussed in this chapter. Read the
scenario carefully and select the most appropriate answer for each
question that follows:
Selena Bandaro, a 40-year-old patient, is visiting her gynecologist
today due to the fact that she felt a lump in her breast that became
painful just before her menstrual period. Upon palpating the breast,
the doctor detected the presence of a single fluid-filled cyst. Although
he told Selena he believes she has fibrocystic breast disease, he has
ordered a mammogram and a biopsy of the cyst. Selena’s physician
has also recommended the use of a good support bra to lessen the
pain, restriction of caffeine in her diet, and mild analgesics for any
discomfort.
1. Selena asks the health care worker to explain what fibrocystic
breast disease means. The best explanation would be:
a. the presence of single or multiple fluid-filled cysts that can be
felt when examining the breasts
b. a benign, smooth muscle tumor of the breast often mistaken for
fibroid tumors
c. presence of multiple tumors varying in size and location within
the uterus
d. tenderness following adhesions (which are the result of
endometrial thickening)
2. Selena’s physician will most likely order which of the following
diagnostic tests to confirm the diagnosis of fibrocystic breast disease
and differentiate it from carcinoma?
a. mammography b. biopsy of the cyst c. bimanual examination
d. ultrasonography
3. To lessen the discomfort Selena is having from the fibrocystic
breast disease, she will be instructed to:
a. take narcotics
b. apply warm compresses to the chest
c. wear a bra with good support
d. avoid wearing a bra to decrease the pressure on the breasts
4. When instructing Selena on dietary changes, the health care
worker will include the importance of omitting:
a. protein b. fats c. calcium d. caffeine
5. What other preventative measure do you think the physician will
recommend to Selena in connection with her disorder?
a. monthly breast self-examination because the cysts tend to recur
b. no more breast self-examination because this may irritate the
area
c. regular Pap smears
d. checking the breasts monthly for equality of size
13 Translate into Ukrainian:
Drugs in Pregnancy
Since the tragic crippling of thousands of unborn children in the
late 1950s by the tranquilizer "thalidomide", the use of drugs during
pregnancy has become a highly controversial issue. Thalidomide was
prescribed as a mild sedative for pregnant women until its disastrous
side effects became obvious. The history of this drug has shown why
it is impossible to rely solely on animal tests in studying the effects of
drugs in pregnant women. Humans were found to be over 700 times
more sensitive to thalidomide than hamsters, for example. Even
enormous doses of the drug given to several species of animals failed
to produce the severe crippling, disfigurement, and limb deletion that
the drug causes in humans.
The effects of drugs in the fetus depend upon the particular drug
(or combination of drugs), the dosage, and most importantly, the
stage of fetal development. Embryonic cells multiply and grow
rapidly while food exchange and waste elimination occur through
simple diffusion. Therefore, drugs capable of rapid cellular diffusion
introduced during this period may cause significant embryonic
alterations. Between the fifth and eighth weeks, drug action can cause
abnormal tissue and/or organ differentiation. Timing is vital, with the
most severe effects occurring in the nervous system between days
fifteen to twenty-five; in the heart between days twenty to forty; in
the legs between days twenty-four to thirty-six; and in the eyes
between days twenty-four to forty. The major parts of the body have
usually been differentiated by the eight week of pregnancy, and the
danger of drugs diminishes. Some effects, like smoking, are
cumulative, however. Most authorities now recommend that the
ingestion of all drugs and medications, including over-the-counter
and prescription drugs, be kept to a minimum or totally eliminated
during all stages of pregnancy, unless such medications are
considered necessary by the physician. Pharmacogenetics, the study
of the interrelationship of hereditary constitution and drug responses,
has become an important specialty as a result of these concerns.
Unit 17
Pre-text assignment
Learn the key words and phrases:
flagellum, parenchyma, perineum, semen,
sterilization, stroma
seminiferous,
Male Reproductive System
Introduction
The male reproductive organs consist of the external genitalia: a
pair of testes, scrotum and penis; accessory glands that secrete special
fluids: the prostate, two seminal vesicles, a pair of bulbourethral
glands known also as Cowper's glands, and the ducts through which
these organs and glands are connected to each other and through
which the spermatozoa are ejaculated during coitus, seminiferous
tubules, epididymis, vasa deferentia and urethra.
Apart from providing structures necessary to transport and
maintain sperm viable, the male reproductive system produces the
male sex cells, spermatozoa or sperm, which contain one half of the
genetic material necessary to produce a living being.
The male sex cell, the spermatozoon (pl. spermatozoa = sperm
cells) is a microscopic, relatively uncomplicated cell, composed of a
head region, which contains nuclear hereditary material
(chromosomes), and a tail region, consisting o a flagellum, or a long
whiplike tail used for locomotion. The s perm cell contains relatively
little food and cytoplasm, for it needs to live only enough to travel
from its point of release from the male to where the egg cell lies
within the female (uterine tube). Only one spermatozoon of about
200 to 500 million s perm cells which may be released during a
single ejaculation (ejection of sperm and fluid from the male urethra)
can penetrate a single ovum and produce fertilization of the ovum. If
more than one egg is passing down the uterine tube when sperm are
present, multiple fertilizations are possible, and twins, triplets,
quadruplets, and so forth may occur. Twins resulting from the
fertilization of separate ova by separate sperm cells are called
fraternal twins. Fraternal twins, developing "in utero" with separate
placentas, have individual patterns of inheritance and resemble each
other no more than ordinary brothers and sisters.
Identical twins are formed from the fertilization of a single egg
cell by a single sperm. As the fertilized egg cell divides and forms
many cells, it somehow comes a part and each part continues
separately to undergo further division, each producing an embryo.
Both embryos share the same placenta. Identical twins are always of
the same sex and very similar in form and feature (physique).
All body organs contain parenchyma (parenchymal cells or tissue)
which perform the essential functions of the organ. Organs also
contain supportive, connective, and framework tissue, such as blood
vessels, connective tissues, and sometimes muscles as well. This
supportive tissue is called stroma (stromal tissue).
Anatomy of the Male Reproductive System
The male gonads consist of a pair of testes, also called testicles,
which develop in the kidney region of the body before descending
during fetal development into the scrotum, a sac enclosing the testes
on the outside of the body. The testes produce the sperm cells and the
male hormone testosterone, which gives a sexually mature male his
distinctively masculine characteristics and his sexual energy and
drive (libido). The interior of a testis is composed of a large mass of
narrow, coiled tubules called the seminiferous tubules. These tubules
contain cells which manufacture spermatozoa.
The seminiferous tubules are the parenchymal tissue of the testis,
which means that they perform the essential work of the organ. Other
cells in the testis, called interstitial cells, manufacture the male
hormone testosterone.
As soon as they are formed, sperm cells move through the
seminiferous tubules and are collected in ducts which lead to a large
tube at the upper part of each testis. This is the epididymis. The
spermatozoa become motile in the epididymis and are temporarily
stored there. The epididymis runs down the length of the testicle and
then turns upward again and becomes a narrow, straight tube called
the vas deferens (seminal duct or ductus deferens). The vas deferens
carries the sperm up into the pelvic region, around the urinary
bladder, and then into a duct leading toward the urethra. It is the vas
deferens that is cut or tied off when a sterilization procedure called a
vasectomy is performed.
The seminal vesicles are glands which are located at the base of
the bladder and they open into the vas deferens as it joins the urethra.
The seminal vesicles secrete a thick, yellowish substance that
nourishes the s perm cells and forms much of the volume of
ejaculated semen. Semen is a combination of fluid and spermatozoa
which is ejected from the body through the urethra. In the male, as
opposed to the female, the genital orifice combines with the urinary
opening (meatus).
Each epididymis is connected to a vas deferens, a part of the
spermatic cord that conducts the spermatozoa to the duet lying close
to the bladder. The vasa deferentia join with ducts leading from the
seminal vesicles just before the urethra. The combined duet is called
the ejaculatory duct. This duct passes through the prostate and joins
with the urethra. The urethra then conducts the semen through the
penis.
The prostate gland secretes a thick fluid which, as part of semen,
aids the motility of the sperm. This gland is also supplied with
muscular tissue which aids in the expulsion of sperm during
ejaculation. Cowper glands, or bulbourethral glands, are located just
below the prostate and they secrete an alkaline fluid into the urethra
that is necessary for the viability of the sperm.
Post text exercises
1 Complete the statements:
1 The organs of the male reproductive system are:
2 The main functions of the male reproductive system are:
3 Identical twins are formed from the fertilization of … sperm.
4 If more than one egg is passing down the uterine tube when s
perm are present … are possible.
5 Seminiferous tubules contain cells which produce …
6 In the male the genital orifice combines with the …
7 The ejaculatory duet passes through the … and joins with the
2 Give the opposite of each term:
1 remember
2 start
3 guilt
4 accept
5 implicit
6 humble
7 attach
8 true
9 identical
10 possible
3 Match the following terms with their meanings:
1 testosterone
a) removal of the prepuce
2 circumcision
b) prepuce
3 phimosis
c) scanty sperm
4 oligospermia
d) a hormone produced by interstitial cells in
testes
5 foreskin
e) a narrowing or stenos is of the prepuce
4 Give the meaning of the following terms:
1 stroma
2 a prostate gland
3
4
5
6
7
8
9
10
sperm cell
scrotum
Cowper glands
hypospadias
seminiferous tubules
teratocarcinoma of the testes
cryptorchism
varicocele
5 Provide the plural forms of the following nouns:
1 scrotum
2 placenta
3 hernia
4 epididymis
5 spermatozoon
6 testis
7 vas deferens
8 teratoma
9 flagellum
10 semen
6 Provide the adjective form of the following nouns:
1 embryo
2 maturation
3 hernia
4 ejaculation
5 perineum
6 testis
7 prostate
8 syphilis
9 semen
10 urethra
7 Match the terms with the applicable definition:
1 balanitis
2 chancre
3 glans penis
4 prepuce
5 hypospadias
6 epispadias
7 spermatogenesis
8 ejaculation
9 scrotum
10 vesicles
a. Blisters
b. The process of expelling the semen from the male urethra
c. Congenital defect in which the urethra opens on the upper side
of the penis at some point near the glans
d. A skin lesion, usually of primary syphilis, that begins at the site
of infection as a small raised area and develops into a red, painless
ulcer with a scooped-out appearance; also known as a venereal sore
e. A loose, retractable fold of skin covering the tip of the penis
f. Sac that houses the testicles
g. Inflammation of the glans penis
h. The tip of the penis
i. The formation of sperm
j. A congenital defect in which the urethra opens on the underside
of the penis instead of at the end
8 Match the procedures with the applicable description:
1 cryosurgery
2 circumcision
3 semen analysis
4 castration
5 TURP
6 vasectomy
7 suprapubic prostatectomy
8 orchiopexy
9 VDRL
10 PSA test
a. A serological test for syphilis, performed on blood serum
b. A test in which elevated levels may indicate significant prostatic
hypertrophy or cancer of the prostate
c. The surgical removal of the testicles in the male
d. A surgical procedure in which the foreskin of the penis is
removed
e. The destruction of tissue by rapid freezing with substances such
as liquid nitrogen
f. A surgical fixation of a testicle
g. Assessment of a sample of semen for volume, viscosity, sperm
count, motility, and percentage of any abnormal sperm
h. The surgical removal of the prostate gland by making an
incision into the abdominal wall, just above the pubis
i. The surgical removal of the prostate gland by inserting a
resectoscope through the urethra and into the bladder
j. Surgically cutting and tying the vas deferens to prevent the
passage of sperm
9 Read each definition carefully and identify the applicable word
from the list that follows:
a) AIDS b) balanitis c) chancre
d) genital
e) warts
f) phimosis
g) epispadias h) anarchism i) orchitis
j) urethritis
k) vasectomy l) cryptorchidism
Example: Men who contract trichomoniasis may experience
dysuria and inflammation of the urethra, which is known as:
urethritis
1. The abbreviation for acquired immunodeficiency syndrome:
2. Inflammation of the glans penis and the mucous membrane
beneath it:
3. Absence of one or both testicles:
4. Condition of undescended testicles:
5. Small, cauliflower-like, fleshy growths usually seen along the
penis in the male and in or near the vagina in women; sexually
transmitted:
6. A tightness of the foreskin (prepuce) of the penis that prevents it
from being pulled back:
7. Inflammation of the testes due to a virus, bacterial infection, or
injury:
8. A congenital defect in which the urethra opens on the upper side
of the penis at some point near the glans:
9. A surgical cutting and tying of the vas deferens to prevent the
passage of sperm:
10. A highly contagious lesion that appears within 10 days to a
few weeks after exposure to syphilis:
10 Complete the following definitions by filling in the blanks
with the most appropriate word:
1. Loss of appetite is known as ….
2. A pair of pea-sized glands that empty into the urethra just
before it extends through the penis (known as Cowper’s glands) are
called the glands.
3. When a disease, such as syphilis, remains inactive for a period
of time it is said to be ….
4. A tightly coiled tubule that houses the sperm until they mature
is known as the ….
5. A loose, retractable fold of skin covering the tip of the penis is
the foreskin, or ….
6. A vague feeling of bodily weakness or discomfort, often
marking the onset of disease or illness, is known as ….
7. An infection that sets up in a host whose resistance has been
decreased is known as an ….
8. The area between the scrotum and the anus in the male is
known as the ….
9. The specialized coils of tiny tubules that are responsible for
production of sperm and are located in the testes are known as the ….
10. A male hormone secreted by the testes responsible for the
secondary sex characteristic changes that occur in the male with the
onset of puberty is …
11 Read each statement carefully and select the correct answer
from the options listed:
1. The medical term for surgical repair of the glans penis is:
a. balanoplasty b. debridement c. cryosurgery d. prostatectomy
2. Inflammation of the urethra is known as:
a. ureteritis b. salpingitis c. balanoplasty d. urethritis
3. The medical term for painful urination is:
a. pyuria b. dysuria c. hematuria d. oliguria
4. The area between the scrotum and the anus in the male is called
the:
a. prepuce b. peritoneum c. perineum
d. truss
5. The absence of one or both testicles is termed:
a. balanitis b. prostatitis c. orchitis
d. anorchism
6. A congenital defect in which the urethra opens on the underside
of the penis instead of at the end is known as:
a. hypospadias b. epispadias c. cryptorchidism
d. orchitis
7. The surgical removal of the testicles in the male is known as:
a. circumcision b. castration c. orchidopexy
d. vasectomy
8. A surgical procedure in which the foreskin (prepuce) of the
penis is removed is known as:
a. circumcision b. castration c. orchidopexy
d. vasectomy
9. An X-ray of the urinary tract using no contrast medium is
known as a:
a. HSV-2 b. VDRL c. KUB d. NGU
10. A male sterilization is called a:
a. vasectomy b. circumcision c. orchidopexy d. semen analysis
12 The following medical scenario presents information on one
of the pathological conditions. Read the scenario carefully and
select the most appropriate answer for each question that follows:
Edward Bain, a 61-year-old patient, visited his internist today for a
physical exam. During the visit, Edward told the physician he was
having difficulty when trying to start urination. He also complained
that he was not able to maintain a constant stream. Edward’s internist
will follow up on this health history information by checking for
benign prostatic hypertrophy (BPH) during the physical exam.
1. The health care worker explains to Edward that the physician
will check his prostate by completing a:
a. orchidectomy b.
circumcision c. rectal exam
d. cystoscopy
2. Edward has many questions about this possible diagnosis. The
health care worker will describe BPH based on which of the
following explanations?
a. it is an accumulation of fluid in the scrotal sac and along the
spermatic cord creating pressure.
b. it is a tightness of the foreskin of the penis that prevents it from
being pulled back.
c. it is a protrusion of a part of the intestine through a weakened
spot in the muscles and membranes of the inguinal region of the
abdomen.
d. it is a noncancerous enlargement of the prostate gland, creating
pressure on the upper part of the urethra or neck of the bladder.
3. The health care worker explains to Edward that the following
diagnostic tests may be ordered by the physician to check for
infection or other abnormalities in the urine. The following tests will
be ordered:
1. urinalysis and residual urine
2. urine culture and KUB X-ray
3. vasectomy
4. cystourethroscopy
a. 1, 2
b. 3, 4
c. 1, 2, 4
d. 1, 2, 3, 4
4. Edward asks the health care worker what treatment is typically
ordered by the physician for patients with BPH. The health care
worker explains that the treatment really depends on the degree of:
a. urinary obstruction b. lymph node involvement
c. infection
in the scrotum
d. inflammation in the fallopian tubes
5. The health care worker explains to Edward that for patients
with recurrent problems due to hyperplasia of the prostate gland
surgery is usually indicated to remove the prostate. One type of
surgery used is called a:
a. epididymectomy b. circumcision
c. orchidopexy
d. transurethral resection
Unit 18
Pre-text assignment
Learn the following words:
ACQUIRED
obtained after conception or birth; not inherited
via genes;
ACUTE
sudden and serious, not chronic;
ANTIBIOTIC
a group of medicines such as penicillin used to
cure bacterial and fungal infections;
ASYMPTOMATIC
symptoms are not present, but infection
is present, and a person may be contagious;
BACTERIAL VAGINOSIS
an inflammation of the vagina
caused by the overgrowth of certain bacteria, including Gardnerella
vaginalis, Gardneralla mobiluncus, and Mycoplasma hominis;
CHANCRE
painless sore; a symptom of early syphilis;
CONGENITAL present at birth, either inherited or acquired
during pregnancy or birth;
CULTURE
to grow a microorganism in a laboratory; this
may be done as part of STD test;
ECTOPIC PREGNANCY
a pregnancy in which the
embryo implants itself in the woman’s fallopian tubes, or somewhere
else besides the uterus (sometimes caused by scar tissue left by STD);
ectopic pregnancies are fatal if not surgically removed;
FUNGUS a microscopic plant; sometimes harmful;
GERM
a harmful microorganism;
HEREDITARY inherited; something people get through their
parents’ genes;
HETEROSEXUAL
1) mostly attracted to people of another
gender (a man who gets crushes or falls in love mostly with women;
a woman who gets crushes or falls in love mostly with men 2) sexual
touch between people of two different genders;
HOMOSEXUAL 1) mostly attracted to people of your own
gender (a man who gets crushes or falls in love mostly with men; a
woman who gets crushes or falls in love mostly with women 2)
sexual touch between people of the same gender;
LESION sore or chancre, an opening of the skin allowing
infection, like HIV, to enter the body easily;
PROTOZOAN
a one-celled organism which is neither a plant
nor an animal; sometimes harmful;
SEQUELA
a condition that is the consequence of a
previous disease, plural: sequelae; i.e., PID can be a sequela of
chlamydia; blindness can be a sequela of CMV;
TRANSMISSIBLE
you can catch or spread it (synonyms:
communicable, contagious);
VIRUS
a packet of genes, not even a whole cell, which cause
harm by entering the body’s cells and turning them into virus
factories.
Note the abbreviations:
STD
Sexually Transmitted Diseases; any of about thirty
infection which people always, or often, catch through sexual contact
and possibly with NO symptoms, so “disease” can.
STI Sexually Transmitted Infection; a term used by health
providers to show that many infections don’t cause disease; they are
asymptomatic and don’t always cause adverse reactions.
AIDS
Acquired Immune Deficiency Syndrome, the end stage
of a disease caused by the germ “HIV”; usually fatal, often within 2
years of diagnosis.
CMV
CytoMegaloVirus; a virus that infects most people
worldwide and is usually harmless except in people with weakened
immune systems.
HIV
Human Immunodeficiency Virus (HIV), an organism
that can damage the immune system, causing what is called “HIV
Disease” and sometimes leading to AIDS.
NGU
Nongonococcal Urethritis; any inflammation of the
urethra which is not caused by gonorrhea; doctors use this term when
they don’t know what is causing the infection. It often turns out to be
Chlamydia.
PID
Pelvic Inflammatory Disease; any inflammation of the
uterus, fallopian tubes, or ovaries; usually caused by gonorrhea or
chlamydia; often leaves scar tissue that may, in the future, cause an
ectopic pregnancy, cancer, or infertility.
RTI
Reproductive
Tract
Infection;
any
harmful
microorganism that has entered the reproductive tract (vagina for
women, urethra for men), usually by sexual transmission, but not
always; does not include oral or anal infections.
VD Venereal Diseases (STDs) named for Venus, the goddess of
love, thus “love diseases”; this term is outdated and no longer used.
Sexually Transmitted Diseases
1. Definition of sexually transmitted infections
Sexually transmitted infections are infections which are mainly
transmitted from one person to another through intimate contact. The
infection can be spread through oral, vaginal, or anal sex, or though
contact with blood during sexual activity. Although uncommon,
transmission can also occur through direct contact with affected body
parts, tissue, or body fluids of infected persons. Some STIs such as
hepatitis B can also be transmitted through sharing or using
unsterilized needles.
Vertical transmission, where the mother passes the infection to her
child in utero or during childbirth, is also possible. HIV, hepatitis B
and syphilis are infections which can be transmitted in this way.
The term STIs describes infections caused by more than 30
different bacteria, viruses and parasites which are transmitted through
sexual intercourse. The common feature of these infections is their
mode of transmission and not their cause, origin, clinical features or
consequences. The most common STIs are the bacterial infections:
chlamydia, syphilis, gonorrhoea; and the viral infections: human
papillomavirus (HPV), HIV and hepatitis B. If not detected on time
or left untreated, these infections can have long-lasting adverse
effects. STIs such as HIV and HPV can be asymptomatic over long
periods of time while the signs and symptoms of others such as
genital herpes can be mild and passing. As a result no attention is
paid to them leading not only to delayed diagnosis and treatment, but
also increasing the chances of infections being passed on unaware
during unprotected sexual intercourse. If untreated, STIs can lead to
complications such as pelvic inflammatory diseases, ectopic
pregnancies or infertility in women, or epididymitis in men. In its
guidelines for surveillance of STIs published in 1999, the WHO
described STIs as a major global health problem leading to acute
illness, long-term disability and death, with serious medical and
psychological consequences for millions of men, women and infants.
HIV and syphilis are life threatening, hepatitis B, HPV and HIV
predispose to malignancy, and gonorrhoea and chlamydia affect
fertility. Chlamydia, gonorrhoea and syphilis can be cured using
antibiotics, while HIV is treatable but not curable. Most Hepatitis B
and HPV infections are cleared by the immune system within a few
months.
Chronic forms of Hepatitis B are however not well treatable and
persistent HPV infections can cause cervical and other forms of
cancer. Furthermore, HPV infection can cause genital warts, which
can be treated using topical creams or cryotherapy, but may also
disappear on their own.
2. Sexually Transmitted Diseases (STD, Venereal Diseases)
The following conditions, occurring in both men and women, are
the most communicable diseases in the world and are transmitted by
sexual intercourse:
chlamydial infection, bacterial infection of the urethra of men and
the vagina and cervix in women; men may experience dysuria and a
white or clear discharge from the penis; women may develop a
yellowish endocervical discharge, but often the disease is
asymptomatic genital herpes infection of the skin and mucosa of the
genitals caused by herpes virus (HSV) type II and sometimes type I;
after primary infection, numerous recurrent episodes of the disease
often follow; in more severe cases lesions may occur within the
vagina and cervix, with ulceration or necrosis of tissue; in such cases
there is higher incidence of cervical cancer; the disease is selflimiting and there is no drug known to be effective as cure.
gonorrhoea inflammation of the genital tract mucous membranes
caused by infection with gonococcus; other areas of the body such as
eye, oral mucosa, rectum, and joints may also be affected; symptoms
include dysuria and yellow mucopurulent discharge in men; some
women carry the disease asymptomatically, while others have pain,
vaginal and urethral discharge and salpingitis.
Syphilis (lues) - chronic infectious disease affecting any organ of
the body caused by a spirochete Treponema pallidum (spiral-shaped
bacterium); it enters the body through a break in the skin or mucous
membrane; at the initial stage the disease is referred to as primary
syphilis; about three weeks after exposure there is a development of a
chancre, or a firm, hard, ulcerlike lesion; in women the chancre
usually appears on the labia or within the vagina; secondary syphilis
occurs about four months after the disappearance of a chancre, which
may also appear on the lip, tongue, eyelid, or anus; the secondary
stage is characterized by a blotchy red rash over the body; thin white
sores appear on the mucosa of the mouth, throat, and genital area;
contagiousness at this time is extremely high; tertiary syphilis, also
called late syphilis, may develop after the symptoms of secondary
syphilis disappear or it may lie dormant for many years. Later stages
include damage to the brain, spinal cord, and heart. Syphilis (named
after a shepherd in an Italian poem) can be congenital in the fetus if
transmitted from the mother during pregnancy.
Trichomoniasis - infection of the genitourinary tract of either sex,
caused by Trichomonas vaginalis, a one-celled organism. This
condition is more commonly found in women and causes vaginitis,
urethritis, and cystitis. In men, it causes prostatitis, cystitis, and
urethritis, but most infected males are asymptomatic carriers who are
infectious to their partners. Several medications are available for the
treatment of Trichomonas.
3. STD Warning Signals for Females
- discharge: abnormal yellow or white vaginal discharge that
causes irritation or itching
- burning upon urination: painful and frequent urination
- sores: painless as well as painful sores or blisters in or around the
vagina, external sex organs, mouth, and rectum
- bumps and lumps: painless vaginal warts, sometimes irritated by
a heavy discharge from the vagina
- itching: intense itching in the genital area that may result in the
appearance of bumps and lumps
- lower abdominal pain: with or without fever, this condition may
indicate serious pelvic inflammatory disease (PID)
4. STD Warning Signals for Males
- discharge: white, clear, or often thick yellowish discharge of pus
from the penis or from the rectum following anal intercourse
- burning upon urination: painful and frequent urination
- sores: painless as well as painful sores or blisters on the penis,
around the genital area, mouth, and rectum
- bumps and lumps: bumpy, painless warts; body rash; pimplelike
bumps on the penis, swelling of lymph nodes in the groin
- itching: intense itching particularly in the genital area.
Post-text Assignments
1 Answer the following questions:
1 Is STD a sexually transmitted disease?
2 What are the names of some STIs?
3 Which of the following is a type of STD?
a) Gonorrhea b) syphilis c) genital herpes d) all of the above
4 How are STIs transmitted?
5 Can an infectious disease be passed through your body fluids?
6 Can all STIs be treated? Where can you go for help?
7 How do you know if you have STI?
8 How can you protect yourself?
2 Agree or disagree with the statement:
1 You can get a STI from a toilet seat.
2 If you wash with soap and water after intercourse, the possibility
of STI decreases.
3 Once a rash or sore heals, it means the infection has cured itself
and cannot be transmitted to anyone else.
4 the transmission of a STI is not possible if a condom is used.
5 A case of genital warts in a female places her at risk for cervical
cancer.
6 If gonorrhea or Chlamydia is left untreated, it can result in pelvic
inflammatory disease and eventual sterility.
7 HIV is transmitted through blood-to-blood contact.
8 Symptoms of HIV do not appear until several months or years
after infection.
9 When one partner has a bacterial infection, they do not need to
tell the other partner.
10 Crab lice or scabies can only be contracted by a person from a
low socio-economic background.
11 Most people with STI do not care if they pass it on to someone
else.
12 Campus, city, or country health clinics often treat STI free or at
reduced cost.
13 College students have a higher risk of contracting a sexually
transmitted disease than any other group.
14 A person under the influence of alcohol is more likely to
develop a STI.
15 You should not have sex while using drugs or alcohol.
3 Share your opinion on the following statements:
1 A person might think he or she had STD if…
2 If a person thinks she or he might have STD, she or he should…
3 Some STDs, if they aren’t cured, can lead to…
4 A person can reduce his or her risk of giving or getting STD
by…
4 Mark the following statements as True or False:
1 All STI are caused by viruses.
2 All STI can be cured easily.
3 Some STI have no symptoms.
4 Most people infected with HIV know they are infected.
5 The 24 to 39 year old age group is most commonly affected by
STI.
6 If you had an STI, you are immune to it and cannot get it again.
7 Some STI can cause infertility.
5 Translate into Ukrainian:
The Controversy of Sexually Transmitted Disease (STD)
Few diseases raise as much controversy as do the sexually
transmitted ones. In the mind of the general public, STD has become
confused with the method of its transmission. Indeed, "we have so
consistently identified this disease with illegimate sex that anybody
who gets it feels as though he were a criminal, no matter how he got
it." Some people claim there is never an "innocent party" to STD. But
how else could we classify the husbands and wives who contract
STD from a "cheating spouse"? Some infected persons develop so
much guilt that they do not seek medical care. Others fear the public
or private censure sometimes dispensed by health professionals so
they avoid treatment. The tragedy of STD is two-fold: while many of
the STDs are both curable and preventable, they are not being cured
in millions of cases, and they are not being adequately prevented!
Many people are convinced that the epidemic of STD throughout
the world is evidence of widespread immorality and the decline of
civilization. Some are more concerned that hundreds of thousands of
untreated individuals are harbouring dangerous and damaging
pathogens that possibly will be transmitted to unsuspected victims.
Other view the increasing numbers of STD cases reported to public
officials as evidence of increased personal and social responsibility.
It is hoped that infected people seek help because they want to be
cured and do not wish to give the disease to someone else. Still others
look upon the alarming statistics of incidence and attribute the
current epidemic to better case- finding and reporting techniques.
Perhaps all viewpoints have some merit. One thing is certain: most
people are not going to stop having sexual relations. If they do get
STD and are not treated early, they are likely to suffer severe
physical damage, perhaps even death.
Unit 19
Pre-text assignments
Learn the key words and phrases:
neoplasm, benign, malignant, tumor, spread, histogenesis, cancer,
oncology, metastasis
Oncology (Part 1)
Oncology is the study of tumors. It includes both malignant and
non-malignant growths, or neoplasms. Cancer is a disease generally
characterized by uncontrolled and excessive growth of body cells. It
may develop in any body tissue and at any age, although more
frequently in older people and rarely in the young ones. As cancerous
cell grow they eventually destroy their surrounding normal tissue and
they have also the ability to spread throughout the body, either by
bloodstream or by lymphatic system, and forms distant sites of
malignant growths, which often causes death.
Lung, breast and colorectal cancers rank highest in the percentage
of deaths for women, while lung, colorectal and prostate cancers are
highest in percentage of deaths for men.
Neoplasms
In healthy individuals cell division is an orderly process in which
body cells are produced for growth of the individual or for
replacement of cells that are destroyed or worn out. In some
instances, however, cell division is without purpose. The newly
formed cells increase at an uncontrolled rate, producing a lump or
swelling known as a tumor or neoplasm. Neoplasms may be either
benign or malignant.
Benign neoplasms
Benign neoplasms are growths that occur in body tissues. They are
composed of the same cells as the tissue in which they are growing.
For example, a benign tumor of a gland is composed of the glandular
tissue from which it is developing. Benign neoplasms are contained
within a capsule and do not invade the surrounding tissue. They harm
the individual only insofar as they place pressure on surrounding
structures. If the benign neoplasm remains small and places no
pressure on adjacent structures, it is not often removed. If it becomes
enlarged or places pressure on other organs or structures, it must be
removed. Benign brain tumours are always very serious, since the
cranial cavity is enclosed and pressure on other parts of the brain
inevitably results. As a general rule, however, benign tumors are not
life-threatening. Once they are removed, they do not regrow.
Malignant neoplasms
The cells that compose a malignant neoplasm often do not
resemble the tissue in which they are growing. In such cases the
tumor is said to be undifferentiated. The tumor cells lack
specialization in both structure and function. More significantly,
however, the cells of the malignant neoplasm are not encapsulated
and are able to spread to normal tissues. This invasive growth occurs
by direct extension or metastasis. In direct extension, the tumor
grows directly into normal tissue. This is called proliferation. With
metastasis the malignant cells from the primary tumor site find their
way into lymph channels or blood vessels and are carried to remote
body structures in which secondary malignant neoplasms develop.
Nomenclature of Tumours
Tumor nomenclature is based, in part, upon the tissue from which
the tumor originates. This is referred to as histogenesis. For purpose
of tumor nomenclature, four types of tissue are identified: epithelial,
connective (including muscle), hematopoietic (blood and lymph), and
nervous tissue. To indicate a benign tumor that arises from epithelial
or connective tissue, add the suffix -oma to the word root. An
exception to this rule is melanoma, which is a malignant tumor of
epithelial origin.
There are certain characteristics of a tumor that help in diagnosing
whether it is benign (noncancerous) or malignant (cancerous). A
benign tumor is usually enclosed within a capsule, grows slowly, and
does not invade surrounding tissue (metastasize). A malignant tumor
is not encapsulated, grows rapidly, and metastasizes.
Staging
Staging is an attempt to define the extent of cancer by classifying
it into three categories: T, N and M. T represents the primary tumor
site or place of origin; N represents local or regional node
involvement; and M tells whether or not there is metastasis. When
the primary site contains classifications of Tl, T2, T3, or T4, the
higher numbers would indicate progressive increase in tumor size and
involvement. Similarly, NO, Nl, N2, or N3 represents progressively
advancing nodular involvement. Finally, MO or M+ defines absence
or presence of metastasis, respectively.
Grading
Grading of a malignant tumor is an evaluation of the histological
makeup of the neoplasm. Generally, four grades are employed, Grade
l to Grade 4. Neoplasms that are composed of cells that closely
resemble the tissue from which they arise are given a Grade l rating.
The tissue demonstrates a minimum amount of anaplasia.
At the other extreme is Grade 4 in which there is a great deal of
anaplasia within the tumor. Such tumors are more serious and
prognosis is very poor. Grades 2 and 3 are intermediate grades
between these two extremes.
Post-text assignments
1 Answer the questions:
1 What is oncology?
2 What types of tumors do you know?
2 Complete the following statements:
1 In healthy … cell division is an … process.
2 Benign neoplasms are … within a …
3 Benign brain tumors are always very …
4 Staging is an … to define the … of cancer.
5 N represents … or … node involvement.
3 Match the following terms with their meanings:
1 proliferation
a) a new growth of tissue
2 staging
b) spread of malignant cells into the
surrounding tissue
3 sarcoma
c) a method of classifying malignant spread
4 neoplasm
d) malignancy of connective tissue origin
4 Give the meaning of the following term:
1 lethal
2 oncologist
3 multicentric
4 dormant
5 fibroma
6 lipoma
7 meninges
8 hemangioma
9 melanoma
10 necrotic
Unit 20
Oncology (Part 2)
Pre-text assignments
Learn the following items:
tissue of origin, benign, malignant
l. Epithelial Tissue Tumors:
surface epithelium
papilloma
carcinoma
glandular epithelium
adenoma
adenocarcinoma
2. Connective Tissue Tumors:
fibrous tissue
fibroma
fibrosarcoma
cartilage
chondroma chondrosarcoma
bone
osteoma
osteosarcoma
fat
lipoma
liposarcoma
blood vessels
hemangioma hemangiosarcoma
lymph vessels
lymphangioma lymphangiosarcoma
smooth muscle
leiomyoma leiomyosarcoma
3. Hematopoietic Tissue Tumors:
lymphoid tissue
myelocytic leukemia
granulocytic tissue
erythroleukemia
erythrocytic tissue
multiple myeloma
plasma cells
plasmocytoma
4. Nerve Tissue Tumors:
glial tissue
glioma
meninges
meningioma meningeal sarcoma
nerve cells
neuroma
neuroblastoma,
melanoma
neuroectoderm
nevus
neurolymphoma
retina
retinoblastoma
adrenal medulla
pheochromocytoma
The terms that are listed below describe the appearance of a
malignant tumour either on gross (visual) or on microscopic
examination
Gross Descriptions
cystic forming large open spaces filled with fluid; mucinous
tumours are filled with mucus, while serous tumours are filled with
watery fluid resembling serum; the most common site is in ovaries
fungating a mushroom-like pattern of growth during which tumour
cells pile one on top of the other; usually found in colon
inflammatory having the features of inflammation: redness, swelling,
heat; usually occur in the breast
medullar large soft fleshy tumors; usually occurring in the thyroid
and the breast necrotic containing dead tissue; any type of tumor can
outgrow its blood supply and undergo necrosis
polypoid projections extending outward from a base, like
extending from a stem or stalk ulcerating characterized by an open,
i.e. exposed surface resulting from death of the overlying tissue;
often found in the stomach breast, colon, skin
verrucous resembling a wart-like growth; tumors of the gingival
are usually of the verrucous type.
Microscopic Descriptions
alveolar
tumor cells look like microscopic sacs; commonly
found in tumors of the muscle, bone, fat and cartilage
diffuse
spreading evenly throughout the affected tissue; e.g.
malignant lymphomas are known to have such spread
dysplastic pertaining to abnormal cell formation, not clearly
cancerous; examples are dysplastic nevi
epidermoid
resembling squamous epithelial cells, often
occurring in the respiratory tract
follicular forming small microscopic, gland-type sacs; e.g. the
thyroid cancer
nodular
forming multiple areas of tightly placked clusters of
cells (nodules); e.g. malignant lymphomas
papillary small finger-like or nipple-like projections of cells;
e.g. bladder cancer
pleomorphic
composed of a variety of types of cells; e.g.
mixed-cell tumors
scirrhous densely packed, hard tumors, overgrown with fibrous
tissue; e.g. breast or stomach cancers
Treatment
Malignant tumors are cancers usually treated by three standard
methods either singly or in combination. These are: surgery, radiation
and chemotherapy. Besides these, new methods of treatment are
being extensively tested and gradually introduced. These include
biological agents, e.g. monoclonal antibodies, and differentiating
agents, e.g. those that cause tumor cells to differentiate stop growing
and die.
Post-text assignments:
1 Give appropriate medical word for the following:
1 the newly formed cells
2 an undifferentiated tumor
3 an attempt to define the extent of cancer
4 an evaluation of the histological makeup of the neoplasm
5 epithelial tissue having velvety appearance
6 penetrating the spaces within tissues
7 a cancerous tumor composed of cells of epithelial tissue
8 tumor of a smooth muscle
9 pertaining to the marrow
10 tumor of the skeletal muscle
2 Provide the adjective forms of the following nouns:
1 cancer
2 lymph
3 glioma
4 structure
5 predomination
6
7
8
9
10
multiplication
genesis
ability
neoplasm
granulocyte
3 Provide the plural form of the following nouns:
1 melanoma
2 nevus
3 axilla
4 radiotherapy
5 area
6 tremor
7 loss
8 neurosurgeon
9 disk
10 month
4 Translate into Ukrainian:
A 37-year-old male underwent abdominal resection for a
malignant melanoma arising in a nevus. One year later, he underwent
bilateral axillary node dissection, which indicated 2 of 23 left axillary
nodes positive for tumor. Two months later, his bone scan was
positive at the right proximal humerus, and a biopsy revealed
metastatic melanoma. The patient began having symptoms of
involvement of the fourth lumbar nerve roots and received
radiotherapy to the L-4 spine and the humerus with good response.
However, several weeks later, he noted progressive right leg
weakness and left leg sensory loss. Myelogram demonstrated two
metastatic lesions at 7 -12/L-1 and L-4 that were not thought to be
accessible surgically. The patient received further radiotherapy to the
affected vertebral areas. The patient received one course of BCNU (a
chemotherapeutic drug) from another physician who noted some
optic disk edema. The patient was placed on dexamethasone
(Decadron) therapy for 2 weeks, after which his course deteriorated
progressively with numbness in his upper extremities bilaterally, left
leg hyperesthesia, and tremors. Decadron was continued and a
neurosurgeon felt that little could be done surgically to reverse the
deficits.
References
1. Gary A. Thibodeau. Human body in health and disease / Gary
A. Thibodeau, Kevin T. Patton – Mosby, 2010. – 580 p.
2. All-in-One Study Guide / Pearson Prentice Hall, 2003. – 273 p.
3. B. D. Jones. Comprehensive Medical Terminology / Betty
Davis Jones – Dallas, 2008. – 1040 p.
4. B. A. Gylys. Medical terminology Systems / Barbara A. Gylys,
Mary Ellen Wedding – Philadelphia : F. A. Davis Company, 2013. –
588 p.
5. N. Thiere. Medical Terminology. Language for health care /
Nina Thiere, Deborah Nelson – Philadelphia : McGrowHill, 2011. –
730 p.
6. A. Ehrlich. Medical Terminology for Health Professions / Ann
Ehrich, Carol Schroeder – Delmar.
6. http://www.innerbody.com.
7. http://www.pfizer.co.za/wellatpfizer/about-medicine/medicinein-different-forms/types/2079.aspx
8. http://quizlet.com/14723720/test.
Навчальне видання
МЕТОДИЧНІ ВКАЗІВКИ
до практичних занять
на тему «Медична термінологія»
з дисципліни «Англійська мова»
(IV семестр)
для студентів спеціальності 7.110101 «Лікувальна справа»
денної форми навчання
Відповідальний за випуск Г. І. Литвиненко
Редактор С. В. Чечоткіна
Комп’ютерне верстання О. В. Шкурат
Підписано до друку 04.04.2014р., поз.
Формат 60х84/16. Ум. друк. арк. 6,74. Обл.-вид. арк. 6,04. Тираж 40 пр. Зам. №
Собівартість видання
грн
к.
Видавець і виготовлювач
Сумський державний університет,
вул. Римського-Корсакова, 2, м. Суми, 40007
Свідоцтво суб’єкта видавничої справи ДК № 3062 від 17. 12. 2007.