2.5 In vivo release of TA from the PU implants
advertisement

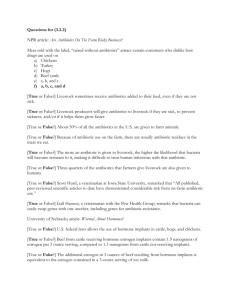
CONTROLLED RELEASE OF TRIAMCINOLONE ACETONIDE FROM POLYURETHANE IMPLANTABLE DEVICES: APPLICATION FOR INHIBITION OF INFLAMMATORYANGIOGENESIS Adriana F. Pereira1, Flávia C. H. Pinto1, Armando Silva-Cunha Junior2, Rodrigo L. Oréfice3, Eliane Ayres4, Sandra A. L. Moura5, Gisele R. Da Silva1 1 School of Pharmacy, Federal University of São João Del Rei, Divinópolis (MG), Brazil School of Pharmacy, Federal University of Minas Gerais, Belo Horizonte (MG), Brazil 3 Department of Metallurgical and Materials Engineering, Federal University of Minas Gerais, Belo Horizonte (MG), Brazil 4 Department of Materials, Technologies and Processes, Minas Gerais State University, Belo Horizonte (MG), Brazil 5 Center of Research in Biological Sciences, Federal University of Ouro Preto (MG), Brazil 2 E-mail: giselersilva@ufsj.edu.br The treatment of inflammatory pathologies usually requires repeated administration of conventional pharmaceutical dosage forms, reducing patient compliance. The development of drug delivery systems may overcome the drawbacks of the conventional therapy. In this study, implants based on polyurethane (PU) for local controlled delivery of triamcinolone acetonide (TA) were developed (TA PU implants). The TA PU implants were characterized by FTIR, SAXS and WAXS. The in vitro and in vivo release of TA from the PU implants was evaluated. Finally, the efficacy of TA PU implants in suppressing inflammatory-angiogenesis in a murine sponge model was demonstrated. FTIR results revealed no chemical interactions between polymer and drug. SAXS results indicated that the incorporation of the drug did not disturb the polymer morphology. WAXS showed that the crystalline nature of the TA was preserved after incorporation into the polyurethane matrix. The PU implants controlled TA release. The TA released from the PU implants efficiently inhibited the inflammatory-angiogenesis induced by sponge discs in an experimental animal model. TA PU implants could be used as drug delivery systems for the treatment of inflammatory-angiogenesis diseases because of their local controlled delivery of TA. Keywords: Waterborne polyurethane dispersion, Local drug delivery system, Implants, Inflammatory-angiogenesis diseases. 1. INTRODUCTION Segmented polyurethane elastomers have been extensively investigated in different biomedical applications, since they can be biocompatible, biodegradable, and can also display high mechanical properties [Jiang, 2007; Zhang, 2007]. In the field of tissue engineering, polyurethanes have been used as biomaterials for scaffold fabrication. These scaffolds based on polyurethanes serve as a matrix for the cells to attach, to proliferate and to form a functional tissue that can be implanted into the patient.5 Accordingly, polyurethane scaffolds have been used for generation of various tissue constructs, such as nerve conduits [Hausner, 2007; Tongkui, 2009], vascular grafts [Williamson, 2006; Zhang 2008], and cartilage [Bonakdar, 2010]. Another interesting biomedical application for biodegradable polyurethanes is related to the use of this type of material to control the release of drugs. Polymers can be loaded with the therapeutic agent and then implanted in specific organs. They would provide transport and controlled release of a therapeutic agent at the target site to treat or prevent different types of diseases [Da Silva, 2009]. Moreover, polyurethane-based systems can lead to a prolonged and controlled release of antimicrobial drugs [Francolini, 2010; Huynh, 2010], for antiseptic activity. Polyurethane intravaginal rings were produced to favor sustained release of antiretroviral agents to prevent the male-tofemale sexual transmission of HIV [Johnson, 2010]. Additionally, polyurethane nanocomposite implants were designed to control the corticosteroid release for the treatment of posterior segment ocular diseases [Da Silva, 2011]. The majority of the polyurethane-based delivery systems has been prepared by simple incorporation of the drug into the polymeric matrices and processing them into the desired morphology. Therefore, the drug remains physically entrapped in the polymer, but it is not anchored through chemical bonds. However, drugs have been also covalently incorporated into polyurethane foams, and they were released together with biomaterial degradation [Sivak, 2009]. In this work, waterborne polyurethane dispersion derived from poly(caprolactone), as soft segments, and isophorone diisocyanate and hydrazine, as hard segments were synthesized. Additionally, triamcinolone acetonide, a potent antiinflammatory drug, was dispersed into polyurethane prior to casting the films to yield triamcinolone acetonide-loaded polyurethane implants (TA PU implants). This drug delivery system was characterized by attenuated total reflectance-Fourier transform infrared, wide angle and small angle X-ray scattering in order to determine how the drug can interact with the polymer and affects its morphology. The analyzed structure of the biomaterial was also useful in understanding the in vitro and in vivo release of TA from the polyurethane. Finally, the efficacy of the TA-loaded polyurethane implants was demonstrated by inhibition of inflammatory angiogenesis in a murine sponge model. In summary, it was hypothesized that the obtained polyurethane implants may be useful as sustained/controlled delivery systems of TA for the treatment of chronic inflammatory pathologies. 2. MATERIALS AND METHODS 2.1 Synthesis of the aqueous polyurethane dispersion Aqueous polyurethane dispersion (PU) was prepared by a prepolymer mixing process, using a 250 mL three-neck glass flask equipped with a heating mantel, a mechanical stirrer and a thermometer. The macrodiol components of polycaprolactonediol (PCL 1000) (Tone Polyol 2221, M n = 1000 g.mol-1) and polycaprolactone-diol (PCL 2000) (Tone Polyol 0249, M n = 2000 g.mol-1) (Dow -USA) (Sigma-Aldrich), isophorone diisocyanate (IPDI) (Bayer – Brazil) (NCO/OH ratio of 2.3) and 2, 2bis(hydroxymethyl) propionic acid (DMPA) (98.3%, Fluka) were added to the reactor in the presence of dibutyl tin dilaurate (DBDLT) (Miracema Nuodex – Brazil) and the reaction was carried out at 70-75ºC within a nitrogen atmosphere for 4 h. The amount of free NCO groups on a percentage basis was determined by the standard di-butyl amine back titration method. After titration, the prepolymer temperature was allowed to drop to 40 ºC. The carboxylic acid groups were neutralized by the addition of triethylamine (TEA) (98%, Vetec - Brazil). The mixture was stirred for another 40 min to ensure that the reaction had been completed. All samples were dispersed by adding deionized water to the neutralized prepolymer which was stirred vigorously. After the dispersion, the amount of hydrazine (HZ) (solution 64%, Arch Química - Brazil) enough to react with free NCO groups was added to the reactor with a small amount of water, and stirring was continued for another 30 min. This chemical procedure was successful in producing a polyurethane dispersion with a solid content of about 25%. The composition of the polyurethane dispersion is shown in Table 1. Films were produced by casting the dispersion in a Teflon mould and allowing them to dry at room temperature for one week. Afterwards the films were placed in an oven at 60 ºC for 24 h [Ayres, 2007]. 2.2 Incorporation of the drug and preparation of the TA-loaded polyurethane implants (TA PU implants) Triamcinolone acetonide (TA) (Sigma-Aldrich, 99.0%) was incorporated into the polymer by dispersing it in the aqueous polyurethane dispersion prior to casting the films to yield materials having 20.5wt% of the drug. The dried films were cut into squares (5 mm in side) in order to obtain the TA-loaded polyurethane implants (TA PU implants). 2.3 Characterization Infrared spectra were collected in a Fourier transform infrared spectrophotometer (FTIR; Perkin Elmer, model Spectrum 1000). Measurements were carried out using the attenuated total reflectance (ATR) technique. Each spectrum was a result of 32 scans with a resolution of 4 cm-1. The measurements of Synchrotron Small Angle X-ray Scattering (SAXS) were performed using the beam line of the National Synchrotron Light Laboratory (LNLS, Campinas, Brazil). The photon beam used in the LNLS SAXS beamline comes from one of the 12 bending magnets of the electron storage ring. The white photon beam is extracted from the ring through a high-vacuum path. After passing through a thin beryllium window, the beam is monochromatized (λ = 1.608 Å) and horizontally focused by a cylindrically bent and asymmetrically cut silicon single crystal. The focus is located at the detection plane. The X-ray scattering intensity, I(q), was experimentally determined as a function of the scattering vector “q” whose modulus is given by q=(4/)sin(θ), where λ is the X-ray wavelength and θ being half the scattering angle. Each SAXS pattern corresponds to a data collection time of 900s. From the experimental scattering intensity produced by all the studied samples, the parasitic scattering intensity produced by the collimating slits was subtracted. All SAXS patterns were corrected for the non-constant sensitivity of the PSD, for the time varying intensity of the direct synchrotron beam and for differences in sample thickness. Because of the normalization procedure, the SAXS intensity was determined for all samples in the same arbitrary units so that they can be directly compared. Wide angle x-ray scattering (WAXS) was performed by using a synchrotron light beam with a wavelength of 1.608Å and an exposition time of 300 s. The scattering intensity was recorded by a Pilatus (100K, 33mm X 84mm) detector. The sample to detector distance used was 80mm. 2.4 In vitro release of TA from the PU implants The in vitro release of TA was carried out under sink conditions during 8 months. As the aqueous solubility of TA is 21.0 gmL at 28oC [Block, 1973], sink conditions were achieved with at least 181 mL for the evaluated polymeric implants. The TA PU implants were placed in different erlenmeyers containing 181 mL of phosphate buffer solution (PBS pH = 7.4) (n = 5). These erlenmeyers were placed inside an incubator set at 37oC and 30 rpm. At predetermined intervals, 181 mL of the PBS was sampled and the same volume of fresh PBS was added to each tube. The amount of TA released from each PU implant was assayed by HPLC method, and expressed as the cumulative percentage of TA released in the medium. The average of the obtained measurements was calculated and used to plot the release profile curve. 2.5 In vivo release of TA from the PU implants The animals were anesthetized with a mixture of (10 mg kg–1) xylazine and (100 mg kg–1) ketamine hydrochloride (i.p.). Their dorsal hair was shaved and the skin wiped with 70% ethanol. TA PU implants were aseptically inserted into a subcutaneous pouch that had been made with curved artery forceps through a 1cm long dorsal mid-line incision. After the implantation procedure, the animals were maintained in individual cages and provided with chow pellets and water ad libitum. The light/dark cycle was 12:12 h with lights on at 7:00 am and lights off at 7:00 pm. Post-operatively, the animals were monitored for any signs of infection at the operative site, or upon discomfort or distress; any mice presenting such signs were immediately sacrificed. At 7, 15, 30 and 45 days post-implantation, animals (n = 5 for each time) were euthanized and the TA PU implants were carefully removed from the subcutaneous pouch of the mice. The TA PU implants were fragmented using a scissor and the pieces were dissolved in 50 mL of a mixture of acetonitrile and ultra filtrated water (1:1). The content of TA remaining in the PU implants was measured by the HPLC method [Da Silva, 2012]. 2.6 Preparation of the sponge discs, implantation and treatment Non-biocompatible sponge discs of 5 mm in thickness, 8 mm in diameter and approximately 4.6 mg in weight (Vitaform Ltd, Manchester, UK) were used as the matrix for fibrovascular tissue growth. The sponge discs were soaked overnight in a 70% (V/V) ethanol solution and sterilized by boiling in distilled water for 15 min before the implantation surgery. The same implantation procedure described above was carried out in order to insert the sponge discs incorporated into TA PU implants (treated group) and sponge discs without the TA PU implants (untreated group). At 7 days post-implantation, mice (n = 6 for each group) were anesthetized and sacrificed by cervical dislocation and the sponge discs were carefully removed, dissected free from the adherent tissue, weighed and fixed in formalin (10% in isotonic saline), embedded in paraffin, and 5 µm-thick sections were obtained. The sections were stained with hematoxylin and eosin and examined under a light microscope. The images were digitized through a JVC TK1270/JGB microcamera. 3. RESULTS AND DISCUSSION 3.1 Characterization Figure 1 shows infrared spectra of the pure polyurethane (PU, Figure 1.a), polyurethane containing triamcinolone acetonide (TA PU implant, Figure 1.b) and pure triamcinolone acetonide (TA, Figure 1.c). A typical infrared absorption bands observed in TA can be detected in spectra of Figure 1.b and 1.c at 3392 cm-1, that can be associated with the stretching vibration of hydrogen bonded hydroxyl, and at ~1726 cm1 , corresponding to stretching vibration of the carbonyl group at aliphatic ester bonds. Other observed infrared absorption bands that are typical of TA are: ~1122 cm-1 – asymmetric axial deformation of C- O-C bond in aliphatic esters and ~1055 cm-1 – stretching vibration of C-F. The FTIR results obtained for pure TA were similar to those previously acquired [Araújo, 2010]. The characteristic infrared absorption bands observed in polyurethanes can be detected in spectra of Figure 1.a at 3336 cm-1, that can be associated with the stretching vibration of hydrogen bonded amines, indicating that isocyanate groups of the isophorone diisocyanate reacted with the hydroxyl and amino groups forming urethane and urea linkages. Other observed infrared absorption bands that are characteristic of polyurethane are: ~1722-1600 cm-1 – stretching vibration of the free carbonyl group of ester groups in poly(caprolactone), urethane and urea bonds, and hydrogen bonded carbonyl in urethane, indicating the synthesis of the polyurethane; ~2800-3000 cm-1 – stretching vibration of the –CH2 group. An absorption band around 2270 cm-1 was not observed in spectra, which indicated the absence of unreacted NCO groups [Pereira, 2010]. If this type of chemical group were present, the occurrence of side reactions which leads to the formation of allophanate or biuret linkages would be possible [Thomas, 2008]. The absorption bands of the pure polymer can also be observed in the spectrum of the polyurethane containing TA (Figure 1.b). The presence of unchanged absorption bands related to PU and TA in the spectra of the produced materials indicates that the incorporation process preserved the original chemical structure of the main components (no pronounced chemical interactions between PU and TA), being TA only partially dissolved in the polymeric matrix. Figure 1. FTIR spectra of pure polyurethane (PU) (a), polyurethane containing triamcinolone acetonide (TA PU implants) (b) and triamcinolone acetonide (TA) (c). Figure 2 shows Small Angle X-ray Scattering (SAXS) data for pure polyurethane, pure triamcinolone acetonide and polyurethane-loaded triamcinolone acetonide system. In curve (a) (Figure 2.a) associated with the pure PU, a small and broad scattering peak can be seen at q close to 0.7 nm-1 which one is usually related to the electron difference between hard and soft domains frequently present in polyurethanes. Phase separation in polyurethanes is often driven by large enthalpies of mixture associated with chemical differences between hard segments (based on urethane bonds) and soft segments (based on polyol units). The observed peak at qmax = 0.7 nm-1 can be associated with the distance (d) between hard domains by applying the Bragg’s equation (d = 2/qmax, i.e. d = 8.9nm). The incorporation of TA into PU (Figure 2.b) did not change significantly the SAXS pattern of the pure polymer, suggesting that no major changes in morphology of the polymeric system were observed. Only a small shift of the broad scattering peak at 0.7nm-1 towards higher values of q and an increase in the scattering intensity at values of q lower than 0.25nm-1 can be seen as, possibly, a consequence of the presence of TA crystals. Therefore, the presence of TA did not alter the natural phase-separated structure of pure PU as an indication that the drug did not interact strongly with the polymer. Figure 2. SAXS scattering data of pure polyurethane (PU) (a), polyurethane containing triamcinolone acetonide (TA PU implants) (b) and triamcinolone acetonide (TA) (c). When collected at wider angles, x-ray scattering (WAXS = wide angle x-ray scattering) can give information related to the distance between crystalline planes within a crystallite. Figure 3 reveals that no define scattering peaks can be noted in curves due to the pure PU containing poly(caprolactone) (Figure 3.a) as a consequence of the presence of a highly amorphous structure. Crystallization of poly(caprolactone) segments having low molar mass (< 2,000 g/mol) in polyurethanes is difficult to occur since these oligomers can not display conformation modes that would result in crystallization while being confined between hard domains [Ping, 2005]. The diffraction patterns of pure TA exhibited intense peaks at 2 = 20.8 and 26.3 and some peaks of lower intensity, indicating the crystalline nature of TA (Figure 3.c). The PU containing the drug (Figure 3.b) depicted typical diffraction patterns of the crystalline structure of TA. Although not shifted, the peaks of TA had a slight reduced intensity in TA-loaded PU implants when compared to pure TA, which may be attributed to the solubilization of TA when incorporated into polyurethane. Figure 3. WAXS curves of pure polyurethane (PU) (a), polyurethane containing triamcinolone acetonide (TA PU implants) (b) and triamcinolone acetonide (TA) (c). It was clearly observed that the obtained polyurethane was formed by separated domains of hard and soft segments. The microphase separation was due to the incompatibility between the hard and soft segments. Polar groups such as urethane in hard segments can hydrogen bond to each other to favor the formation of hard domains [Koberstein, 1992]. The microphase structure of the polyurethane can be changed by the introduction of functional and/or ionic groups into the polymer chains. For example, ionic groups can interact electrostatically, contributing to the structural arrangement of the segmented polyurethane [Francolini, 2010], and consequently altering mechanical properties and solubility [Suchocka-Galas, 1998]. However, according to the obtained SAXS results, the incorporation of TA into polyurethane did not lead to significant changes in the natural phase-separated structure of the polymer, suggesting that the drug was present within the polyurethane as isolated crystals. Furthermore, the FTIR and WAXS results showed no significant changes in the functional groups and amorphous pattern of the polyurethane after introduction of the TA into the polymer, indicating not only the integrity of the polyurethane, but also the maintenance of the chemical and morphological characteristics of the drug. 3.2 In vitro release of TA from the PU implants The in vitro release profile of TA from the PU implants was demonstrated in Figure 4. The PU implants exhibited a minimal burst release of the drug over the first 7 days, followed by a sustained TA release for a period of approximately 8 months. The PU implants released approximately 64% of the drug in 8 months under sink conditions. The minimal initial burst observed within 7 days may be due to the rapid dissolution and diffusion of the drug crystals deposited in the PU implant surface and/or the no intense chemical interaction between the drug and polymer. However, in the second stage, the TA was constantly and slowly released from the polymeric implant, which is most likely due to the hydrophobic character of poly(caprolactone) polymer present in the soft segments, and consequently its corresponding low permeability to water. The hydrophobicity of poly(caprolactone) can cause delay in water penetration and consequently the diffusion of the drug through the polyurethane matrix into the aqueous release medium was slow [Smith, 2007]. Furthermore, it is necessary to consider that the biodegradation of the polyurethane, based on poly(caprolactone) in the soft segments, in PBS medium is also slow, prolonging the period of TA release from the PU implants. In terms of bonds present in poly(ester urethane), the most susceptible to hydrolysis are ester bonds. However, the hydrolysis of ester bonds of urethane groups is one order of magnitude slower relative to ester bonds of the soft segment. Therefore, the soft segment bonds hydrolyze at a greater rate than hard segment bonds, and govern the degradation rate of the poly(ester urethanes) [Tatai, 2007]. In summary, at the initial stage, the TA release was mainly controlled by diffusion mechanism, and it was expected that the remained drug in PU implants was released, in the second stage, as a combination of polymer degradation and diffusion of the drug. Figure 4. In vitro cumulative TA released from PU implants. Results represent mean ± standard deviation (n = 4). 3.3 In vivo release of TA from the PU implants The in vivo release profile of TA from the PU implants, which was estimated as the amount of TA remaining in the implant, is shown in Figure 5. The PU implants exhibited an initial burst release of the drug over the first 7 days. This initial burst may be useful in rapidly achieving a local therapeutic concentration. During the first stage, the concentration of TA delivered by the PU implants was approximately 28.3 µg/day. In a second stage, that occurred between the 8th and the 45th days of the test, the PU implants provided the controlled and sustained TA release within subcutaneous tissue of mice. During this period, the PU implants released the drug at a daily dose of approximately 18.2 µg. Finally, these biodegradable implants released almost 81% of the drug in 45 days. It was considered that the mechanism of TA delivery from the PU implants was the simultaneous degradation of the polyurethane and the diffusion of the drug through the polymeric matrix, as previously described. However, the in vivo degradation of the polyurethane may involve other mechanisms such as the enzymatic hydrolysis by the presence of esterases and oxidation of the polymer due to the body environment that contains active moieties such as free radicals. Even though the enzymes are designed for highly specific interactions with particular biological substrates, some appear capable of recognizing and acting upon ‘‘unnatural’’ substrates such as polyurethanes [Santerre, 2005]. Accordingly, 64% of the TA was released from PU implants in vitro during 8 months and 81% of the drug was delivered by PU implants in vivo in 45 days. The differences between the simulated physiological conditions (in vitro test) and the physiological environment (in vivo test) explain the lack of correlation between the in vivo and in vitro profile release of TA from the PU implants. Figure 5. In vivo TA release from PU subcutaneous implants in mice. Sustained release of the drug was observed up to day 45 post-implantation. Results represent mean ± standard deviation (n = 5). 3.4 Inhibition of inflammatory angiogenesis in a murine sponge model The efficacy of TA PU implants in minimizing the inflammatory response and angiogenesis in a murine sponge model was evaluated. The murine sponge model of angiogenesis has been extensively used to induce acute as well as chronic inflammatory responses allowing the characterization of key components of fibrovascular tissue (cell influx, blood vessels formation, extracellular matrix deposition). The effects of various anti-inflammatory/anti-angiogenic compounds have been determined using this implantation technique [Xavier, 2010]. Histological analysis revealed that non-biocompatible sponge discs induced infiltration of inflammation-mediating cells, representing by macrophages, polymorphonuclear leukocytes, monocytes, fibroblasts and eventually giant cells form. The inflammation-mediating cells in the sponge discs of the untreated group were stained by hematoxylin and eosin (Figure 6.a). The permanence of the sponge matrices in vivo caused the acute inflammatory response to advance to the chronic phase, which is characterized by the fibrotic deposition around the non-biocompatible discs and by the presence of fibroblasts. Capillaries were evident in new vascularized areas of the sponge discs. By contrast, the cellular response, characterized by the massive infiltration, and the angiogenesis were inhibited in the sponge discs containing TA PU implants (Figure 6.b). Additionally, the TA eluted from the polymeric devices prevented progression to the chronic inflammatory phase revealed by the lack of fibrotic deposition around the sponge discs on day-7 post-implantation. Therefore, the glucocorticoid was controlled released from the PU implants directly into the targeted site and efficiently restricted the pathological condition by inhibiting the production of proangiogenic/inflammatory/fibrogenic components. Figure 6. Representative histological sections (stained with hematoxylin and eosin) of untreated group (a) (sponges) and treated group (sponges containing TA PU implants) (B). In (a), a dense inflammatory infiltrate was observed. In (b), the number of cells decreased in the sponge disc due to the TA release from the PU implants. The polyurethane incorporated into the sponge absorbed hematoxylin during the coloration process (circle). (a and b) – x40 magnification. The efficacy of TA PU implants in modulating key components of spongeinduced inflammatory angiogenesis in mice was attributed to the following reasons: (1) PU implants provided controlled TA release for a prolonged period, and displayed a persistent therapeutic effect for 7 days; (2) the concentration of TA released from the PU implants (approximately 28.3 µg/day, according to the in vivo TA release) was enough to inhibit the cellular uptake in the non-biocompatible sponge and the formation of new vessels in this experimental model; (3) the preparation technique of the TA PU implants did not affect the chemical and morphological integrity of the incorporated drug into the polymeric matrix and released from it, which was confirmed by FTIR, SAXS and WAXS results. The chemical integrity of the TA is an essential factor that assured the anti-inflammatory, immunosuppressive and anti-angiogenic actions of the glucocorticoids by genomic and/or non-genomic mechanisms [Stahn, 2008; Alangari, 2010]. 4. CONCLUSION In this study, TA was incorporated into polyurethane in order to develop a new implantable drug delivery system. The preparation technique of TA PU implants provided a uniform distribution of the drug throughout the system. Data obtained from FTIR showed no pronounced chemical interactions between PU and TA. SAXS results indicated that the incorporation of TA into the polymeric matrix did not promote any modification in the microdomain morphology of the polyurethane. Data obtained from WAXS demonstrated the integrity of the crystalline nature of the TA after incorporation into polyurethane matrix. The in vitro and in vivo release studies showed that TA was controlled released from the polymeric implants. The TA-loaded polyurethane implants efficiently modulated the key components of sponge-induced inflammatory angiogenesis in mice. Finally, the TA PU implants could locally control the delivery of this drug in order to inhibit the inflammatory-angiogenesis pathologies. AKNOWLEDGEMENT The authors would like to acknowledge the financial support received from the following institutions: FAPEMIG (Minas Gerais – Brazil), CAPES/MEC (Brazil), CNPq/MCT (Brazil) and Federal University of São João Del Rei (Minas Gerais – Brazil). REFERENCES 1. Ayres E, Oréfice RL, Yoshida MI. 2007. Eur Polym J 43:3510-3521. 2. Jiang X, Li J, Ding M, Tan H, Ling Q, Zhong Y, Fu Q. 2007. Eur Polym J 43:1838-1846. 3. Zhang C, Zhang N, Wen X. 2007. J Biomed Mater Res 82(3):637-650. 4. Hausner T, Schmidhammer R, Zandieh S, Hopf R, Schultz A, Gogolewski S, Hertz H, Redl H. 2007. Acta Neurochir Suppl 100:69-72. 5. Tongkui C, Yongnian Y, Renji Z, Li L, Wei X, Wang X. 2009. Tissue Eng Part C: Methods 15:1-9. 6. Williamson MR, Black R, Kielty C. 2006. Biomaterials 27(19):3608-3616. 7. Zhang L, Zhou J, Lu Q, Wei Y, Hu S. 2008. Biotechnol Bioeng 99:1007–1015. 8. Bonakdar S, Emami SH, Shokrgozar MA, Farhadi A, Ahmadi SAH, Amanzadeh A. 2010. Mater Sci Eng C 30(4):636-643. 9. Smith M, Omidi Y, Gumbleton M. 2007. J Drug Target 15(4):253–258. 10. Da Silva GR, Ayres E, Moura SAL, Cara DC, Oréfice RL, Silva-Cunha A. 2009. J Drug Target 17(5):374-383. 11. Francolini I, D’Ilario L, Guaglianone E, Donelli G, Martinelli A, Piozzi A. 2010. Acta Biomater 6:3482-3490. 12. Huynh TTN, Padois K, Sonvico F, Rossi A, Zani F, Pirot F, Doury J, Falson F. 2010. Eur J Pharma Biopharm 74:255-264. 13. Johnson TJ, Gupta KM, Fabian J, Theodore HA, Kiser PF. 2010. Eur J Pharma Biopharm 39(4):203212. 14. Da Silva GR, Silva-Cunha A, Behar-Cohen F, Ayres E, Oréfice RL. 2011. Mater Sci Eng C 31(2):414-422. 15. Sivak WN, Zhang J, Petoud S, Beckman EJ. 2009. Acta Biomater 5(7):2398-2308. 16. Block LH. 1973. J Pharm Sci 62(4):617-621. 17. Araújo FA, Rocha MA, Mendes JB, Andrade SP. 2010. Biomed Pharmacother 64(1):29-34. 18. Thomas V, Jayabalan M. 2008. J Biomed Mater Res Part A 89(1):192-105. 19. Ping P, Wang W, Chen X, Jing X. 2005. Biomacromolecules 6(2):587-592. 20. Koberstein JT, Galambos AF, Leung LM. 1992. 25:6195–6104. 21. Suchocka-Galas K. 1998. Eur Polym J 34:127–132. 22. Tatai L, Moore TG, Adhikari R, Malherbe F, Jayasekara R., Griffiths I, Gunatillake PA. 2007. Biomaterials 28:5407-5417. 23. Santerre JP, Woodhouse K, Laroche G, Labow RS. 2005. Biomaterials 26:7457-7470. 24. Xavier DO, Amaral LS, Gomes MA, Rocha MA, Campos PR, Cota BDCV, Tafuri LSA, Paiva AMR, Silva JH, Andrade SP, Belo AV. 2010. Biomed Pharmacoth 64(3):220-25. 25. Stahn C, Buttgereit F. 2008. Nat Clin Pract Rheumatol 4:525–533. 26. Alangari AA. 2010. Ann Thorac Med 5(3):133–139.