Form 8(a): Severe Allergies (Individual Health Care Plan and
advertisement
: Severe Allergies (Individual Health Care Plan and")
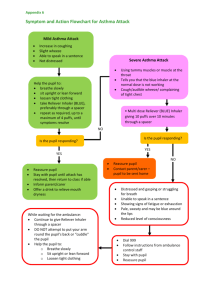
Appendix 2 Page 1 of 8 Form 8(a): Individual Health Care Plan Severe Allergies Pupil’s name: Date of birth: CHI: Address: Insert photograph of pupil School: This Plan should be completed by the pupil’s parent/carer and approved by the hospital consultant/ specialist nurse/GP. The parent/carer is responsible for obtaining a medical practitioner’s signature. Once completed, the parent/carer is responsible for taking a copy of this Individual Health Care Plan to all relevant hospital/GP appointments for updating Appendix 2 Page 2 of 8 Form 8(a): Individual Health Care Plan Severe Allergies Parent/Carer Contact 1 Parent/Carer Contact 2 Name: Name: Relationship to pupil: Relationship to pupil: Address: Address: Home: Home: Work: Work: Mobile: Mobile: Hospital/Clinic Contact General Practitioner Name: Name: Address: Address: Other Relevant Contact(s) Name: Name: Address: Address: Appendix 2 Page 3 of 8 Form 8(a): Individual Health Care Plan Severe Allergies Details of Medical Condition This pupil is allergic to: Details of Symptoms: The pupil may present with some of the following symptoms: itching red blotchy rash tingling/burning sensation in mouth tingling/burning sensation in lips swelling of lips swelling of eyes swelling of face swelling round sting increased rate of breathing behaviour change, less responsive or confused collapse Details of medication: Medication Dose Comment Antihistamine As per action flow chart. Repeat if vomited within 30 minutes. (Continue 4 hourly for 24 hours) (Name of medication) Ventolin (Salbutamol) Inhaler As per action flow chart. 2-10 puffs via spacer, 2 puffs initially then 1 puff per minute. Adrenaline Pen As per action flow chart. Parent/carer, please consult your GP when your child’s weight has reached 30kg as they will require the adult adrenaline pen. Details of emergency care: Follow instructions as per flow chart attached Appendix 2 Page 4 of 8 Form 8(a): Individual Health Care Plan Severe Allergies School Management of Severe Allergies (Anaphylaxis) All school staff, supply teachers, visiting teachers and support staff should be made aware of severe allergies and anaphylaxis and the emergency care procedures. Involved staff will know about the Individual Health Care Plan. In primary schools, one adrenaline pen will be kept in a zipped ‘poly pocket’, with the Emergency Care Flow Diagram, in the pupil’s classroom. Another adrenaline pen will be kept, with an Emergency Care Flow Diagram in a central, easily accessible place. In secondary schools, the pupil will carry one adrenaline pen with another adrenaline pen kept in a central, easily accessible place with an Emergency Care Flow Diagram. Emergency Care Flow Diagrams should also be kept in the register folder in each classroom It is the responsibility of the parent/carer to ensure that: medication is supplied to the school. the medication is ‘in date’. the medication is replaced as necessary. the medication is collected at the end of each summer term. all medication has the original pharmacy label attached stating: the pupil’s name, date of birth and dose. The class register should be clearly marked to indicate pupils with severe allergies so that when a supply teacher takes a class she/he is aware of any pupils with severe allergies in that class. Consideration of a pupil’s allergies will be made with regard to classes to be attended, e.g. food preparation or use of certain materials in science. Appendix 2 Page 5 of 8 Form 8(a): Individual Health Care Plan Severe Allergies Symptom and Action Flowchart for Severe Allergic Reaction (Anaphylaxis) Using an Adrenaline Pen Insert photograph Pupil’s name: of pupil Date of birth: Refer to Individual Health Care Plan and medication container for dosages. Severe Reaction Mild/Moderate Reaction Swollen lips Flushed, itchy, blotch skin Abdominal pain and nausea Swelling round eyes Fast breathing Swollen tongue Hoarse voice, difficulty swallowing Cough, difficulty breathing, noisy, laboured breathing Change in colour Feeling faint Deteriorating consciousness Collapse Lie pupil down and raise pupil’s feet. Give Antihistamine Dose: as stated on pharmacy label Administer Adrenaline Pen Hold Adrenaline Pen firmly Remove outer safety cap Hold the other end (non-safety cap end) of Adrenaline Pen 2 cm from the upper outer thigh Jab the Adrenaline Pen into the leg until you hear it click Hold the Adrenaline Pen firmly in place for 10 seconds Remove Adrenaline Pen from leg Rub leg If asthmatic, give reliever via spacer (2 puffs). Another 8 puffs, 1 puff per minute, can be given. Contact parent/carer to inform them that their child has had an allergic reaction Supervise closely. If condition worsens to severe reaction: Dial 999 Follow instructions from ambulance control Stay with child If no improvement in breathing or alertness after 5 minutes, give second Adrenaline Pen Contact parents Give Adrenaline Pen to ambulance staff Appendix 2 Page 6 of 8 Form 8(a): Individual Health Care Plan Severe Allergies Symptom and Action Flowchart for Severe Allergic Reaction (Anaphylaxis) WITHOUT Using Adrenaline Pen Pupil’s name: Date of birth: Refer to Individual Health Care Plan and medication container for dosages. Insert photograph of pupil Mild/Moderate Reaction Swollen lips Flushed, itchy, blotch skin Abdominal pain and nausea Swelling round eyes Fast breathing Severe Reaction Give Antihistamine Dose: as stated on pharmacy label If asthmatic, give reliever via spacer (2 puffs). Another 8 puffs, 1 puff per minute, can be given. Swollen tongue Hoarse voice, difficulty swallowing Cough, difficulty breathing, noisy, laboured breathing Change in colour, pale, clammy Feeling faint Deteriorating consciousness Collapse Lie pupil down and raise pupil’s feet. Contact parent/carer to inform them that their child has had an allergic reaction. Supervise closely. If condition worsens to severe reaction: Dial 999 Follow instructions from ambulance control Contact parents Stay with child Appendix 2 Page 7 of 8 Form 8(a): Individual Health Care Plan Severe Allergies Agreement to Individual Health Care Plan This Plan was completed on and its contents agreed by the undersigned. Parent/carer I wish my child to have the medication/care detailed in this plan and I accept that the emergency services will be summoned, as required, in the event that the school staff are unable to administer the plan at any time where appropriate. Name of parent/carer: Signature: Date: Pupil (if appropriate) Name of pupil: Signature: Date: Medical practitioner Name of medical practitioner: Signature: Date: Date of next planned review: (no later than 12 months from date of initial completion) For completion by school: CONFIRMATION OF THE SCHOOL’S AGREEMENT I agree to the procedures detailed in this plan being administered in school. In the event that these procedures cannot be implemented at any time the school will follow the advice received from the health professionals in summoning the emergency services where appropriate. Name of Head Teacher/designated person: Signature: Copy to be given to parent/carer. Date: Appendix 2 Page 8 of 8 Form 8(a): Individual Health Care Plan Severe Allergies Review Agreement Statement by Parent/Carer Pupil’s name: Date of birth: I confirm that the existing Individual Health Care Plan for my child continues to reflect the current needs of my child. I agree therefore that the review date stated on the Plan remains applicable. I will inform the school if my child’s needs change prior to the agreed review date. Name of parent/carer: Signature: Copy to be given to parent/carer. Date: