File - Respiratory Therapy Files
advertisement

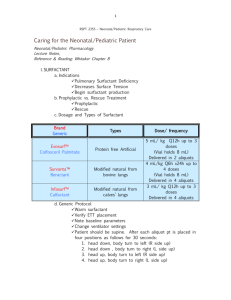
Ventilatory Strategies for Newborns Management of premature infants with respiratory distress syndrome should be guided by data from clinical trials. Management of premature infants with respiratory distress syndrome should be guided by data from clinical trials. By Rune Toms, MD, & Wally Carlo, MD Neonates frequently present with respiratory problems requiring oxygen supplementation and more invasive respiratory support. Despite several advances in respiratory care in neonates, complications from respiratory failure such as bronchopulmonary dysplasia (BPD) and air leaks are prevalent and can lead to increased mortality and important long-term morbidities. Management of premature infants with respiratory distress syndrome (RDS) should be guided by data from clinical trials. The driving force behind recent studies of respiratory support is to find the optimal combination of available therapies to improve survival and survival without BPD, a chronic lung disease that develops mostly in premature infants as a result of abnormal lung development secondary to lung damage from immaturity, mechanical ventilations and oxygen. Considerations for management strategies will be discussed. Surfactant Reduces Mortality State-of-the-art use of surfactant therapy, nasal continuous positive airway pressure (NCPAP) is a new option, based on evidence from the SUPPORT, COIN and VON trials and mechanical ventilation in neonates. It is well-established through randomized controlled trials that administration of surfactant in RDS decreases mortality.2 Thus, the current recommendations are administration of surfactant shortly after birth in preterm infants with RDS.1 Following initial studies showing improved outcomes with rescue surfactant administration, subsequent trials reported improved outcomes with prophylactic or early administration of surfactant.3,4 Meta-analysis of early surfactant studies supports the use of early surfactant in preterm infants (< 32 weeks gestation) with minimal time on mechanical ventilation.5,6 Most of these trials, however, did not provide NCPAP as default to infants who were randomized to the no surfactant group. Early surfactant results in fewer pneumothoraces, less pulmonary interstitial emphysema and less BPD than in patients receiving late selective surfactant.6,7 Mechanical Ventilation & Lung Injury Mechanical ventilation in preterm infants with RDS as a result of surfactant deficiency results in lung injury.8 Because administration of surfactant decreases morbidity, the concept of intubation for surfactant administration and rapid extubation to avoid prolonged mechanical ventilation has been studied. Intubation and rapid extubation (INSURE) randomized controlled trials showed shorter duration of ventilation and fewer pneumothoraces as compared to the late selective administration of surfactant.9 Preterm infants who have been intubated for surfactant may not always be extubated rapidly and thus sustain lung injury from prolonged periods of mechanical ventilation. NCPAP Nasal continuous positive pressure ventilation (NCPAP) may prove to be an even less invasive form of respiratory support in preterm infants based on animal studies. NCPAP delivers continuous flow via nasal prongs or masks delivered by a bubble CPAP or a ventilator. Use of intermittent ventilation delivered by the ventilator has not shown to provide any benefits compared to regular continuous NCPAP.10 None of the initial surfactant trials tested NCPAP as the respiratory support mode in the control group. Positive NCPAP Trial Results Recent trials of early initiation of NCPAP in preterm infants with RDS show promising results.11 The Surfactant Positive Pressure and Pulse Oximetry Randomized Trial (SUPPORT) conducted by the NICHD Neonatal Research Network compared NCPAP initiated in the delivery room with intubation and surfactant administration within the first 60 min after birth in 1316 extremely preterm infants.12 The NCPAP group had stringent requirements for intubation for surfactant administration and both groups were managed with a ventilator weaning protocol. The SUPPORT trial showed a trend for reduction in death or BPD at 36 weeks (47.8%) in the NCPAP compared to the surfactant group (51.0%). In the 24 to 25 weeks gestation infants, there was a significant reduced mortality in the NCPAP group (23.9%) compared to the surfactant group (32.1%).12 The trial of the Australasian Trial Network compared the effectiveness of NCPAP to intubation and mechanical ventilation (COIN Trial: CPAP or Intubation) in preterm infants who were breathing spontaneously at five minutes of life.13 Similar to the SUPPORT trial, the COIN trial showed a trend toward lower rates of death or BPD and a shorter mean duration of ventilation in infants who received CPAP.13 The Vermont Oxford Network Delivery Room Management Trial (VON DRM Trial) assigned 26-29 week gestation infants randomly to one of three treatment groups: Prophylactic surfactant and continued ventilation, prophylactic surfactant and extubation to CPAP, or CPAP alone without surfactant.15 There were no significant differences between the three groups. Prophylactic CPAP A meta-analysis comparing the use of prophylactic surfactant versus prophylactic stabilization with CPAP and selective administration in extremely preterm infants with RDS showed that prophylactic CPAP reduced the incidence of death and BPD.3 Evidence from these trials supports the use of early or prophylactic CPAP and does no longer support the benefits of early or prophylactic surfactant administration in these infants.3 Conventional & High-Frequency Ventilators Conventional and high-frequency ventilators are used in neonates. Conventional ventilators deliver either intermittent mandatory breaths (CMV) or are synchronized (SIMV) with the patient own breaths. High-frequency positive pressure ventilation (HFPPV) provides low volume breaths at a very high rate. Neither HFPPV nor SIMV have been associated with a reduction in the incidence of BPD.16 Synchronized Ventilation Synchronized ventilation compared to CMV has been shown to result in a shorter duration of ventilation. A meta-analysis finds that the use of HFPPV reduces the risk of air leak.16 Individualized patient care is important with a goal of providing gentle ventilation. When mechanical ventilation is necessary, infants should be weaned aggressively based on permissive hypercapnia on the ventilator. The SUPPORT trial set a goal of extubation within 24 hours once extubation criteria were met. Infants in the CPAP group who were receiving ventilation were to be extubated once they met all the following criteria: PaCO2 below 65 mmHg with a pH higher than 7.20, an SpO2 above 88% with FiO2 below 0.5, a mean airway pressure below 10 cm of H2O and a ventilator rate of less than 20 breaths per minute.12 Implementation of stringent weaning and extubation criteria is important to transition to less invasive forms of ventilation such as NCPAP or oxygen. New Evidence Recent evidence supports the strategy of treating preterm babies with RDS with CPAP immediately after initial stabilization after birth with subsequent selective surfactant administration as an alternative to giving surfactant early. Infants who are treated with early NCPAP are at reduced risk for death and BPD. These studies also reassure us that preterm infants treated with early NCPAP who receive delayed or no surfactant administration are not at increased risk for adverse outcomes. The awareness of these data is essential for the experienced healthcare giver and meticulous respiratory management from birth on is essential in the prevention of morbidities. Rune Toms is assistant professor, University of Alabama at Birmingham, and medical director, Division of Neonatology, Neonatal Cardiac ICU, UAB Health System; and Wally Carlo is Edwin M. Dixon Professor of Pediatrics, University of Alabama at Birmingham, director, Division of Neonatology, and director, Newborn Nurseries, UAB Health System.