Lancashire Teaching Hospitals
NHS Foundation Trust
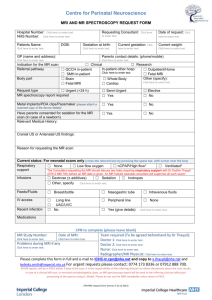
MRI Imaging Department, Royal Preston Hospital, Sharoe Green Lane, Fulwood, Preston PR2 9HT
MRI Appointments Tel 01772 522014
G.P REFERRAL FOR NON URGENT MRI SCANS OF THE KNEE
SURNAME ( BLOCK CAPITALS )
FORENAME(S)
DATE OF BIRTH
ADDRESS
POSTCODE
TELEPHONE
HomeMobilePREVIOUS RELEVANT
EXAMINATIONS
NHS NUMBER
PLEASE CHECK IF ANY OF THE FOLLOWING CONDITIONS APPLY TO THE PATIENT AS EXCLUSIONS WILL
APPLY OR CARE IS REQUIRED WHEN REFERRING
SCAN CONTRAINDICATED FOR ANY OF THE BELOW
CARE REQUIRED FOR ANY OF THE BELOW
Patient can be referred but please provide further information
Cardiac Pacemaker SCAN CONTRAINDICATED
Cochlear Implants SCAN CONTRAINDICATED
Neurostimulators
SCAN CONTRAINDICATED
Intracerebral Aneurysm Clips
Artificial Heart Valves
Metal Implant/fragment in eye/body
Information
DIRECT REFERRAL- EXCLUSION CRITERIA MRI KNEE
If any of the criteria below apply to the patient- DO NOT REFER- consider clinic referral
Is the patient < 15 years or > 60 years old?
Are there signs of active inflammation?
Is this a recent acute/severe injury?
Does the patient have severe OA?
Is the knee locked?
Has the patient had previous meniscal surgery?
Is the patient pregnant?
DIRECT REFERRAL- INCLUSION CRITERIA MRI KNEE
Symptoms present in right or left knee?
Right
Left
Does the patient have signs and symptoms of meniscal tear?
If 'yes' to signs of meniscal tear, are they medial or lateral?
Does the patient have signs or symptoms of knee instability?
Please describe symptoms including nature and duration:
What is the probable nature of the pathology in your opinion?
Date of referral:
GP SIGNATURE
GP NAME please print
PRACTICE NAME AND
ADDRESS
Yes
No
Medial
Lateral
Yes
No
Tel Number:
Please provide a contact
number, we may need to call
you to clarify some details or
to confirm patient safety
PLEASE REFER TO DIRECT ACCESS REFERRAL GUIDELINES FOR CLARIFICATION
OFFICE USE ONLY
RECEIVE DATE
 0
0