click here
advertisement

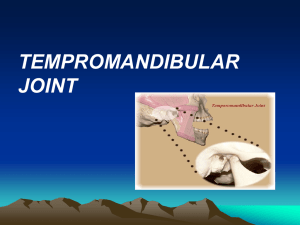
The following description of the TMJ is complements of Dr. Mark Piper: The condylodiscal ligaments are intracapsular support structures that are responsible for maintaining the general posture of the disc superior to the condylar surface. These ligaments occupy the medial and lateral poles of the mandibular condyles, and they blend with the fibrous connective tissue of the medial and lateral portions of the disc. These ligaments are not weight-bearing structures. However, they play a vital role in maintaining the disc in proper alignment at both poles. Furthermore, these internal ligaments must remain tight enough to tether the disc, but at the same time, they must have enough laxity to allow the disc to assume a more posterior relation with respect to the condyle during forward translation. Like other ligaments, if the joint is hyperextended, these structures must hold up to these forces. Finally, although the condylodiscal ligaments function in harmony to hold the disc in alignment, they are independent structures and are functionally distinct. Hence, they may break down independently. The articular disc starts out as a biconcave structure composed primarily of dense fibrous connective tissue. The disc generally is divided into thicker posterior and anterior bands with a thinner mid-portion that will take the greatest compressive force from the adjacent osseous surfaces. At the periphery, the disc has some vascular networking. This anatomic arrangement allows the disc to lock onto the underlying condyle during compressive loading. Furthermore, as the condyle translates anteriorly during normal function, the perimeter of the disc can make immediate adjustments in relative thickness by minute changes in vascular shunting. This will allow the disc to remain in a stable relationship over the mandibular condyle while simultaneously changing its relative thickness on the anterior and posterior bands to match the space available for it between the condyle and fossa or between the condyle and eminence. Thus, as the relative space between the bony structures changes, the disc can make appropriate adjustments in its thickness, at least at the perimeter. The consistency of the disc is such that it is somewhat pliable, yet still firm enough to compress against adjacent articulating structures for participation in normal synovial nutrition. Furthermore, the disc will be dependent on synovial fluid compression for its nourishment in the midportion. Because of the relative limitation of the depth that synovial fluid will penetrate, this mid-portion must remain between one and three millimeters in thickness. At the periphery, the disc can receive nutrients both directly and indirectly from the synovial fluid and directly from its own blood supply. Discal positioning over the superiorly seated condyle should have the posterior band just proximal to the mid-fossa. In this relation, any compressive forces from the mandibular condyle will tend to lock the disc into this posture. Furthermore, the disc must retain this relative position just proximal to mid-fossa on both the medial and lateral poles. As long as this relation is maintained, a superiorly compressed condyle cannot slip posterior to the disc, because of the locking forces generated by the posterior band over the top of the condyle. During forward translation of the mandibular condyle, the disc will rotate more posteriorly in relation to the condyle, and the condyle will slide closer to the anterior band of the disc as these structures reach the level of eminence. At this forward posture, the shunting of blood out of the anterior band of the disc will allow this area to compress, and the shunting of blood flow into the posterior band will cause the area to thicken in order to fill the gap intervening between the posterior slope of the condyle and the proximal slope of the eminence. Finally, the proper positioning of the disc within the articular space will allow the adjacent intrarticular hard and soft tissues to perform their individual physiologic functions, as will be explained subsequently. The lateral pterygoid muscle has upper and lower bellies that are separated by the epimysial tissue. The upper head originates from the infratemporal surface of the greater wing of the spheroid bone. The lower head originates from the lateral surface of the lateral pterygoid plate. Insertion points for the upper head are both into the disc through an orifice of the external capsule as well as into the upper part of the fovea of the anterior part of the condyle. The inferior belly inserts entirely into the anterior neck of the condyle. The upper and lower bellies have distinctly different electromyographic activity. On mandibular opening, the inferior head contracts and the superior head maintains resting activity. On closure of the mandible, the superior head contracts while the inferior is at rest. Functionally, then, it is the superior head that may influence discal position. Hence, because the superior head inserts both into the condyle and into the disc, it is felt to function by making rapid adjustments in the relative positioning of the disc and condyle during closure. Thus, the relative alignment of the disc over the condyle becomes more than merely mechanically dictated by the shape of the anterior and posterior bands of the disc, and it may, in fact, be under more precise neurologic control by the central nervous system. Muscles function by moving the insertion point closer to the origin. Therefore, in the TMJ, the condyle and disc will move anteriorly and medially toward the infratemporal fossa and lateral pterygoid plate when the lateral pterygoid muscle is in a foreshortened state. The most common form of muscle foreshortening is through contraction. In fact, all muscles have underlying electrical activity that allows an average number of myofibrils to be contractile at any point in time. This defines a "resting length" of the muscle. However, the resting length of a muscle is also defined by the laxity of its fascial tissues. The upper and lower bellies of the lateral pterygoid muscle each have an outerconnective tissue layer of epimysium and perimysium, and collagenous septa divide the muscle fascicles. The reticular layer around the individual muscle fibers makes up the endomysium. All muscles must on occasion be stretched in order to maintain the laxity of fibrous connective tissue layers. Before leaving the muscle, it is important to consider the vascular network that feeds the lateral pterygoid muscle as well as that blood supply that courses through the muscle. The maxillary artery arises from the external carotid artery and immediately gives rise to feeder vessels into the inferior half of the lateral pterygoid muscle. More anteriorly, the maxillary artery initially lies superficial to the inferior belly; toward the origin of the muscle, the artery dives between the two bellies. Therefore, anteriorly, the artery will eventually supply branches to the pterygopalatine fossa. More posteriorly, there are two important dependent areas of maxillary artery blood flow. Crossing first inferiorly and then medially to the lateral pterygoid is the middle meningeal artery in its extracranial course just before it enters the foramen spinosum at the medial part of the articular eminence of the TMJ. Hence, patency of this vessel may be influenced by the posture of the TMJ structures. Second, the posterior blood supply from the maxillary artery must also eventually perfuse at the mandibular condyle. Those branches that perfuse the head of the condyle course through the superior belly of the lateral pterygoid muscle and perfuse the cortical bone to supply the underlying marrow. The neck of the condyle receives its blood supply from vessels that must pass through the upper and lower bellies of the lateral pterygoid muscles. The synovial tissue of the TMJ is the internal lining of the external capsule. Thus, one would normally expect to find synovial tissue at the periphery of the joint. Generally, it is accepted that synovial tissue may be of several types, depending on what intraarticular tissue it covers. For example, most joints have loose connective tissue, dense fibrous or an adipose type of synovial tissue. Therefore, that part of the synovium that rests on the non-articulating retrodiscal attachment would be of the loose connective type. More fibrous synovial tissue would be found around the medial and lateral condylodiscal ligaments and the tendinous insertion of the upper belly of the lateral pterygoid muscle. Where villi of synovial tissue project into the joint space from the perimeter, there usually is fatty tissue in the stalks of the villi, and this is classic adipose synovial tissue. Larger villous folds will be found to contain blood vessels. The synovial fluid is generally a dialysate of blood that also contains mucin, lymphocytes, monocytes, and macrophages. The non-vascularized tissues of the joint are dependent on synovial fluid for nutrition. Hence, the thinner mid-portion of the disc and the articular cartilage covering the condyle, fossa and eminence are dependent on the pumping of synovial fluid. As in most other synovial diarthroses, the synovial fluid must be compressed by the articulating surfaces and thereby be driven into deeper layers of these tissues. Thus, the mechanism of synovial nutrition in the TMJ is dependent on three factors. First, the disc must be compressed against the adjacent articulating surfaces in normal juxtaposition between the condyle and the opposing superior osseous structures. Second, there must be compressive loading of structures against each other, and the articulating structures must be firm yet pliable enough to drive the synovial fluid into the tissues effectively. Third, the tissue being penetrated by synovial fluid must be relatively thin. Thus, the thicker anterior and posterior bands of the disc will have their own internal blood supply. Additionally, in most synovial joints, the intra-articular cortical bone is nourished at least in part by synovial fluid. The retrodiscal attachment tissues are the intra-articular part of the joint posterior to the condyle and disc. Functionally, this statement pertains to whether the condyle and disc are seated in the fossa or whether in fact they are seated more anteriorly. Hence, this tissue must have a volume that is very strictly defined when the condyle and disc are in centric relation, and this volume must increase instantaneously when the condyle translates anteriorly. Thus, there is a rather prominent vascular shunt in the upper part of the retrodiscal attachment, and this vascular network is contained within loosely organized fat, collagen and elastin. Perhaps because the disc tends merely to rotate against the condyle (as opposed to translating, as the disc does against the upper articular surface), there is a need for the disc to be tethered to the condyle posteriorly. Hence, there is a stratum at the interior portion of the retrodiscal attachment that is composed of relatively inelastic and tightly packed collagen. In fact, this interior stratum of collagen blends medially and laterally with the condylodiscal ligaments, and functionally, this inferior stratum may be considered a separate ligament structure that must maintain a certain length to keep the disc and condyle in proper alignment. One cannot consider the synovial fluid without also defining the normal spaces of a joint. An open space must be maintained in both the upper and lower joint cavities so that synovial fluid can access the intraarticular structures for nutrition and lubrication. Ultimately, the superior space will be bounded by the attachments of the articular capsule medially, and laterally by the origination of the retrodiscal attachment posteriorly, and by the blending of epimysium, capsule and periosteum anteriorly. The capsule is primarily a medial and lateral joint structure. Medially, it will generally course along an area approximating the squamosphenosal suture line. Laterally, the capsule will originate from the inferolateral edges of the fossa and eminence. In the anterior of the upper joint cavity, the space will be limited generally to the eminence at its most prominent portion or slightly, onto the anterior slope of the eminence. This reflection comprises a blending of epimysium with the periosteum of the anterior eminence through an orifice of the capsule. As such, this boundary is usually obliquely oriented medially and anteriorly. There is no true capsule in the posterior portion of the TMJ. Therefore, the posterior boundary is limited by the posterior and superior origin of retrodiscal attachment. This tissue generally originates just anterior to the squamotympanic and petrotympanic fissures. The inferior joint cavity is bounded medially and laterally by the insertion of the medial and lateral collateral ligament onto the condylar surface. Anteriorly, this cavity is limited to the blending of capsule and tendon between the part of the superior belly of the lateral pterygoid muscle that inserts into the disc and the part that inserts into the condyle. Posteriorly, the retrodiscal tissues normally blend with periosteum approximately 10 mm down onto the neck of the mandibular condyle. The fibrocartilage covers the intra-articular osseous surfaces. This tissue is therefore entirely dependent on synovial fluid for its nourishment. Furthermore, the joint must be free of adhesions so that the synovial fluid will have access to the articular cartilage. This tissue is generally thicker on the loaded portions of the joint surfaces. There is greater thickness of fibrocartilage on the anterosuperior condyle and on the proximal slope of the eminence. Likewise, it is these areas that receive the primary compression during normal joint movement, and hence as synovial fluid is driven into these surfaces, a thicker tissue layer can be maintained. The osseous elements of the TMJ are the condyle, fossa and articular eminence. The mandibular condyle forms the inferior articulating structure and is the convex member of the joint. The condyle receives its nourishment from three sources. The most superficial part of the intra-articular cortical bone is nourished by synovial fluid. The part of the condylar cortex and marrow that is contained within the joint capsule is dependent on the perforating blood vessels from the insertion of the lateral pterygoid muscle for its blood supply. Those parts of the condylar head and neck that are extra-articular will receive a more direct blood supply from the periosteum and adjacent muscle tissues. Hence, the parts of the condyle that are most demanding of the blood supply are posterior and superior. Furthermore, the outflow of marrow blood is generally to more dependent parts of the cancellous bone, and if there is to be adequate blood flow into the condyle, there must also be equal flow of blood out through the condylar neck. The narrower the neck or the tighter the trabecular bone of the neck, the more vulnerable the condyle may be to venous outflow sludging. This blood will back into the arterial side, and a diminished condylar blood supply will result. The superior articulating structures are the fossa and the eminence. The fossa is the concave portion of the joint, and functionally, in all synovial joints, the majority of movements take place with the convex and concave surfaces in articulation. The fossa generally is wellvascularized extracapsularly by periosteal and muscular attachments, and blood supply is usually not a problem. The medial half of the fossa is beneath the middle cranial fossa, and in this area, the bone is quite thin. The articular eminence is part of the temporal bone and is convex from anterior to posterior. As such, this part of the articulation is not structured to function for long periods with the convex condyle. Even though the disc is normally interposed, the two convex surfaces will have one point of contact that will overload the joint locally as these areas. This, in turn, could result in osteochondritis dissecans and localized collapse of these areas. It is not infrequently found that mastoid air cells extend into the eminence and as such pose a potential communication between the joint and the mastoid sinuses. Again, the blood supply to the eminence is generally favorable because of the abundant adjacent muscle attachments. Of one final note is the potential occlusion of the middle meningeal artery with antecomedial displacement of TMJ structures. The last tissue to be considered is the articular capsule. The attachment points of the capsule have already been discussed. It is important to realize that this capsule is an incomplete structure. That is, the capsule does not extend posterior of the condyle. In fact, the posterior part of the TMJ is bounded by the tympanic plate on the medial twothirds of the joint and by external ear cartilage on the lateral third. On the lateral part of the joint, the capsule is a well-defined structure that functionally limits the forward translation of the condyle. This capsule is reinforced more laterally by an external TMJ ligament, which also limits the distraction and the posterior movement of the condyle. Medially and laterally, the capsule blends with the condylodiscal ligaments. Anteriorly, the capsule has an orifice through which the lateral pterygoid tendon must pass. This area of relative weakness in the capsular lining becomes a source for possible herniation of intra-articular tissues, and this in part may allow for forward displacement of the disc.