Crittenton Hospital Medical Center * Quality and Outcomes
advertisement

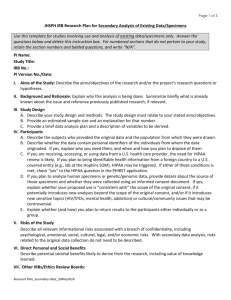
Project Request Form Wayne State University / Crittenton Hospital Medical Center This form must be completed and processed BEFORE any work on the project begins. Project Title ____________________________________________________________ Type of project (circle one): Quality Improvement Research Quality Improvement Project Problem Statement/Aim:(what is the problem you Research Project Hypothesis: What PDSA tools do you plan to use for this project? Describe efforts to research and learn previous studies on this topic currently see? – DO NOT include any solutions) Which hospital initiative(s) does this project align with? Date of Request ______________________ Data Needed by_____________________ Requestor __________________________ Department _________________________ Phone ____________________________ Email _____________________________ Quality Improvement Project Research Project Description of data needed: Background supporting method of testing hypothesis and describe what data you want to collect and analyze Type of data (circle one): What procedures will you use to collect data? Root cause analysis Process measure Outcome measure Date Range of Data to be included _____________to_____________ Codes to Include (circle one or more and specify below): DRG ICD-9 CPT-4 **Contact Medical Records to determine specific codes needed** Page 1 of 2 rev. Oct 2014 Other Data Fields to be Included (circle one or more): FIN Patient Name Dates of Service LOS Patient Age Attending Other: Data will be provided in Excel format The project has been presented to the Task Force for Quality Improvement and agreed to be a (circle one) Quality Improvement Project / Research Project. Date Reviewed: ___________________ QI Project Sign Off: The data being collected for this project is being used as part of a process improvement initiative and not a research project. I understand the data may contain patient identifiers and have reviewed the CHMC HIPPA Administrative Requirements policy. Any identifiers given will be used to find the root cause of the problem, measure the process, and/or the outcome of the process change. It is my responsibility to delete/remove patient identifiers from the data set. I certify I will delete identifiers 14-01_administrative from the data set after collecting information. _guidance_policy_(hipaa)_-_ Requestor Signature: ________________________________ Date: _________________ Program Director:__________________________________ Name Printed Signature: ________________________________________ Date: _________________ Quality and Outcomes Department Sign-Off _______________________________________________ Date: __________________ Lisa Takis – Quality and Outcomes Manager Research Project Data Recipient Sign Off: I understand that I have been provided with patient identifiers for the sole purpose of retrieving information. It is my responsibility to delete/remove patient identifiers from the data set. I certify I will delete identifiers from the data set after collecting information. Requestor Signature: _____________________________________ Date: _________________ Program Director:________________________________________ Name Printed Signature: ______________________________________________ Date: _________________ Page 2 of 2 rev. Oct 2014