February 2014 - Retina New Zealand
advertisement

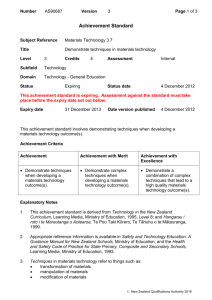
Retina NZ Newsletter February 2014: From the Editor ....................................................................................................................................... 1 From the President’s Desk ...................................................................................................................... 2 Audio described theatre in Auckland...................................................................................................... 3 Retinal laser therapy ............................................................................................................................... 5 Trevor Plumbly: Independence Day ........................................................................................................ 6 Inherited retinal disease database.......................................................................................................... 8 Meet a member: Donald Hunt .............................................................................................................. 10 3D Printing and disability ...................................................................................................................... 11 Glare and your sunnies ......................................................................................................................... 12 Personalised medicine .......................................................................................................................... 13 Gyles Baskett: The Great Schism .......................................................................................................... 15 Regional news ....................................................................................................................................... 16 Mailbag ................................................................................................................................................. 17 Retina NZ details ................................................................................................................................... 18 From the Editor Happy New Year! I hope you’re all enjoying the Summer so far, it’s definitely less intense than last year’s drought, but there have been some pleasant scorchers here in Auckland. In this issue we look at accessible theatre, 3D printers, genes, lasers and… data. Having worked with databases for ten years now, I’m no stranger to the meticulous eye for detail that dealing with data requires. Working with them in the museum and gallery sector means that I’m aware of how ‘rich’ datasets are everything. The back offices of museums and galleries echo with the disappointed belly sighs of people who find the appropriate entry for an object in the database (eureka!), only to find the entry says ‘Painting, by anonymous’ with no year of acquisition, no donor or artist details, nor any production information. A good museum database record is enormously rich, providing all possible clues and a long history of the object’s life before the museum and since it arrived. Your local museum will have a room full of people attempting to fill in the blanks; it’s interesting but repetitive work. In this issue we look at databases for our genes, which also need to be filled in adequately – it’s not simply a bank of numbers or a list of blood tests and swabs. Also on the scientific and technology front, this issue has a look at personalised medicine. If I were to name a home office appliance that I thought might change our lives in the coming years, I doubt I would have considered my aging bulky grey printer. However, after reading that a team of scientists at Cambridge have just printed out two types of rat retina 1 cells using a piezoelectric inkjet printer, I am seeing my printer in new light. Printing them out is one thing, but making them work inside our eyes is another issue entirely. However, the cells are viable after the printing process, and they plan to move on to trying rods and cones next. From topics as dry as databases and printers exciting and creative things can emerge. I hope you find the issue interesting, and please get in touch with me with any feedback or ideas for what you would like to hear about during 2014. Zoë Hill Newsletter Editor From the President’s Desk 2014 is now a month old and scanning my email inbox suggests to me that this is a year of opportunity that promises progress in areas related to our mission. In peer support we are re-writing “Your Blue Book” (to keep pace with technology changes and assistance structures), Retina Youth reaches out to more people every month, and in our quest to support the search for effective treatments we are strengthening our Scientific and Medical Advisory Board (SMAB) and pursuing fundraising for research. In our public awareness work we will hold our first public meeting in New Plymouth in March. I recently upgraded my work software systems and experienced the normal little frustrations. I was asked by the IT guy if digital systems were getting easier for blind people. As the range of tasks I’m unable to do progressively decreases, my first instinct was to say “easier, much easier”. Because I’d worked with the team for around five years, I thought I’d reverse the question: “you work with me, what would you say on this topic”. His answer was “no change really”. I guess our expectation changes and the difference between reality and expectation does not. The real challenge of course is how we impact positively on the general perceptions of the capabilities of blind people in the digital world. Last year an IT guy enquired as to whether the person who operated my computer was available, on the assumption that I didn’t actually operate my PC independently! This stresses the importance of public awareness work that is largely done voluntarily by blindness consumer organisations like Retina New Zealand. In my view, it also highlights the fact that we should take our personal advocacy responsibilities seriously. In promptly making our IT service aware of screen reading systems and some of them taking up the offer to briefly trial some voice synthesis options, their perceptions changed instantly and forever. It took just one email, one minute of my time. As I write this, I’m thinking the author of the book I’m currently reading would likely have an appropriate quote for this and he did: “Success is stumbling from failure to failure with no loss of enthusiasm.” ― Winston Churchill 2 And the brilliant work of the great man that I’m currently reading? “A history of the English speaking Peoples”. It’s four volumes and spans nearly 2,000 years but completely worth staying the ultrathon distance from all accounts. Happy summer days, Fraser Alexander President Audio described theatre in Auckland By Zoë Hill The Signal programme at The Edge (home of the Aotea Centre, The Civic Theatre, Auckland Town Hall and Aotea Square) offers audio described and signed performances to blind, partially sighted and deaf theatre goers. It is just one of many groups or individual theatres around New Zealand who are offering such services. I caught up with Nolwenn HugainLacire, current co-ordinator of the programme, to ask her how the service was going. How long has Signal been in operation at The Edge? The Signal programme was launched in 2011 with an audio described performance of Miss Saigon and a sign language interpreted performance of The Brothers Size by Silo Theatre. Why was Signal started? There were two reasons why this programme started. The first, and most important one, was recognition that there were people in the wider Auckland community who weren’t able to be audience members here because we simply weren’t providing the facilities for them to be able to do so. Obviously, that’s far from an ideal situation. Secondly, Bronwyn Bent, Producer of Foundation Programmes at The Edge, was the driving force in getting the programme up and running. Bronwyn had worked on audio described and sign language interpreted shows in the UK, and knew what great experiences they provided for audiences, cast and crew. She also knew we would be able to do at least a little of that here in Auckland too. How did Signal develop in the early days; what organisations in the disabled community did you liaise with? In 2009, Bronwyn started meeting with a few key groups, including the Blind Foundation and Deaf Aotearoa. They gave valuable advice, especially in regards to how we market shows to audience members who may not have ever been to a show. The Edge’s existing budgets were explored to find money which could be used to employ a programme coordinator who could make it all happen. After the initial consultation with the various communities, Stephanie Clarke was employed in February 2010 to set up and co-ordinate 3 the Signal programme. Stephanie had previous experience running a similar programme at the Bristol Old Vic, a producing theatre, which meant she knew what needed to be done in order for it to run successfully in Auckland. How do you choose which productions are suitable? We would love to have all our shows, big or small, audio described and sign language interpreted, however the budget doesn’t always stretch. We receive a small amount of funding annually, and as with any budget we are limited to the number of sign language interpreted and audio described performances we can support. The average cost to put on an audio described performance was initially around $3,000. In 2012, we purchased our own equipment which reduced our costs to around $2,000. The other ongoing issue is lack of audience. The first Signal performance was in 2011 and the vast majority of potential audiences are still unaware of what audio description is. To overcome hurdles such as cost and reaching out to the target audience effectively, we are first and foremost supporting main stream productions. Each audio described show also has a touch tour, during which the audience can come up on stage and touch some keys elements of the set or costumes. Is the price for an audio described performance different to normal ticket costs? For each Signal performance, we try to provide some discount tickets. However, it depends on the company support for this and so there specific rule. The Edge is currently providing the sole budget for Signal, however our goal is to be able to work more closely with companies to broaden what we are able to offer. Are you aware of what other theatres in NZ are doing for disabled audiences? Is there knowledge/resource sharing between organisations or cities? Arts Access Aotearoa is a national organisation following each venue and creating the link between them to be able to share our experiences and resources. How successful has Signal been? Have you attracted the audience you targeted? We run feedback sessions with staff and Signal patrons, and then make tweaks to the programme. For example, when we first offered audio description we received feedback that the sound quality wasn’t very good. This led us to finding a new provider and the problem was solved. Our evaluations show that people who have been to a performance come back again. At the moment we’re evaluating how we’re reaching people and are in discussion with the communities about the best communication channels. As well as signed and audio videos, we are using specific logos to identify the service we’re offering. Last November we completed our first musical and it was a real success. We had great feedback from our patrons and we had about 25 visual impaired patrons. This attendance 4 and feedback encourages us to continue to develop the programme. What have been the challenges in setting up Signal? Getting companies on board: Given that the service was in its infancy, most companies had a lot of concerns that needed addressing. Among the main concerns were the cost and resources required, plus the impact the programme could have on their existing patrons. Getting the equipment: It’s important to have good-quality transmitters and receivers for the audio description so the experience for patrons is really positive. This was achieved through feedback, and trial and error. I am looking for funding for us to buy our own equipment, which would significantly reduce the cost of each performance. Training the interpreters and describers: There is no specific training in New Zealand for the describers and sign language interpreters to specialise in theatre. After training an audio describers team the past few years, we are now focusing on the sign language interpreters. We are running a theatre interpreting workshop this month, which is really exciting! Arts Access Aotearoa are holding an audio description workshop in March, does this reflect the growing interest in providing services for the disabled in this sector? This is really positive. I think that theatres are realising that it is possible and they can learn from each other and be less apprehensive about providing such a service. Link to the Signal programme: www.the-edge.co.nz/signal Retinal laser therapy By David Worsley and Zoë Hill David Worsley, a retinal specialist at Hamilton Eye Clinic, is one of 20 ‘initial users’ worldwide of a new therapy for macular degeneration. Nanosecond retinal laser technology is a breakthrough new treatment that may reduce the risk of vision loss from early macular degeneration. It is the only laser of its type in New Zealand, and is a product of Australian eye disease medical technology company, Ellex. The laser delivers a dose 1/10,000 of the power of conventional retinal lasers. The low power dose stimulates the retinal pigment epithelium (RPE) without any damage to the overlying retina and without formation of laser scars. The ‘rejuvenated’ RPE clears soft drusen (accumulations of damaging waste products under the macula) from beneath the macula. Reducing or eliminating soft drusen is considered to significantly reduce the risk of progression to vision loss from advanced macular 5 degeneration, either wet or dry. In many patients clearing drusen also improves their central vision. Soft drusen are an early feature of macular degeneration, and are the highest risk factor for progression from early disease to advanced disease with significant vision loss. Until now the only strategy to slow progression of early disease has been diet and supplements. Published results show that by six months after laser treatment: drusen are decreased in 70% of eyes central visual function is improved in 50% of eyes there is no evidence of laser damage to the overlying retina Soft drusen before laser treatment: Soft drusen after laser treatment: Patients with dry macular degeneration and soft drusen may be referred by their optometrist or ophthalmologist for an assessment of their suitability for this new therapy. If you think you might benefit from this treatment, please speak to your local optometrist or ophthalmologist to check suitability. For those living outside the Hamilton area, information can be sent to suitable patients beforehand, and usually everything can be done on one visit. Follow up can usually be arranged locally. The cost of assessment for suitability is roughly $300, depending on how much investigation is required, and the treatment itself is $980. Copies of an information sheet are available from marwyn@hamiltoneyeclinic.co.nz Trevor Plumbly: Independence Day For 'Normals' (non Blindies) running out of milk and bread isn't really that big a deal, they can hop in the car or just pop up to the nearest dairy. To be honest it wasn't that much of a problem for me either, despite the fact that Pam was away for a few days, my friendly local store was just a five minute walk away. However, for some inexplicable reason I decided to go to the supermarket. It may have been a rabid flash of independence, a yearning for 6 adventure, or just plain stupidity, but, cane in hand off I set to tackle the 20 minute walk to the local Countdown, and on reflection the name itself should have served as a warning of things to come. Off I set at the merriest clip a 70 plus body shoving a four foot cane could muster. I tackled the climb uphill without disaster, pausing briefly at the intersection to avoid an invasion of 'hoverers', I meandered gently down the hill with a distinct feeling that this independence stuff was a piece of the proverbial. Outside the supermarket I paused to formulate a plan of action. I could just stroll up to the checkout and ask someone to get the stuff… but what the hell! This was independence day so why take the easy route. Trolley or not? Taking a trolley to collect a litre of milk and a loaf of bread seemed a bit much, but the alternative was to tap up and down the isles, thanking hoards of 'hoverers' anxious to render my newly founded independence redundant. The cane, I decided, should be discreetly folded in the trolley to indicate an ability to cope rather than a subtle plea for help. Not being sure where exactly in the store the necessities were, I decided that an elimination strategy was the way to go. If I went up one aisle and down the next I was bound to find the stuff. I soon discovered that other shoppers were keen to give me a wide berth which seemed to suit us all fine, but the main problem was the 'specials'. To Blindies 'specials' are a supermarket’s answer to landmines, they create artistic little piles and pyramids of all sorts of overstocked or unsold goodies and plonk them in the middle of the highest traffic areas. In all modesty I feel I made good progress up and down those aisles, I passed all sorts of interesting gear, stuff that I might have been tempted by if I could have read the labels, but as time passes I tend to adopt the attitude that if I can't see it, it’s not going to be that important to me, unless it’s an approaching vehicle of course. I reached the dairy section without incident or injury only to find that the act of buying milk had become a lot more complicated since my last visit, there were literally acres of plastic bottles on display some with different coloured tops that obviously meant something to trained shoppers, but not to me. Light, Trim, Low Fat or Standard? More decisions. Independence day was starting to lose its appeal, and my hesitancy caused a bit of a trolley jam. Unable to decide, I grabbed the nearest bottle caring not if it contained Calci-Trim or weed killer. At the Bakery section I found that bread makers had joined the dairy folk in making life complicated, as I was faced with a bewildering array of Wholegrain, Farmhouse, Gluten-Free, Sourdough and far too many mystical offerings to make any sort of choice. Obviously it was time to quit this independence nonsense and leave Countdown to its own devices. I toddled home in a less adventurous frame of mind, stopping at my friendly local dairy where trolleys and 'specials' don't exist, and you can buy stuff without ulcerous deliberations. I don't regard this independence day a total failure, more of a hiccup and I assure you there will be others, of which of course, I will report accordingly. 7 Inherited retinal disease database By Andrea Vincent and Zoë Hill A registry for Inherited Retinal Disease and Optic Nerve Disease in New Zealand was established in 2009 by Dr Andrea Vincent in Auckland. Dr Vincent worked in the Genetic Eye Disease Investigation Unit at the New Zealand National Eye Centre, University of Auckland’s Department of Ophthalmology. She is the only qualified genetic ophthalmologist in New Zealand, and was able to establish and maintain the registry with support from the Save Sight Society, The Ombler Trust, and Retina New Zealand. The database incorporates detailed clinical information, imaging and genetic information, and will help improve our understanding of retinal disease and optic nerve disease. To date, over 400 patients and family members are enrolled, and data entry and recruitment is ongoing. Inherited retinal disorders and optic neuropathies (IRDON) describe a group of clinically and genetically variable disorders affecting the retina and optic nerve. These disorders are usually bilateral and progressive, resulting in degeneration of the retina or optic nerve (or both) with resultant loss of vision, although poor vision may be present form birth. Over 200 genes are implicated in the pathogenesis of IRDON, although not all of them are yet known. These disorders may occur sporadically, however many are familial, showing autosomal dominant, autosomal recessive, X-linked or mitochondrial inheritance. One of the most common causes of visual impairment is age-related macular degeneration, and recent work shows a strong underlying genetic component. So, why establish a registry? Determining the epidemiology, incidence and degree of visual impairment data for NZ Identification of patients in the future, should gene-specific or disease-specific trials or interventions become available Integrated genetic information sharing for families throughout New Zealand A research resource for study of genotype-phenotype correlations (correlating the clinical findings with the genetic findings) Identification of individuals without known mutations, may permit novel gene discovery. Further research funding has been obtained from the Auckland Medical Research Foundation, and Fight for Sight UK to allow further investigation of unknown genes, with some promising early results which need further work. Improved health care Inherited disorders predominantly affect young individuals from birth, with subsequent progressive visual loss leading to blindness in many of those affected. As many of these will 8 eventually be registered blind, the support and rehabilitation required for these young individuals with visual impairment contributes to a significant social and economic cost in New Zealand, but there is not a lot of available data available to determine the exact prevalence and impact of retinal blindness. Identifying genes involved in the pathogenesis of these disorders provides opportunity to recognise novel therapeutic strategies, such as gene or gene-related therapies, that may cure or slow the progression of these disorders. It is important to realise that it is neither ethical nor suitable to just collect a DNA sample from a patient with inherited retinal disease in isolation. DNA is only one piece of the puzzle, and without all the other clinical information such as family tree, age of onset, electrophysiology, clinical appearance and progression with age, any DNA finding is meaningless. Anybody who contributes a DNA sample also needs to have an understanding of how their DNA will be kept and used, and face to face consent and discussion is vital in this situation. A number of patient’s have decided they do not want to go ahead with involvement in the registry after they have had the discussion, and it also important to realise opting out does not compromise their access to care of their eye condition. As Dr Vincent is the only qualified genetic ophthalmologist in New Zealand, all patients on the registry have been seen and examined by Dr Vincent. However, this does not preclude people from outside Auckland being involved. As a tertiary service, individuals from the rest of New Zealand can be referred to Dr Vincent at the Genetic Eye Clinic at Greenlane Hospital, Auckland by their current ophthalmologist, and the costs of travel should be covered by their own District Health Board. The genetic eye consultation, examination and gene testing costs are covered by the public health system. Some gene therapies are about to enter, or are already in, phase I, or phase II clinical trials. There are also a few phase III clinical trials underway. Treatment or participation in such trials may be able to be offered to a selected group of patients, but a prerequisite is identification of the underlying genetic cause. Having a database will give rapid access to details of patients and their mutations, thus enabling contact with them in the future to offer them these opportunities as they become available. Better knowledge Establishing a database of these disorders will help researchers in New Zealand to identify a unique local mutation spectrum in the NZ population. The individuals without identified mutations in known genes may provide the opportunity to determine new genetic mechanisms, or even novel genes involved in the pathogenesis of this group of disorders. Early results suggest there is a different mutation spectrum and disease causing genes in the Māori and Polynesian populations. 9 Meet a member: Donald Hunt By Zoë Hill If you’ve ever passed through the South Canterbury town of Waimate, chances are you’d remember the wide main street, fresh local strawberries, perhaps stopping at the Savoy tearooms for a lamington, or at the gardens to pat the Wallabies. Donald Hunt has lived most of his life in Waimate, and despite an early diagnosis of RP has raised his family and built a successful career there. As his Mother had RP as well, Donald knew from a young age that he would have to approach work differently to his peers, and by the age of 12 was already thinking ahead to possible self-employment options for his future. When he visited the local library, the local parks and reserves staff would leave examples of flowering plants in the foyer, which piqued Donald’s interest in plants, also supported by an actively gardening Dad and Grandfather. After he finished High School, Donald took up a five year apprenticeship in Gardening and Horticulture at Victoria Gardens in Waimate, and went on to work at the Timaru Botanic Gardens before returning to Waimate some years later with his florist wife, Rose, to manage a nursery and floristry. Managing a garden shop and nursery with decreasing vision presented many challenges, but Donald says the biggest challenge was access to information. Accessing information, writing receipts and the day to day running of the business obviously requires you to perform daily reading and writing tasks. Donald had lost 90% of his vision by age 40, and started using magnifiers, then illuminating magnifiers, then finally CCTV to help him conduct business. Glare was a bit of a problem when moving from the shop into the outside nursery, but spring loaded flip top sunnies helped with that! After joining the Blind Foundation and the Association of Blind Citizens at age 42, he soon had a talking book, and had learnt to touch type via a Blind Foundation correspondence course. Also on offer was cane training. After using a cane for about ten years, the Guide Dog Manager came and visited Donald at his business, and persuaded him to consider a Guide Dog. Initially reluctant because he only had half a mile to walk each way to work, Donald says it was ‘the best decision he made’, and 18 months later he had his first dog, Regan. Life with a dog brought more independence and mobility, and his current dog is a gorgeous Labrador, Nero (or, for guide dog genealogy tracers, Vero). Fast forward 32 years of volunteering and involvement with the Foundation and he is still the Chairman of the Waimate District Advisory Committee. He is a man of the community, with longstanding roles on numerous community boards. Donald still gardens and is in the enviable position for a blind person of being able to identify weeds by touch due to his career in horticulture. “I can tell chickweed from grass’ he says ‘because of how they feel different at ground level, and I can always find the stinging nettle”. He has four large raised beds for every kind of vegetable and some fruit trees, which he can prune by feeling out the 10 leader branches. Although he has lost all vision now, he navigates the beds easily and has his garden mind mapped, in fact he says he feels ‘more settled because I know what I can do and what I can’t.” Gardening whatever the light level is a blessing, and Donald can still be in the garden or turning the compost well after the sun goes down. He has witnessed a huge change in adaptive technology throughout his life so far, and says that accessing email and using JAWS made the biggest difference to him. When he was first diagnosed with RP by an Ophthalmologist in Timaru, a big wheel was used to do the field test. It had a dot in the middle and threads radiating out to the circumference, along which the Ophthalmologist would manually move a white bead. Considering Donald is about to have his first lesson on navigating the web beyond email using JAWS, it’s a huge leap in both science and technology. 3D Printing and disability By Zoë Hill It can be quite hard to think of what a 3D printer might be good for. Prepare yourselves, however, to hear a lot more about the 3D printing industry, as it has been predicted by a leading IT research and advisory company to grow 75% this year, with predicted consumer spending of US$133 million. With consumers buying 3D printers now, what on earth are they doing with them? 3D printing has exploded in the design community. At a consumer level, anyone can use a 3D modelling computer program to make a 3D design template, and then upload it to internet sites like Thingiverse (a community of amateur 3D designers) to share your design for other people to print out your objects using plastic and other material in special cartridges. The designs on Thingiverse are free, and free from copyright by using less restrictive ‘creative commons’ licenses. In late January, The Guardian published a list of things being made by 3D printers right now, and it’s dizzying reading. Fighter jet parts, prosthetic limbs, skin (which was successfully grafted onto mice), a six metre tall printer has printed a house in Amsterdam, horse shoes, jewellery, shaped chocolate and sugar structures, and musical instruments. It’s easier to imagine how this technology might revolutionise the manufacturing industry, but 3D printers are already also becoming a household gadget now they are dropping in price (you can buy one for under US$500). As the world tries to decide what it could 3D print, and more importantly, why it would want to, the technology seems to already pair easily with the disabled world. The rest of the world might be asking, ‘why on earth do I need all of my possessions to be that customised’, while many disabled people have required access to low cost ways to customise their day to day lives for a long time. 11 A few years ago a disabled man from Germany printed out his own customised ramp for his wheelchair – it was light and easy for him to carry around. At the time it cost under NZ$100 and took 26 hours to print out, which isn’t too bad for an emerging technology. In August last year a prototype of a white cane was uploaded to Thingiverse for people to use. It looks like something from a lego set (for starters, it’s bright yellow), however it’s easy to see the potential for consumers and manufacturers in this area. For some disabled people, customising and tweaking everyday household objects so they are easier to use is not a luxury but a necessity. Even though a cane is not very useful without training and support, it shows how the power to customise your world could be placed in the hands of those in need. As the BBC states in a recent article about 3D printing and the disabled world, “accessible equipment is often obtained from disability professionals or specialist shops. Many complain that these can be unattractive, costly and don't always work very well.. and can often be expensive as demand is relatively small.” For blind and partially sighted people, this technology could also open up the arts and science worlds. A student at Canterbury University here in New Zealand, Ellen Palmer, is working with 3D printing as she studies a Bachelor of Engineering and Science. She is keen to work with blind and visually impaired people in New Zealand to see how 3D printing might assist them. Ellen’s boyfriend is blind, and has had prosthetic eyes since he was very young. Ellen has designed and printed out a number of things so far, including some gears so her boyfriend could feel the intricacies of how they operate. Where this technology can really break down a traditional ‘no touching’ barrier is in museums and galleries. The Smithsonian Institution (made up of 19 museums and galleries, and nine research institutions) has a 3D digitisation lab. Instead of the old methods of making replicas of objects (which meant making plaster moulds and potentially damaging the object irreparably) objects are measured with lasers, and copies made available to be shared and printed out around the world. Let’s hope this technology hits its stride and is used to create a customised, helpful and more creative world. If you have any comments for Ellen Palmer, please contact her on keat333@gmail.com Glare and your sunnies By Zoë Hill Summer is always a good time to assess whether your sunglasses are still suiting your needs. I recently left my beloved sunglasses behind at a wedding, and after a short period of mourning, and headaches from using a backup pair, I decided to do some research before I reluctantly purchase a new pair. Retina Youth lead man Zane Bartlett recently purchased new sunglasses, and pointed me in the direction of the USA based company, NoIR Medical Technologies. You can choose your vision problem from a list on their website, and it details the right kind of lens for your sunglasses. Zane took this information along to his local sunglasses shop, found a helpful ear 12 of someone who could see what his needs were, and bought some great sunnies to suit his RP with added blue blockers. The Blind Foundation stock NoIR sunglasses, ranging in cost from $36 - $91 if you are not a Blind Foundation member and $20 - $64 if you are. They can be ordered directly from the Blind Foundation website (not all styles are pictured, so you might want to go try them on if you can). If you have access to a low vision clinic, they too will be able to provide you with assistance. Link to Noir Medical Technology site - http://www.noir-medical.com/ Link to Blind Foundation sunglass selection - http://blindfoundation.org.nz/product Personalised medicine By Zoë Hill The concept of more personalised medicine has been around a long time, and there is no singular definition; ‘precision medicine’, or the more straight forward ‘providing the right medicine to the right person at the right time’ are common. More officially, the National Academy of Sciences in the USA describes personalised medicine as ‘the use of genomic, epigenomic, exposure and other data to define individual patterns of disease, potentially leading to better individual treatment’. After hearing the term bandied about at a few Ophthalmology networking events, I decided to have a look at what it really meant. There have been many examples of personalised medicine in the news over the last few years, and it is becoming increasingly common to hear of drugs being released to people with a certain genetic sequence. In a recently released report (October 2013) from the USA’s Food and Drug Administration, details were included of four cancer drugs being approved in the past couple of years for use in patients whose tumours have specific genetic characteristics, plus a new therapy for use in cystic fibrosis patients who have a specific genetic mutation. However, personalised medicine doesn’t always mean identifying gene mutations individuals and making specific drugs for those gene carriers. In something of a sci-fi movie twist, a three-dimensional printer created a bioresorbable tracheal splint for a critically-ill baby last year. They took images of the child’s damaged airways, measured up the exact missing part, printed it out and inserted it. It then acted as a ‘placeholder’ while cells grew over it, leaving the area reformed satisfactorily after one year. After three years, the part will have been absorbed by the body. You can’t get much more ‘personalised’ than that. It’s easy to see from this example that advances in technology are propelling things forward in the world of personalised medicine, but it’s not the only factor allowing for the rapid advances. It’s been about ten years since the Human Genome Project was completed, which aimed to identify all 20,500 human genes, and determine the sequences of the 3 billion chemical base pairs that make up human DNA. After 13 years of work it was completed in 2003 and unleashed what the Food and Drug Administration called “an explosion of genetic information” into the scientific world. They state that “the tools of the last two decades have left us awash in data, yet we still have a relatively limited understanding of what it all 13 means”. In parallel to these developments, the computational power is now available to store and access huge amounts of data in new ways, and to interrogate and share that data. It sounds quite neat and straightforward to have completed the first mapping of the human genome, but it’s just the beginning. As New Zealand’s National Health Committee states in their 2012 ‘think piece’ on personalised medicine: “the range of mechanisms of disease at a genetic level is complex and our understanding continually evolving”. It might be less of a daunting task if one faulty gene equalled one disease, but as the committee describes “there are many different mutations that may lead to the same disease. This idea becomes more complex when we consider cellular communication pathways. Imagine you are in a traffic jam on a road with a number of traffic lights – it does not matter which of those traffic lights is faulty, the result is the same, your 15 minute commute now takes 3 hours”. The Food and Drug Administration report also identifies the challenges that still lie ahead. One example is outdated disease classification systems, which define diseases primarily by their signs and symptoms and “don’t easily accommodate emerging information about disease mechanisms, particularly when it is at odds with traditional physical descriptions”. Also ahead are the challenges of policies and procedures for handling the ethics of the personalised medicine era. As the National Health Committee point out, the areas involved are “(the) physician-patient relationship; privacy and prevention of discrimination; and public health”. So while the scientists are coming to terms with their classification systems and wrangling an explosion of data, how does it affect patients? It seems to be a very participatory era. Patients are part of this scientific progression and need to be involved in the process. As we all know, people are more complex than the sum of their genes, and it is the face to face learning that creates a full picture of the person and their disease. One organisation actively seeking out patients is Irish patient-led charity Fighting Blindness. They have a project called Target 3000 – Gateway to Vision. Speaking of exciting retinal research projects that are moving out of the research phase and into clinical trial phase, they say that “many of these therapies will rely on repairing the specific gene abnormality for each individual. This is why it is imperative that we identify the exact genetic profile of the estimated 3,000 people affected by a retinal degenerative condition in Ireland.” Samples collected from those who wish to be involved are tested and stored in laboratories at Trinity College Dublin. 14 They outline the entire process on their website and answer common questions, saying that “It is because of patients who volunteered in previous studies that we have today’s knowledge and understanding of retinal conditions, so it is vital that people with inherited retinal conditions join us now in this project”. As Target 3000 explains to prospective participants, the reason for doing this is that ‘knowledge is power’, and it is this knowledge of ‘who has what’ that can lead to clinical trials being performed on smaller groups of patients selected with more knowledge of what their particular disease mutation is. This leads to faster, less expensive trials, which is traditionally the most expensive phase of drug development. The Food and Drug Administration report also outlines all risks involved in the potential changes to clinical trials, and says “one implication of dramatically smaller pre-market exposure, however, is a general increase in the importance of and emphasis on post-market monitoring, because relatively rare adverse events, in particular, are unlikely to show up when a drug is being tested in a small population, but will arise when a broader population is treated." We are sifting through what puts us together, and revealing things at an alarming rate, more and more easily, and for less cost. The first human genome cost US$75 million to sequence, in 2012 it cost approximately US$5 – 10,000 to sequence, and predictions are that will ultimately cost less than US$1,000. The relationship required between patient and health care professional in order for this era to be fully realised will be interesting to watch develop. It is not as simple as taking a blood sample and swab and sending someone on their way, and organisations around the world involved in this work are considering ethics closely. As Hippocrates said “It’s far more important to know what person the disease has than what disease the person has.” Gyles Baskett: The Great Schism It’s like those religious seismic shifts: who will stay faithful to the world's most popular screen reader JAWS and who will break away to use MAC products. I can only relate my own experience and suggest to others that they carefully consider the options. I have used JAWS at an intermediate level for 20 years. The problem is that JAWS is both complex and expensive. It’s over $1,000 to get JAWS from the Christchurch dealer Pacific Vision, with further costs every few years to keep the software up to date in its capabilities. If you are prepared to spend the time in learning from the many well laid out tutorials that are free with JAWS, then it is a wonderful Internet tool. The problem for me is that when Windows version 8 was released the keystrokes I had become familiar with suddenly ceased to function and there are lots of new ones to learn. Every now and then I glance at a yahoo email chat list for JAWS users, where, if you have time, you can swim with the other users as they thrash about swapping solutions. Apple, with its built in ‘voiceover’ features, offers alternatives, and I have an iPhone 5. It is generally considered by the blind community that Apple has more consistently offered userfriendly access software for the non-sighted. You may need some help in setting up any Apple products with ‘voiceover’, whereas JAWS has a talking installation. In this short article 15 my goal is to alert you to some of the choices. If you have finance readily available, then this might tip the balance in favour of JAWS. For those with limited Internet requirements who require simple to use products, then I recommend Apple products. Both platforms can be equally challenging, however I feel you can enter the field slowly with Apple products, and if you have assistance to get started, then that is what I would recommend. My guess is that you will have more pleasure and less frustration! In summary, both systems have their fervent religious following, and both systems have their advantages. However, few of us have the time and money to worship at both churches, and I for one have found a renaissance of spirit as I take up the Apple creed. Yahoo List for JAWS Users: JAWS-Users-List Freedom Scientific Podcasts (host: Jonathan Mosen) for JAWS www.freedomscientific.com/FSCast/ JAWS dealers ‘Pacific Vision’ Phone +64 3 3765072 www.lowvision.com.au Apple advice: Jonathan Mosen http://mosen.org Regional news Retina NZ meeting in New Plymouth Retina NZ invites you to attend a meeting in New Plymouth. Any member of the public who has a sight loss issue is welcome to attend. Please spread the word! Guest speakers are Optometrist Philippa Charteris and Retina NZ President Fraser Alexander. When: Saturday the 22nd of March Where: Blind Foundation rooms at 131 Vivian St Time: 1.30pm – 3pm RSVP: Please phone 0800 560 869 Ext 2 for catering purposes. KAPITI: When: 3rd Monday of the month Where: Kapiti Community Centre About 30 people attended our shared lunch at the Kapiti Community Centre in the middle of December. The noise level suggested that it was a real meeting of old friends, and it was lovely to welcome one of the Kapiti VIPs founding co-ordinators, Gael Hambrook, who travelled out from Wellington with her guide dog to join in the fun and carols. The Kapiti VIPs kicked off their 2014 programme with a meeting in January where people shared hints and gadgets that made life easier for them. It is intended to have a speaker about Emergency Preparedness in February, in the light of recent earthquakes. We would 16 love you to become part of our fun-loving support group and answer your questions about living with low vision. Phone Elizabeth East to attend - (04) 299 1800. TAURANGA: When: 1st Saturday of the month, 10.30 till 12pm Where: Tauranga Library We've been meeting for just over a year now, it's been great to support each other and share ideas and handy hints. Please phone Sara Ash to attend - (07) 570 0917 DUNEDIN: When: 4th Wednesday of the month, 1:30pm Where: Dunedin Public Library, 4th floor Dunnington Suite. At our last VIP meeting for 2013, we launched VICTA's bright yellow, highly reflective wristbands ($10). These were created to help VIPs cross the road safely, but they're so gorgeous just about everyone who sees them wants a pair (cyclists, walkers, joggers, school kids, horse riders, disco dancers), so now we're helping keep all vulnerable road users safe. Our February meeting will feature a panel of partners and spouses discussing "caring for someone who is losing their sight." Phone Karen Manning to attend (03) 455 2207. HAMILTON: Saturday 22nd February 1.30pm - 3pm followed by afternoon tea. Phone Mike Smith to attend - 0800 569 849 (ext 3) Mailbag Garden Hint – Use of Contrast Makes It Easier To Be Independent. To make it easier to identify compost from potting mix or mulch , when you can no longer easily read labels, I have recently purchased some different coloured heavy duty plastic rubbish bins with clip on lids from a well-known hardware chain. I put the compost in the red one, the potting mix in the yellow one and the mulch in the black one. Since I did this three months ago it has saved me time as I have not had to struggle to guess what was in each bin, or wait for someone to help me. I have also purchased some hand tools which are bright orange and have found that when I 17 put these down I have been able to find them quite easily compared to my previous ones which were metal with wooden handles. Using these brightly coloured tools saved me lots of frustrating moments in the garden. - Elizabeth East Retina NZ details Editor: Zoë Hill (editor@retina.org.nz) Membership Officer: Petronella Spicer (membership@retina.org.nz) The opinions or position expressed in articles are the author’s own views and do not necessarily express the policy or views of Retina New Zealand Inc. What format of newsletter would you like? (Members may receive an email version in addition to either a print or CD copy at no extra cost) Email: If you would like to receive an email version please email your request to membership@retina.org.nz so that we can ensure we have the correct email address. CD or Print: If you would prefer to receive it as an audio CD or in large print please phone 0800 LOW VIZ (0800 569 849 Ext 2 or 4). Publications: A range of helpful brochures and books are available free of charge to our members. Please contact us via secretary@retina.org.nz or by phoning 0800 LOW VIZ (0800 569 849 Ext 2). Bulk orders are available to eye care professionals on request, however there may be a small charge to cover postage to non members and businesses. Mission Statement: To promote public awareness of retinal degenerative disorders; to provide information and support; and to foster research leading to treatment and an eventual cure. Retina New Zealand Inc is grateful to the Blind Foundation for funding the printing of this newsletter. Retina New Zealand would also like to thank the New Zealand Lottery Grants Board for helping to fund this newsletter. 18