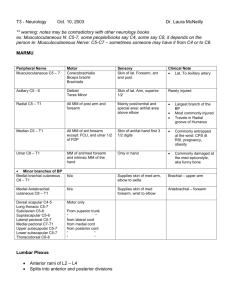
*Forgot to put in the graphic that musculocutaneous nerve innervates the anterior compartment of the arm + tends to pierce the coracobrachialis! Erb-Duchenne’s Palsy o Upper brachial plexus lesion (superior trunk) Damage to C5, C6 o Commonly affects suprascapular n., musculocutaneous n., axillary n. o Inability to abduct Abduction: supraspinatus (0-15°), deltoid (15-90°) o Inability to flex at elbow or supinate forearm "Waiter's tip" Klumpke's Palsy o Lower brachial plexus lesion (inferior trunk) Damage to C8, T1 o Commonly affects intrinsic muscles of the hand, wrist/finger flexors "Claw hand" Intrinsic Muscles of the Hand o "Bye-bye muscles" o Flex MCP + extend IP o Lumbricals 1 + 2: innervated by median n. 3 + 4: innervated by ulnar n. Closer to the pinky! o Interossei "PAD / DAB" Palmar "ADduct" Dorsal "ABduct" Blood Supply -Subclavian artery (before rib #1) -Becomes the Axillary artery (after 1st rib to the end of pectoralis minor) -Becomes the Brachial artery (after pectoralis minor) -Divides at distal end of cubital fossa to form Radial artery (lateral) + Ulnar artery (medial) Main Branches of Axillary Artery “Sally Thompson Loves Sex And Pot” Superior thoracic artery (I don’t think you’re responsible for this one, but it goes into the intercostals space) Thoracoacromial artery (has branches that go to the pecs + the acromion) Lateral thoracic artery (goes toward the serratus anterior muscle) Subscapular artery (has 2 branches!) o Circumflex scapular (goes around/under) o Thoracodorsal (goes to the latissimus dorsi) Anterior circumflex humeral artery (usually smaller + above the posterior circumflex humeral a.) Posterior circumflex humeral artery (usually fatter + goes posteriorly) -Median cubital vein: most commonly used for blood draws; it’s the connection between the cephalic + basilic veins -Cephalic vein: lateral; passes through the deltopectoral groove -Basilic vein: superficial + medial! The flexor retinaculum + extensor retinaculum mainly just function to hold the flexor/extensor tendons in place so they don’t pop out; that probably wouldn’t be really fun. :/ Elbow Ligaments Ulnar (medial) collateral ligament Radial (lateral) collateral ligament) Annular ligament (encircles the head of the radius) o If radial head slips out of annular ligament => nursemaid’s elbow (will present with guarding of elbow + inability to supinate) Carpal Bones (8) Proximal row (lat to med): Scaphoid, Lunate, Triquetrum, Pisiform Distal row (lat to med): Trapezium, Trapezoid, Capitate, Hamate) o “Trapezium” – “Thumb” (they kinda rhyme, so that might help you remember that that’s the “T” that’s closest to the thumb?) o “Some Lovers Try Positions That They Can’t Handle” Proximal to distal, lateral to medial for both rows o “So Long To Pinky, Here Comes The Thumb” Proximal to distal, lateral to medial => medial to lateral Carpal Tunnel! 9 tendons + 1 nerve o Flexor digitorum superficialis (4), Flexor digitorum profundus (4), Flexor pollicis longus (1) o Median nerve Phalen test: hold wrist in complete/forced flexion with dorsal surfaces of both hands pushed together Tinnel test: lightly tap over the median nerve o Pain/tingling sensation for either of these tests can mean that the pt is (+) for carpal tunnel syndrome “High-Yield” and/or Fun Facts o Axillary nerve usually runs with the posterior circumflex humeral artery in the quadrangular space o Can be damaged by shoulder dislocations + surgical neck fractures on the humerus o Radial nerve usually runs with profunda brachii (deep brachial) artery o Can be damaged by humeral shaft fractures / spiral fractures o Ulnar nerve = what causes the “funny” sensation you feel when you hit your funny bone (how humerus :O ) o Damage to the long thoracic nerve causes winged scapula b/c it innervates the serratus anterior o “C5 C6 C7, raise your arms to heaven” – to help remember the nerve roots + action o Radial artery runs through floor of anatomical snuffbox, so you can palpate your pulse there too! o => deep palmar arterial arch in the hand o But…speaking of the anatomical snuffbox, the borders are made up by the abductor pollicis longus, extensor pollicis longus + extensor pollicis brevis tendons If you palpate the snuffbox + feel a whole ton of pain, your scaphoid bone is probably fractured :/ This leads to all kinds of bad times and possibly avascular necrosis + poor healing due to lack of blood supply, so try not to fall on an outstretched hand :[ o Ulnar artery travels with the ulnar nerve + gives off common interosseous artery, which branches into the anterior + posterior interosseous arteries o Different from the nerves in that… Radial nerve => posterior interosseous nerve (after it passes through the supinator muscle) Median nerve => anterior interosseous nerve o => superficial palmar arterial arch in the hand o During pronation/supination, the radius is the bone that moves o Biceps = your strongest supinator o Brachioradialis, aka your “beer drinking muscle” the only flexor that’s innervated by the radial nerve! o Brachial artery = what you’re using to measure BP when you’re taking it in the arm! o Recurrent branch of the median nerve innervates the thenar eminence (abductor pollicis brevis, flexor pollicis brevis, opponens pollicis) o The adductor pollicis muscle isn’t cool enough to be part of the thenar eminence, so it is instead innervated by the deep branch of the ulnar nerve Sheaths o o Medial digit sheath communicates with common flexor sheath Common flexor sheath + sheath of pollex tendons communicates with carpal tunnel Joints (for the most part) o Acromioclavicular Joint Type I Tear in ACV ligament Type II Complete tearing of ACV ligament + partial tear to coracoclavicular ligament Type III ACV joint dislocated ("shoulder separation") o Glenohumeral Joint (Rotator Cuff) Stabilization Anterior Subscapularis Posterior Infraspinatus, teres minor Superior Supraspinatus Axillary nerve at risk for damage Travels through quadrangular space w/ posterior circumflex humeral artery Can use the “inverted soda can test” to test for impingement, esp. for the supraspinatus o Elbow "Nursemaid's elbow" Dislocation of elbow joint caused by sudden pull on extended + pronated arm Head of radius slips from annular ligament Guarding of elbow Inability to supinate o Wrist/Hand Fracture of distal radius in forearm Colles' fracture Posterior displacement of wrist + hand "Dinner fork" hand Tends to happen when falling with outstretched arms Scaphoid bone is the most commonly fractured! Can disrupt blood supply Radial artery runs through anatomical snuffbox (you can palpate your pulse there!) Blood perfuses distal to proximal (retrograde!) o Hip Extension tightens ligaments Femur head gets screwed into acetabular fossa Dislocation Femoral head dislodged from socket Weak Spot Posterior! (iliofemoral + ischiofemoral ligaments) Affected limb will shorten + internally rotate Fracture Fracture of femoral neck Much more common Angle of inclination decreases with age => greater stress on femoral neck External rotation: gluteus maximus, piriformis, quadratus femoris Medial circumflex femoral a. in danger! Supplies majority of blood to femoral head/neck Trendenlenburg Gait Contralateral pelvis drop/sag due to inability/difficulty abducting the lower limb Abduction: gluteus medius, gluteus minimus Lesion to superior gluteal n. Presentation: leaning to the side of the problem o Knees Terms used to describe distal aspect of limb distal to the joint Varus: "bowlegged" | Coxa valgus/Genu varum o Valgus: "knock-kneed" | Coxa varum/Genu valgum Ligaments Anterior cruciate ligament (ACL) Anterior drawer test Lachman test Posterior cruciate ligament (PCL) Cruciate ligaments are not inside synovial joint of knee Medial collateral ligament (MCL) Lateral collateral ligament (LCL) Swelling/effusion can be seen extending into suprapatellar bursa (superior extension of synovial joint--not a separate bursa) Popliteal (Baker's) Cyst Joint effusions can push synovial lining out of fibrous joint capsule + create synovial swelling in popliteal fossa "Unhappy Triad" From lateral trauma! Damage to medial meniscus, MCL, ACL McMurray's test used to check for tears in meniscus Patellar Dislocation Patella dislocates (usually laterally) Pain "inside knee cap" + tendency to flex leg even when relaxed Patellar Tendon Rupture Will be able to see patella moving further up quadriceps Difficulty/inability extending Complete Tear Tendon separates completely from top of tibia Inability to straighten leg Partial Tear Some fibers of patellar tendon torn Patellar Tendonitis Tendon torn in middle due to damage from overuse Feet :[ Foot Drop o Damage to common fibular n. or paralysis of muscles in anterior compartment of lower leg Weakness in dorsiflexion High-stepping gait Waddling gait Swinging out of leg gait Achilles Tendon Rupture Most commonly injured despite being the strongest/thickest tendon Often occurs by sudden plantarflexion or forced dorsiflexion outside ROM Lateral Ankle Ligaments During inversion, tendons on lateral side get stretched + will rupture if inversion is forceful enough. Ligaments will rupture in this order: Anterior talofibular Calcaneofibular Posterior talofibular Inversion injuries most common b/c deltoid ligament on medial side is one strong son-of-a-gun (medial malleolus typically tears away before it ruptures) Further eversion will fracture distal tibula Pott's fracture Proximal tibiofibular joint is a separate synovial joint at the knee OPP Correlate Check for fibular head dysfxn by gliding fibular head anterolaterally + posteromedially Fibular head anterior S/D: fibular head posteromedial glide restriction External rotation of tibia or Eversion of the foot carries distal fibula posteriorly + glides fibular head anteriorly They should be opposite of one another! Butt/Thigh Superior Gluteal Muscles Gluteus maximus o Extends + laterally rotates thigh o Inferior gluteal nerve (since it’s so big, it can actually reach the inferior portion – “big butts hang low,” if that helps?) o Superior + inferior gluteal arteries Gluteus medius/minimus o Abduction, medial rotation, prevent pelvic tilt w/ gait* o These are kinda like the “rotator cuff” muscles of the hip! o Superior gluteal nerve o Superior gluteal artery Tensor fascia lata o Stabilizes the knee in extension o Superior gluteal nerve *Trendelenburg gait: gluteus medius or minimus damaged or weak, so you end up with “hip drop,” where your hip drops on the side that you’re not standing on Deep Gluteal Muscles (short lateral rotators that stabilize the femoral head) – “PGOGOQ” from superior to inferior Piriformis o Sciatic nerve usually runs under it, so it hypertrophies or if sciatic n. runs through it instead of underneath it, it’ll get compressed + lead to sciatica (can eventually lead to weakness/loss of fxn of certain muscles) o Nerve to the piriformis Gemellus superior o Usually darker in color o The “GOG” makes up the “oreo” (dark-light-dark) Obturator internus o Dives around to attach to the femur; tends to be lighter in color since it’s mostly tendon here o Nerve to obturator internus innervates this + gemellus superior! Gemellus superior/inferior = hitchhiking gemelli brothers, so they don’t get their own innervations! Gemellus inferior o Sits on the outside of the obturator foramen; usually darker in color; super deep! Obturator externus o You can’t really see this one from a posterior view, but if you move the pectineus out of the way + look reallyyyy deep, it’ll be there Quadratus femoris o Square-shaped + underneath the “oreo”! o Nerve to quadratus femoris innervates this + gemellus inferior! Posterior Thigh (“butt kickers!” – extend thigh/flex leg) – tibial n. (except the short head!!!) / deep femoral a. Biceps Femoris o Long head o Short head This one’s the odd one out! It’s too short, so it can only flex the leg + is innervated by the common fibular/peroneal n. Fibular/peroneal = the same thing Semitendinosus o Has a really long tendon Semimembranosus o Looks really shiny o Most medial (membranosus/medial) Anterior Thigh – femoral n. / femoral a. Sartorius o “Hacky sack” muscle – flexes/laterally rotates thigh + flexes leg o Longest muscle in the body! Quadriceps femoris o Rectus femoris Rectus = “straight,” so…it’s the straight one in the middle of the anterior thigh The only one in this group that flexes the thigh as well as extends the leg!! o Vastus lateralis Most lateral o Vastus medialis Most medial o Vastus intermedius In the middle Iliopsoas o Not exactly a muscle of the anterior thigh, but it’s a major hip flexor Medial Thigh (adductors!) – obturator n. (except the hamstring part of adductor magnus!)/ obturator a. Pectineus Adductor brevis Adductor longus Adductor magnus o Hamstring part of adductor magnus Extends the thigh (it basically acts like a posterior thigh muscle) Tibial n.! because it’s so ginormus, it reaches the back + tibial generally gets all of the posterior thigh muscles Gracilis o Long + skinny! Leg *Other than fibularis brevis, there are no other “brevis” muscles in this section! :] Posterior Compartment (plantarflexion (mainly)!) – tibial n. / posterior tibial a. o Superficial Gastrocnemius Soleus Think of a slab of fish sitting underneath the gastrocnemius? Plantaris Tiny; practically looks like a nerve, but don’t be fooled! :O o Deep (“Tom, Dick And Nervous Harry”) Anterior to Posterior: tibialis posterior, flexor digitorum longus, posterior tibial artery, tibial nerve, flexor hallucis longus Flexor hallucis longus Flexor digitorum longus Tibialis posterior Anterior Compartment (dorsiflexion) – deep fibular n. / anterior tibial a. Medial to Lateral: “Tom’s Hairy Dog Fornicates” o Tibialis anterior Also helps with inversion of foot This tends to be what gets inflamed when you get shin splints! o Extensor hallucis longus Also extends great toe o Extensor digitorum longus Also extends digits 2-5 o Fibularis tertius Also helps with eversion of foot Lateral Compartment (eversion/plantarflexion) – superficial fibular n. / perforating branches of fibular a. o Fibularis longus o Fibularis brevis Greater saphenous vein: medial; travels anterior to medial malleolus + terminates in femoral vein in femoral triangle Lesser saphenous vein: lateral; runs between the 2 heads of the gastrocnemius m. + empties into popliteal v. Foot Tarsal Bones (“Tiger Cubs Need MILC”) (R foot, superior to inferior, medial to lateral) o Talus Articulates w/ tibia + fibula to form ankle joint o Calcaneus Heel bone (largest!) o Navicular o Cuneiform (Medial, Intermediate, Lateral) o Cuboid Plantar Compartment – medial + lateral plantar n. / medial + lateral plantar a. o 1st layer (Superficial) Abductor hallucis Flexor digitorum brevis Abductor digiti minimi nd o 2 layer Quadratus plantae Lumbricals rd o 3 layer Flexor hallucis brevis Adductor hallucis Flexor digiti minimi brevis Blood Supply Femoral artery o Popliteal artery Anterior tibial artery Dorsalis pedis artery (where you take the dorsalis pedis pulse) o Communicates w/ deep plantar arterial arch via deep plantar artery Posterior tibial artery Fibular artery Lateral plantar artery (forms deep plantar arterial arch on sole of foot) Medial plantar artery Innervation Sciatic nerve o Tibial nerve Medial plantar n. Lateral plantar n. o Common fibular nerve Superficial fibular n. Deep fibular n. Random Other Stuff (Possibly High-Yield) Femoral Triangle o Boundaries (“SAIL”) Lateral: Sartorius *Medial: Adductor longus Superior: Inguinal Ligament *I think your book might have something different for the medial border(?), so if that’s the case, please default to your lab sheet. :O o Contents Medial to lateral: VAN (femoral vein, femoral artery+deep femoral artery, femoral nerve) Or…lateral to medial: NAVEL (Nerve, Artery, Vein, Empty space, Lymph) Medial circumflex femoral artery = main blood supply to the femoral head, so if you knock that out (e.g. hip fracture) => necrosis :[ Common iliac artery o Splits into external + internal iliac arteries [Common] Femoral artery = continuation of external iliac a. at the inguinal ligament Called the superficial femoral artery after the deep femoral artery splits off o Becomes the popliteal artery after it goes through the adductor hiatus + comes out of the adductor canal Bifurcates into anterior + posterior tibial arteries
 0
0
advertisement
Related documents






Download
advertisement
Add this document to collection(s)
You can add this document to your study collection(s)
Sign in Available only to authorized usersAdd this document to saved
You can add this document to your saved list
Sign in Available only to authorized users