Instructor Guide - UNDP GEF Global Healthcare Waste Project
advertisement

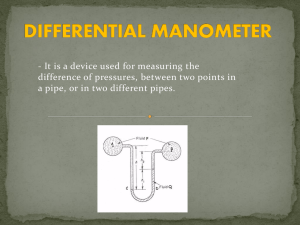
UNDP GEF Project on Global Healthcare Waste INSTRUCTOR GUIDE MODULE 19: RATIONALE FOR MERCURY-FREE HEALTHCARE 1 UNDP GEF Project on Global Healthcare Waste MODULE 19: RATIONALE FOR MERCURY-FREE HEALTHCARE Estimated Time Module Overview Learning Objectives Target Audience Lecture: 45 minutes Present the chemical and physical properties of mercury Describe the health effects of different forms of mercury from acute and chronic exposures Describe the health effects of mercury on children from pre-natal exposures Present the sources of mercury in the environment Introduce the WHO policy on mercury and the international campaign for mercuryfree health care Understand key properties of mercury including how mercury cycles in the environment Describe the health effects of mercury from acute and chronic exposures, as well as from pre-natal exposure Describe the contribution of the health sector to global mercury emissions Explain the WHO policy on mercury Understand the benefit of mercury-free health care Administrative Personnel HCWM Coordinators Facility Managers Healthcare professionals Other management staff Facility engineers and other staff involved in the repair, clean-up and storage of mercury devices 2 UNDP GEF Project on Global Healthcare Waste Instructor Preparation Materials Needed Student Preparation Review Questions Make notes pages of PowerPoint slides to hand out to class There are no directly associated Blue Book chapters for this module, but you may want to look through the other materials included in the References and notes. Make copies of any additional documents/readings that may be handed out to class, such as those included in the References If possible, download a copy of the Bowling Green State University: Mercury Vapor Experiment video at http://wbgustream.bgsu.edu/bgsu/epa/index-fl.html and prepare to show portions of the video in place of Slide 6 Prepare any additional notes to be discussed during the presentation Prepare any additional discussion points or review questions Projector Student handouts: slides, exercise, homework Flip chart and marker pens and/or board and chalk Read any articles provided by the instructor. How might a mercury spill affect patients, health providers and waste workers? What happens to mercury when it is released into the environment? How can mercury in the environment affect the community? Is your healthcare facility mercury-free? Does your healthcare facility have plans that follow the WHO policy on mercury? What are your country specific regulations for mercury? 3 UNDP GEF Project on Global Healthcare Waste PRESENTATION Slide Number/Title Teacher’s Notes Slide 1: Title Slide Note: there are some very detailed notes pertaining to many of the slides in this presentation. You may choose to summarize the information that has been included. There are advanced additional notes included for certain slides. Slide 2: Module Overview Introduce the outline and major points of the presentation Slide 3: Learning Objectives Describe what participants will learn at the end of this module. Slide 4: Properties of Mercury In the next slides, we will look at the properties of mercury, beginning with its chemical forms. We will also describe its volatility, its persistence in the environment, its bioaccumulative properties, and its toxicity. Slide 5: Chemical Forms of Mercury Mercury exists in different shapes and colors. Mercury has three basic chemical forms: elemental mercury as shown by the drop of liquid metal, inorganic mercury compounds (such as the white powder mercuric chloride and the red ore cinnabar), and organic mercury compounds (such as methyl mercury, Thimerosal – an organic mercury-based preservative whose chemical structure is shown on the bottom – and mercurochrome or merbromin, a red tincture once used as an antiseptic. Slide 6: Volatilization of Mercury Mercury has the highest volatility of all metals. Mercury droplets quickly vaporize at room temperature. The photo on the left shows a carpet with a few droplets of mercury from a broken thermometer. If you look closely, you can see some of the droplets on the carpet. Although mercury vapors cannot be seen by the naked eye, it is possible to see mercury vapors using a short-wave ultraviolet light source (black light) and a fluorescent background. The photo on the right shows the rising fumes of mercury vapor as seen under ultraviolet light. 4 UNDP GEF Project on Global Healthcare Waste Photos from a video experiment by Bowling Green State University, Ohio EPA, and Rader Environmental Services. Downloading and showing the video by Bowling Green State University is recommended. http://wbgustream.bgsu.edu/bgsu/epa/index-fl.html Slide 7: Persistence of Mercury in the Environment Mercury persists in the environment through the mercury cycle. The cycle begins when mercury vapor is emitted into the air from human activity (such as incineration or breaking a thermometer) and from natural sources such as degassing from rocks, soils, bodies of waters or volcanoes. Mercury then circulates in the atmosphere for between 3 months to 1-1/2 years. Eventually, mercury is deposited down into the ground or water by rain or snow or as mercury particles falling out of the atmosphere. In the water or in some soils, mercury is converted into insoluble forms which settle in the sediment. The mercury compounds are then converted by bacteria into an organic form which enters the food chain. Mercury is eliminated from organisms back into the environment or remains in the organism until it dies and decomposes. Eventually, mercury and its volatile forms in the soil and water are re-emitted back into the atmosphere to continue the mercury cycle. Slide 8: Bio-magnification of Mercury What is bio-magnification? When mercury falls in rain or snow, or when it falls out of the air as dry deposition, it may eventually be washed into waterbodies by rain. Bacteria in soils and sediments convert mercury to methylmercury. In this form, it is taken up by tiny aquatic plants and animals. Fish that eat these organisms build up methylmercury in their bodies. As ever-bigger fish eat smaller ones, the methylmercury is concentrated further up the food chain and bioaccmulates in the larger species. 5 UNDP GEF Project on Global Healthcare Waste Slide 9: Health Effects of Mercury (Hg) All forms of mercury are toxic at varying degrees, but the health effects depend on the form of mercury (whether it is elemental, inorganic, or organic), and the type of exposure (whether it is acute, meaning a short-duration exposure such as a few hours usually at high concentrations, or chronic, meaning long-duration such as exposures for months or years usually at very low concentrations). The health effects also depend on the route of exposure (whether the mercury is inhaled, ingested, or absorbed through the skin), and the dose or the amount of mercury. Acute exposure to high levels of elemental mercury in humans results in effects on the central nervous system such as tremors, slowed nerve functions or memory loss. Acute exposure of high concentrations of mercury through inhalation can result in kidney failure. Respiratory effects, such as chest pains, shortness of breath, and pulmonary function impairment have also been reported. Acute exposure to inorganic mercury by ingestion may result in nausea, vomiting, and severe abdominal pain. The major effect from chronic exposure to inorganic mercury is kidney damage. ADDITIONAL NOTES: Acute inhalation exposure of humans to high concentrations has resulted in kidney effects ranging from mild transient proteinuria to acute renal failure. Gastrointestinal effects and respiratory effects, such as chest pains, dyspnea, cough, pulmonary function impairment, and interstitial pneumonitis have also been noted from human inhalation exposure to elemental mercury. Slide 10: Chronic Exposure to Elemental Hg Chronic exposure to elemental mercury in humans affects the central nervous system in what has been called the Mad Hatter syndrome. In Lewis Carroll's famous book Alice's Adventures in Wonderland, the Mad Hatter is a fictional character who appeared to be crazy. Hatters, that is, people who made hats, used mercury to treat fabric before drying and stretching it to make felt hats. The mercury vapors poisoned the hatters, causing severe neurological damage. It was not unusual for hatters to appear mentally disturbed or confused. Other symptoms included erethism (abnormal irritability), tremors, and gingivitis (inflammation of the gums), as well as kidney disease. These are the chronic symptoms of exposure to elemental mercury. 6 UNDP GEF Project on Global Healthcare Waste Slide 11: Chronic Exposure to Elemental and Inorganic Mercury Another disease caused by chronic exposure to either elemental or inorganic mercury is a rare syndrome called acrodynia, or “Pink disease.” It’s an allergic reaction that occurs in some children exposed to mercury compounds. Its symptoms include severe leg cramps, rashes, fever, and a painful peeling of hands and feet which turn pink. Slide 12: Health Effects of Organic Forms of Hg The health effects of chronic exposure to organic mercury are different from effects related to elemental or inorganic mercury. Methylmercury is the form of mercury most easily absorbed through the gastrointestinal tract (about 95% is absorbed). Methylmercury is absorbed about six times more easily than inorganic mercury, and can migrate across the blood-brain and placental barriers, allowing it to affect brain and fetal cells. Slide 13: Health Effects of Organic Forms of Hg The most famous example of chronic exposure to methyl mercury happened in Minamata, Japan—a small town consisting mostly of farmers and fishermen and dominated by the chemical company Chisso. From 1932 to 1968, Chisso dumped an estimated 27 tons of mercury waste into Minamata Bay (as shown in the photo), with most of the mercury released after 1951. By the mid-50s, people started noticing a strange disease that affected cats, dogs, pigs, birds and people. That illness became known as the "Minamata Disease". It was caused by mercury in Chisso’s wastewater, which was transformed into methyl mercury, biomagnified in fish and shellfish, and then eaten by the local population. ADDITIONAL NOTES: The Chisso Corporation began as a fertilizer company, and gradually became a petrochemical and plastics company. Accused of polluting the bay, Chisso transferred their dumping in 1958 from the bay to the Minamata River which flows past the town of Hachimon and into the Shiranui Sea. Soon, people in this area also began developing the disease. According to the Japanese Ministry of the Environment (in Minamata Disease The History and Measures), 2,265 persons have been confirmed with Minamata disease in the Yatsushiro Sea coast around Minamata Bay as of the end of March 2001. 7 UNDP GEF Project on Global Healthcare Waste Slide 14: Chronic Exposure to High Levels of Methyl Mercury According to the Japanese Ministry of the Environment (in Minamata Disease The History and Measures), 2,265 persons have been confirmed with Minamata disease in the Yatsushiro Sea coast around Minamata Bay as of the end of March 2001. Chronic exposure to methyl mercury in humans affects the central nervous system with symptoms such as constriction of the visual field, irregular gait, and loss of coordination. The photo shows Yae Sato who is carrying fish home for her family. She is lame due to poisoning by methyl mercury in Minamata. Some victims suffered brain damage which made them resemble “living wooden dolls.” ADDITIONAL NOTES: Chronic exposure to methyl mercury in humans affects the central nervous system with symptoms such as loss of speech, paresthesia (a sensation of pricking on the skin), blindness, and malaise. Slide 15: Photo: 16-year old child with congenital Minamata disease Tomoko Uemura, shown here with her mother, is an example of a living wooden doll. After Tomoko’s mother ingested high levels of methyl mercury during pregnancy, she was born with severe cognitive impairment, ataxia (gross lack of coordination of muscle movement), blindness, and cerebral palsy. Tomoko, who is 16 years old in this photo, was poisoned in the womb and has been physically crippled since birth. Minamata disease is the result of chronic exposure to high concentrations of methyl mercury. Slide 16: Health Effects of Prenatal Exposure to Mercury: Faroe Islands Study 8 UNDP GEF Project on Global Healthcare Waste Slide 17: Results of Faroe Island Study This graph shows some of the results of the Faroe Islands research. The light blue-green columns on the left represent children in the lowest mercury exposure group. The red columns represent children in the highest mercury exposure group. The y-axis shows the percent of children in each exposure group that scored poorly in each category. Within each skill category, brain function impairment increases as mercury exposure increases. The adverse effects of mercury on attention, memory, and language are significant. ADDITIONAL NOTES: In this study, the mercury exposure of about 1000 children was evaluated prenatally and at the time of birth. Seven years later, impairments in attention, memory, and language were associated with increasing prenatal mercury exposure. The analysis controlled for potential social, economic, medical, and toxicologic confounders. The y-axis shows the percent of children in each exposure group that scored poorly (in the lowest quartile) in each cognitive category. The results are particularly striking for attention, where the percent of children scoring poorly more than doubles between the lowest and highest exposure quartiles. The effects of mercury on attention, memory, and language are all significant at the p<0.05 level. Slide 18: Seychelles Study Another famous study was conducted in the island nation of Seychelles in the Indian Ocean. The inhabitants have a diet high in fish. Although the study indicated a possible adverse association between mercury levels in the mothers’ hair during pregnancy and hand-eye coordination in the children, the Seychelles study showed no other developmental or IQ effects on children from the low levels of mercury their mothers were exposed to from eating fish. Slide 19: Follow-up to the Seychelles Study A few years later, the same researchers presented a follow-up study. They discovered that when beneficial effects of long-chain polyunsaturated fatty acids, such as omega-3 fatty acids, are taken into account, prenatal methyl mercury exposure shows an adverse effect on the Psychomotor Developmental Index of the children at 30 months of age. Therefore, if the beneficial effects of long-chain polyunsaturated fatty acids in fish are not considered, the adverse effects of prenatal methyl mercury exposure can be masked. MeHg = methyl mercury; PDI = Psychomotor Developmental Index 9 UNDP GEF Project on Global Healthcare Waste Slide 20: Prenatal Methyl Mercury Exposure and Cognitive Development One study quantified the impact of prenatal methyl mercury exposure on cognitive development. The researchers looked at three major epidemiological studies to quantify the association between prenatal methyl mercury exposure and cognitive development as measured by the intelligence quotient (IQ). They concluded that prenatal methyl mercury exposure that is sufficient to increase the mercury concentration in mother’s hair at child birth by 1 microgram per gram, decreases IQ by 0.7 points. ADDITIONAL NOTES: This analysis aggregates results from three major prospective epidemiology studies to quantify the association between prenatal MeHg exposure and cognitive development as measured by intelligence quotient (IQ). This paper identifies important sources of uncertainty influencing this estimate, concluding that the plausible range of values for this loss is 0 to 1.5 IQ points. Slide 21: Maternal Fish Consumption and Risk of Preterm Delivery Another fairly recent study indicated a higher risk of preterm delivery among women with low to moderate exposure to mercury. Preterm delivery is the most common cause of premature birth. In this large, community-based study, total fish consumption was associated with increasing mercury levels in hair. The study showed that compared with women who delivered at full term, the women with preterm deliveries, that is, women who delivered before 35 weeks' gestation, were more likely to have higher hair mercury levels. ADDITIONAL NOTES: This is the first large, community-based study to examine risk of every preterm birth in relation to mercury levels among women with low to moderate exposure. Total fish consumption and consumption of canned fish, bought fish, and sport-caught fish were positively associated with mercury levels in hair. The greatest fish source for mercury exposure appeared to be canned fish. Compared with women delivering at term, women who delivered before 35 weeks' gestation were more likely to have hair mercury levels at or above the 90th percentile (> 0.55 µg/g) , even after adjusting for maternal characteristics and fish consumption (adjusted odds ratio = 3.0 ; 95% confidence interval, 1.3–6.7) 10 UNDP GEF Project on Global Healthcare Waste Slide 22: Summary of Health Effects of Methyl Mercury on Humans This chart summarizes the health effects of methyl mercury according to the route of exposure (inhalation, ingestion or oral exposure, and dermal contact), based on studies reviewed by the U.S. Agency for Toxic Substances and Disease Registry in 1998. Methyl mercury has neurologic, developmental, and genotoxic impacts, as well as systemic effects depending on the route of exposure. Slide 23: Mercury: Declining Threshold of Harm This graph displays the general trend in the apparent toxic threshold for mercury as established at various points in time over the past three decades. Exposure to mercury is shown on the vertical axis, and year is on the horizontal axis. The blue squares represent prenatal mercury exposures associated with adverse neurodevelopmental outcomes. The Faroe Islands study, for example, is represented by the second blue square from the right edge of the graph. The red triangles represent recommended limits for human mercury exposure by regulatory agencies. The graph shows the tendency for apparent toxic thresholds to decline with advancing knowledge, as neurodevelopmental effects are seen at lower and lower thresholds for mercury by using increasingly sensitive exposure and outcome measures, and better statistical methods of analysis. ADDITIONAL NOTES AND ADVANCED DISCUSSION: The initial Iraqi toxic threshold is shown as the upper left-hand point on the graph. Within a few years of this observation, it became apparent that many children exposed prenatally to lower levels of mercury were delayed in learning to walk and talk, in spite of apparently “normal” development in infancy. (1) Subsequently, a variety of studies on diverse populations have established progressively lower thresholds for mercury effects by using increasingly sensitive exposure and outcome measures, and better statistical methods of analysis.(2-11) The Faroe islands study identified deficits in language, memory, and attention that occur at prenatal mercury exposures under 0.85 micrograms per kilogram per day. This exposure is less than 3% of the toxic threshold identified in the initial observations from the Iraqi epidemic. The presence of mercury effects below this level of 0.85 micrograms/kg/day implies that the actual threshold, if one exists, is lower. The blue squares on the graph represent prenatal mercury exposures associated with adverse neurodevelopmental outcomes. The red triangles represent World Health Organization (WHO), EPA, and Agency for Toxic Substances and Disease Registry (ATSDR) recommended limits for human mercury exposure. The standard issued by the FDA regulates the level of 11 UNDP GEF Project on Global Healthcare Waste mercury in fish, rather than in people. Thus, a wide variety of exposures may occur within the FDA regulatory limit, depending on how much and how often one eats fish, and the mercury level of the fish consumed. The indicated exposure is that of a 60 kg woman eating at the high end of fish consumption (100 grams/day, 95-97th percentile), eating fish contaminated at the FDA permitted limit. In this worst-case scenario, the woman is exposed to 1.65 mg/kilogram/day, about 16.5 times EPA’s recommended safe limit. Studies of the neurodevelopmental effects of mercury generally use hair or blood levels as markers of exposure, since these are more accurate indicators of exposure than dietary surveys. Healthbased guidelines, however, are expressed as recommended limits of dietary exposure. For the purpose of comparing data between studies, and for comparing effects levels with regulatory guidelines, exposures as indicated by hair and blood levels of mercury have been converted to approximate equivalent dietary exposures. The quantitative relationships are described in the ATSDR Toxicological Profile for Mercury. (12) Study results that identified a range of exposures within which an effect was observed have been shown at the mid-point of that range. Due to differences in study methods, results are not strictly comparable between studies, and are shown here mainly to indicate general trends over time. Sources: 1. Marsh D. Fetal methylmercury poisoning: new data on clinical and toxicologic aspects. Trans Am Neurol Assoc 102:69-71, 1977. 2. Marsh DO, Myers GJ, Clarkson TW et al. Fetal methylmercury poisoning: clinical and toxicological data on 29 cases. Ann Neurol 7:348-353, 1980. 3. Marsh DO, Myers GJ, Clarkson TW, et al. Dose-response relationship for human fetal exposure to methylmercury. Clinical Toxicology, 18(11): 1311-1318, 1981. 4. McKeown-Eyssen GE, Ruedy J Neims A. Methyl mercury exposure in Northern Quebec II. Neurologic findings in children. Am J Epidemiol, 118(4): 470-479, 1983. 5. WHO task group on environmental health criteria for methylmercury: Methylmercury, Environmental Health Criteria 101. Geneva, World Health Organization, 1990. 6. WHO Ibid. 7. Marsh DO, Clarkson TW, Cox C, et al. Fetal methylmercury poisoning. Arch Neurol 44:10171022, 1987. 8. Davidson PW, Myers GH, Cox C. Longitudinal neurodevelopmental study of Seychellois children following in utero exposure to methylmercury from maternal fish ingestion: 12 UNDP GEF Project on Global Healthcare Waste outcomes at 19 and 29 months. Neurotoxicology 16(4):677-688, 1995. 9. Grandjean P, Weihe P, White R. Cognitive Deficit in 7-year-old children with prenatal exposure to methylmercury. Neurotox Teratol 19(6):417-428, 1997. 10. Sorensen N, Murata K, Budtz-Jorgensen, et al. Prenatal methylmercury exposure as a cardiovascular risk factor at seven years of age. Epidemiology 10(4):370-5, 1999. 11. Environmental Protection Agency. Mercury Study Report to Congress: Executive Summary, vol. I, p 3-39, 1997, available at: http://www.epa.gov/ttnuatw1/112nmerc/volume1.pdf 12. Agency for Toxic Substances and Disease Registry: Toxicologic Profile for Mercury, draft. Atlanta, US Department of Health and Human Services, 1998. Slide 24: Growing number of fish consumption advisories due to high fish mercury levels With more data on mercury pollution and its health impacts at lower concentrations, many states have issued fish consumption advisories, warning that certain types of fish may have high levels of mercury that are of concern. These advisories recommend limiting the amount of fish consumed per week and avoiding certain kinds of fish. Greater than 95% of the mercury found in fish and shellfish is in the form of methyl mercury. Since methyl mercury concentrates in the muscle tissue of fish, it cannot be removed through cooking. Slide 25: Hg Exposure Potential from Seafood Nearly all fish and shellfish contain traces of methylmercury. In general, larger fish that have lived longer have the highest levels of methyl mercury since they generally prey on smaller fish and have had more time to accumulate mercury. Large fish such as swordfish, shark, king mackerel and tilefish pose the greatest risk. Typical concentrations are shown in parts per million. Canned light tuna generally has lower levels of mercury than tuna steak. RfD is the reference dose; it is an estimate of the highest daily exposure to a chemical over a lifetime without an appreciable risk of adverse effects. Eating more than one serving of swordfish or shark in one month may exceed the reference dose for methyl mercury. ADDITIONAL NOTES: Eating canned tuna more than two times a week (more than 12 ounces a week) may exceed the reference dose. RfD = reference dose, an estimate of daily exposure to the human population that is likely to be without appreciable risk of deleterious effects during a lifetime (IUPAC Compendium of Chemical Terminology, 2006) Graphic: swordfish (www.fun-with-pictures.com) 13 UNDP GEF Project on Global Healthcare Waste Slide 26: Mercury and Omega-3 Fatty Acids The beneficial impact of prenatal intake of omega-3 polyunsaturated fatty acids on cognitive function and the extent to which fish consumption protects against coronary heart disease and stroke in adults must be considered. Despite mercury contamination, fish are an important source of beneficial omega-3 fatty acids. The levels of mercury and omega-3 fatty acids vary according to fish and shellfish species. For example, fresh salmon and herring consumed in the U.S. are generally low in mercury and high in omega-3 fatty acids. In comparison, swordfish is generally high in both mercury and omega-3 fatty acids, while king mackerel is high in mercury and relatively low in omega-3 fatty acids. Consumers should check with their health authorities to find out the relative concentrations of mercury and omega-3s in locally available fish and shellfish species. Slide 27: Keep Mercury Out Of The Fish Not Fish Out Of The Mother! Fish Consumption Advisories should inform women who may become pregnant, women who are pregnant, nursing mothers, and the parents of young children about how to get the positive health benefits from eating fish and shellfish lower in mercury (for example, shrimp, canned light tuna, salmon, and catfish), while minimizing mercury exposure by avoiding types of fish that are higher in mercury (for example, shark, swordfish and king mackerel). Keep the mercury out of the fish, not the fish out of the mother. Slide 28: Mercury Emissions & Sources from Human Activity In tests of ice cores, peat cores, and lake sediment cores, an increase in mercury concentration is observed today compared with mercury concentrations during the pre-industrial period. Lake sediment cores, for example, indicate a three-fold increase in mercury levels compared to pre-industrial times. The pie-chart shows that about two-thirds of global atmospheric releases of mercury from human activity come from Asia, with China as the largest contributor worldwide. The United States and India are the second and third largest emitters. Slide 29: Global Mercury Trends 14 UNDP GEF Project on Global Healthcare Waste Slide 30: Range of Global Mercury Emissions in 2005 This chart shows the estimated range of global atmospheric mercury emissions to the atmosphere in one year. The bottom of the bar is the low end of the estimate, the top of the bar is the high estimate. Human activity accounts for about 1930 tonnes of mercury emitted to the air in 2005. The emissions from human activity alone are roughly equal to the combined estimates of natural emissions from oceans plus those from land. Re-emissions add a further contribution, with about half of re-emissions due to human activity. Thus, human activity accounts for a significant portion of mercury emissions. ADDITIONAL NOTES: Global atmospheric emissions of mercury from human activity in 2005 were estimated to be about 1930 (range 1230-2890) tonnes. This number is in the same range as the combined estimates of natural emissions from oceans (400-1300 tonnes per year) plus from land (5001000 tonnes per year). Re-emissions add a further contribution of around 1800-4800 tonnes per year. Slide 31: Sources of Mercury from Human Activities What are the sources of mercury pollution? Burning of fossil fuels, primarily coal, is the largest source of emissions from human activity, accounting for about 45%. Other sources include small-scale gold mining, industrial gold production, other mining and metal production, waste incineration, and releases from product use. Mercury is a pollutant also released by the healthcare sector. The largest sources as medical waste incinerators and the breaking and dumping of mercury-containing devices such as mercury thermometers and sphygmomanometers. Slide 32: Environmental Mercury and Medical Waste Incinerators Slide 33: WHO: Policy on Mercury in Health Care The growing concern over mercury led the World Health Organization to issue a policy on Mercury in Health Care in August 2005. In the short term, WHO called for plans to reduce mercury use, increase use of mercury-free alternatives, and to address the problem of mercury waste clean-up, handling, and storage. In the medium term, countries are asked to 15 UNDP GEF Project on Global Healthcare Waste further reduce unnecessary mercury equipment. In the long term, WHO supports a ban on mercury devices and promotion of alternatives. Slide 34: The Global Movement for Mercury-Free Health Care As a concrete step in achieving mercury-free healthcare, the international non-governmental organization Health Care Without Harm and the World Health Organization are co-leading a global initiative to achieve virtual elimination of mercury-based thermometers and sphygmomanometers over the next decade and their substitution with alternatives. The goal is to phase out demand for mercury thermometers and sphygmomanometers by 70% by the year 2017 and to shift production towards accurate, affordable, and safer mercury-free alternatives. The initiative is a component of the UN Environment Programme's Mercury Products Partnership. You may refer this website for more information on the current negotiations. http://www.unep.org/hazardoussubstances/mercury/tabid/434/default.aspx Slide 35: Picture of Poster in Different Languages By learning about the properties, sources and health effects of mercury, we can all do our part in protecting public health and the environment from mercury pollution. We hope this presentation generates discussion on the leading role that the health sector can play in reducing the harm from mercury. Slide 36: Minamata Convention on Mercury The convention took four years to negotiate and deals with a wide range of issues including mining of mercury, import and export of mercury, and safe storage. Governments agreed to ban the production, export and import of specific mercury-containing products by 2020, including non-electronic mercury devices such as clinical thermometers and blood pressure devices (sphygmomanometers). Discussion: Is you facility prepared to comply with the Minamata Convention on Mercury? For more information: http://unep.org/hazardoussubstances/Mercury/Negotiations/INC5/tabid/3471/Default.aspx Slide 37: Discussion Generate a discussion based off these questions 16 UNDP GEF Project on Global Healthcare Waste References (in order as they appear in slides) Bowling Green State University: Mercury Vapor Experiment. http://wbgustream.bgsu.edu/bgsu/epa/index-fl.html Minolta Photography - William Eugene Smith 1918-1978 with Aileen Mioko Sprauge Smith and Ishikawa Takeshi. Grandjean P, Weihe P, White R et al. Cognitive Deficit in 7-yr Old Children with Prenatal Exposure to Methylmercury. Neurotoxicology and Teratology 19(6):417-428, 1997 Myers GJ, Davidson PW, Cox C, Shamlaye CF, Palumbo D, Cernichiari E, Sloane-Reeves J, Wilding GE, Kost J, Huang LS, Clarkson TW: Prenatal methylmercury exposure from ocean fish consumption in the Seychelles child development study. Lancet 2003, 361:1686-1692 Landrigan PJ, Goldman L. Prenatal methylmercury exposure in the Seychelles. Lancet. 2003 Aug 23;362(9384):666. AH Stern, JL Jacobson, L Ryan and TA Burke: Do recent data from the Seychelles Islands alter the conclusions of the NRC Report on the toxicological effects of methylmercury? Environmental Health: A Global Access Science Source 2004, 3:2 PW Davidson, et al.: Neurodevelopmental effects of maternal nutritional status and exposure to methylmercury from eating fish during pregnancy, NeuroToxicology Volume 29, Issue 5, September 2008, Pages 767-775 “Long-chain polyunsaturated fatty acids and mercury,” JJ Strain, MP Bonham, (University of Ulster) PW Davidson, GJ Myers, SW Thurston, TW Clarkson, A Stokes-Riner, J Janciuras, J Sloane-Reeves, E Cernichiari, (University of Rochester School of Medicine and Dentistry), CF Shamlaye (Ministry of Health, Republic of Seychelles), EM Duffy, PJ Robson, JMW Wallace (University of Ulster), International Conference on Fetal Programming and Developmental Toxicity, Torshavn, Faroe Islands, 20-24 May 2007. Joshua T. Cohen PhD, David C. Bellinger PhD & Bennett A. Shaywitz MD (Harvard Center for Risk Analysis, Harvard School of Public Health, Boston, Department of Neurology, Children’s 17 UNDP GEF Project on Global Healthcare Waste Hospital, Boston, Massachusetts, Department of Pediatrics and Neurology, Yale University), Am J Prev Med. 2005 Nov;29(4):353-65. Fei Xue (Harvard School of Public Health, Harvard University, USA), Claudia Holzman (Department of Epidemiology), Mohammad Hossein Rahbar (Department of Epidemiology), Kay Trosko (Integrative Toxicology, Michigan State University, USA) and Lawrence Fischer (Integrative Toxicology, Michigan State University, USA)Environmental Health Perspectives Volume 115, Number 1, January 2007 Marsh D. Fetal methylmercury poisoning: new data on clinical and toxicologic aspects. Trans Am Neurol Assoc 102:69-71, 1977. Marsh DO, Myers GJ, Clarkson TW et al. Fetal methylmercury poisoning: clinical and toxicological data on 29 cases. Ann Neurol 7:348-353, 1980. Marsh DO, Myers GJ, Clarkson TW, et al. Dose-response relationship for human fetal exposure to methylmercury. Clinical Toxicology, 18(11): 1311-1318, 1981. McKeown-Eyssen GE, Ruedy J Neims A. Methyl mercury exposure in Northern Quebec II. Neurologic findings in children. Am J Epidemiol, 118(4): 470-479, 1983. WHO task group on environmental health criteria for methylmercury: Methylmercury, Environmental Health Criteria 101. Geneva, World Health Organization, 1990. Marsh DO, Clarkson TW, Cox C, et al. Fetal methylmercury poisoning. Arch Neurol 44:10171022, 1987. Davidson PW, Myers GH, Cox C. Longitudinal neurodevelopmental study of Seychellois children following in utero exposure to methylmercury from maternal fish ingestion: outcomes at 19 and 29 months. Neurotoxicology 16(4):677-688, 1995. Sorensen N, Murata K, Budtz-Jorgensen, et al. Prenatal methylmercury exposure as a cardiovascular risk factor at seven years of age. Epidemiology 10(4):370-5, 1999. 18 UNDP GEF Project on Global Healthcare Waste Environmental Protection Agency. Mercury Study Report to Congress: Executive Summary, vol. I, p 3-39, 1997, available at: http://www.epa.gov/ttnuatw1/112nmerc/volume1.pdf Agency for Toxic Substances and Disease Registry: Toxicologic Profile for Mercury, draft. Atlanta, US Department of Health and Human Services, 1998. American Heart Association & Food and Drug Administration “The Global Atmospheric Mercury Assessment: Sources, Emissions and Transport,” UNEPChemicals Branch, United Nations Environment Programme, Geneva, Switzerland, 2008. US Geological Survey, 2002 WHO: Mercury in Healthcare. http://www.who.int/water_sanitation_health/medicalwaste/mercury/en/ WHO: Mercury in Health Care Policy Paper. http://www.who.int/ifcs/documents/forums/forum5/mercurypolpaper.pdf WHO, Health Care Without Harm: Mercury-Free Health Care. www.mercuryfreehealthcare.org Health Care Without Harm. www.noharm.org UNEP, You may refer this website for more information on the current negotiations. http://www.unep.org/hazardoussubstances/mercury/tabid/434/default.aspx 19