Population Policies in the Pacific Island Countries: WHAT Future?
advertisement

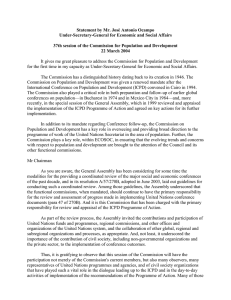
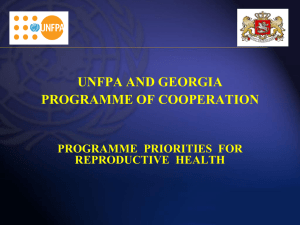
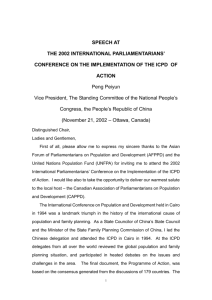
Reflections Number 3 Perspectives December 1999 POPULATION POLICIES IN THE PACIFIC ISLAND COUNTRIES: WHAT FUTURE? by William J. House Adviser on Population Policies and Development Strategies The Situation Pre-ICPD Many of the Pacific island countries formulated population policies in the period before the International Conference on Population and Development (ICPD) which was held in Cairo in 1994. They expressed a principal concern for reducing high fertility and rapid population growth. While the policy statements often demonstrated the need for population-responsive policies in the various social and economic sectors, their targets and objectives were already enclosed in various other documents. For example, environment policy was sometimes incorporated in a National Environmental Management Strategy (NEMS), family planning programmes were being actively implemented by Ministries of Health and there were often formal policies both for women and for youth. Yet, attempts at coordination of the various policy interventions through a high-level National Population Council and a multisectoral coordinating committee were not very effective. Since they pre-dated the ICPD, the policies were very much driven by anti-natalist demographic concerns and failed to introduce the ICPD concepts of reproductive rights and reproductive health. And the demographic targets of the policies were often totally unrealistic. As a result they seem to have had little lasting influence, such that many are currently under revision. Despite this, family planning programmes have made progress recently in many countries by overcoming to some extent “All States now understand that, if they are to provide adequately for the future health and education of their citizens, they need to incorporate population policies into their development strategy.” Secretary-General Kofi Annan, speaking at the Opening Ceremony of the UN Special Session of the General Assembly on 30 June 1999. 1 various constraints, such as shortages of finance, skilled service providers and counsellors, contraceptives, infrastructure and management skills. But the family planning programmes generally did not rely on the national population policy for their rationale and justification and tended to be vested in the Ministry of Health. The multisectoral approach to population policy, which was meant to be reflected in the operations of the Population Policy Coordinating Committees, was never very effective and proved incapable of taking a leading policy-making role in the implementation of the policy. Family planning units in Ministries of Health persevered without any major moral or vocal support for population policy from Heads of State and Government, Cabinets or Ministries of Finance. No doubt, this failure to galvanise the support of the national political leadership, particularly the civil and religious leaders, as well as officials in the National Treasury, impeded the implementation of the MCHoriented family planning programme as well as the multi-sectoral population policy. Nor has population and population-related issues been adequately integrated into the national development planning process, partly because of the failure to raise population concerns high enough on the policy-agenda. The result is that population policy has continued to be largely identified with Ministries of Health and their family planning programmes. Post-ICPD In the period since ICPD, advocacy has been undertaken to reorient policy makers, programme managers and project personnel towards a better understanding of the concept and scope of reproductive health and to assist countries to move towards comprehensive reproductive health, including family planning and sexual health services (RH/FP-SH). Reorientation has sought to generate an appreciation of the linkages between population dynamics and development and the implications of the paradigm shift from MCH/FP to RH/FP-SH. Emphasis has shifted to promoting individual choice and well-being rather than demographic targets, and a stress on integrated quality of care and services. After five years of advocacy efforts, the concept has been widely accepted and the operational implications are well understood by national programme managers and service providers. The integration of reproductive health is already occurring in the practical stages in varying degrees at the primary care level, but more needs to be done at the secondary and tertiary or Indicators and threshold levels of achieving goals of the ICPD Programme of Action by the 2005. Goal and Indicators Threshold Levels Goal: Access to reproductive health Proportion of deliveries attended by trained health personnel Contraceptive prevalence rate Proportion of population having access to basic health services 60 per cent 55 per cent 60 per cent Goal: Mortality reduction Infant mortality rate Maternal mortality ratio Goal: Universal primary education Gross female enrolment rate at primary level Adult female literacy rate 50 infant deaths per 1,000 per live births 100 maternal deaths per 100,000 live births 65 per 100 eligible population 50 per cent Source: United Nations Population Fund (1996) 2 national levels. To this end, increasing elements of the reproductive health concept are being incorporated into the new cycle of various donor projects. However, most countries need financial and technical assistance from their development partners in the interpretation and implementation of the ICPD POA to meet local conditions. Of the population policies that have been designed in the post-ICPD era, perhaps the draft policy for Vanuatu comes closest to reflecting the philosophy of the ICPD’s POA1. For example, the draft document is explicit in upholding the principles of the ICPD POA and confirms the inalienable rights of women to equality and equity, their right to determine their own fertility, as well themselves, as well as the means to reduce fertility and the rate of population growth. However, the policy has yet to be endorsed by Government. With the new emphasis on reproductive health, where does that leave the demographic concerns of the earlier versions of population policy? Will the purveyors of the new reproductive health approach be able to galvanise the support of national political and religious leaders and policy makers in order to attract their blessing and financial and moral commitment, when the earlier family planning programmes often failed to do so? If their principal concern is with too rapid population growth in relation to natural and Goal Indicators of the PICs % of Deliveries Attended by Trained Personnel (1) 60 Contraceptiv e Prevalence Rate (%) (2) 55 60 50 100 65 50 Melanesia Fiji Solomon Islands Vanuatu 100 87 79 *31 *8 *15 100 80 80 16 38 45 31 *550 68 90 *36 70 91 *20 *30 Micronesia FSM Kiribati Marshall Islands Nauru Palau 82 72 na 100 100 *25 *28 *26 na *46 75 100 95 100 80 46 *67 *63 11 20 *561 *225 0 0 0 83 78 79 95 90 66 91 69 95 88 Threshold Level by 2005 % Pop. With Access to Basic Health Services (3) Infant Mortality Rate Maternal Mortality Rate (4) (5) Female Primary School Enrolment (%) 5-14 years (6) Polynesia 100 *53 100 11 20 100 Cook Islands 100 *39 100 18 0 96 Niue 100 na 100 38 *170 98 Tokelau 94 *32 100 19 *160 91 Tonga 100 *40 100 *51 0 88 Tuvalu 95 *31 100 22 70 94 Samoa * Failure to meet the relevant threshold Source: UNDP (1999). Columns (1) – (3) and (5) are taken from WHO (1997 and 1998). Column (4) is from SPC (1998). Adult Female Literacy Rate (7) 94 97 90 99 95 96 as the elimination of violence against women. However, the draft policy is still anti-natalist in tone and wishes to lower the national rate of population growth as well as fertility and mortality. The extended provision of quality reproductive health and family planning services, including IEC, are identified to be a worthy end, in and of other resources, then the reproductive health agenda emanating from the Cairo POA must be shown to have a significant demographic effect. But can this linkage be adequately demonstrated to the political leadership which may treat the too rapid growth in numbers as the priority concern for development expenditure and planning? 1 This writer would propose that high and middle level political and bureaucratic The UNFPA Country Support Team based in Fiji has provided significant technical guidance in the preparatory activities and the drafting of the policy. 3 commitment to address national populationrelated problems, including extensive reproductive health concerns, are more likely to be attained if broad-based national population problems and multi-sectoral strategies to deal with them are expressed in a national population policy. To the political elite, seemingly esoteric reproductive health and gender concerns will not be adequately appreciated if they are treated as independent health issues. They are much more likely to receive the support and expanded budgetary allocations of national exchequers and international donors if they are conceived to be integral parts of broadbased national efforts to deal with population and development problems in a holistic manner. Already the enthusiasm surrounding the new concepts arising from the ICPD has been dampened by the hard reality of having to compete with other interested parties for the national purse strings. The international donor community has fallen way behind in meeting the projected financial needs for implementing the reproductive health programmes identified in the International Conference on Population and Development. One way to arouse renewed interest would be to incorporate the linkages between interventions to promote improved reproductive health status, fertility decline and reduced population growth in the form of national population policies, conceived as integral parts of national development programmes. Meanwhile, if this approach is accepted, the Pacific island countries will require much technical support to undertake this task. Status of Population Policy in the Countries of the South Pacific Country Cook Islands Fiji Kiribati Marshall Islands FSM Nauru Niue Palau PNG Samoa Solomon Islands Tonga Tuvalu Vanuatu Status of Population Policy None Implicit Policy in Development Plan In preparation Revised and Endorsed Draft to be revised None In preparation Completed Policy revised Draft completed Revision completed In preparation In preparation In preparation Principal Demographic Concerns Limit population growth Lower fertility Reduce fertility: health oriented improvements To promote return migration and repopulate Reduce out-migration, retard alien inflows Lower fertility, reduce urbanization Lower fertility, promote development Lower fertility, reduce ubarnization Lower fertility; reduce urbanization Lower fertility/RH/FP/ICPD goals Source: Authors' estimates and interpretation References: SPC (1998), Pacific Island Populations, Noumea UNDP, (1999), Pacific Human Development Report 1999: Creating Opportunities, UNDP, Suva UNFPA, (1996), A Revised Approach for the Allocation of UNFPA Resources to Country Programmes, New York WHO (1997), Country Health Information Profiles, WHO Regional Office for the Western Pacific, Manila. WHO (1998), Western Pacific Regional Health Databank, WHO, Manila. Reflections will be published periodically by the UNFPA Country Support Team for the South Pacific. Views expressed do not necessarily reflect the opinions or policy of the United Nations Population Fund. Correspondence should be addressed to: The Director, UNFPA Country Support Team, GPO Box 441, Suva, Fiji. Phone: (679) 312-865 Fax: (679) 304-877 Internet email: Registry@unfpacst.org.fj Homepage: http://www.undp.org./popin/regional/asiapac/fiji/fijihome.htm 4