FLOODS IN MOZAMBIQUE
advertisement

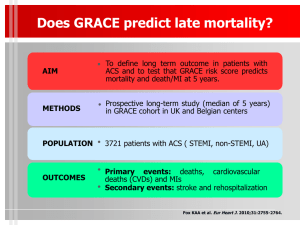
FLOODS IN MOZAMBIQUE EMERGENCY HEALTH REPORT 1- Introduction The floods have been caused mainly as a result of heavy rains (from December 2000 to April 2001), flooding in from central Mozambique and neighbouring countries, producing twice as much rain as compared to previous years. The areas most affected are the Sofala, Zambezia, Tete and Manica provinces. The affected population is estimated to exceed 500,000 (including 50 deaths), out of which 220,000 inhabitants live in Accommodation Centres (ACs). Several homes, bridges and farms were destroyed. Access roads have been rendered impassable by the floods resulting in isolated populations in many areas. 2- Terms of reference Co-ordinating WHO’s response with MOHs, NGOs, UN agencies and donors. Preparing and completing a WHO format for consolidated appeals. Mobilising funds. Developing a tool for measuring quality and effectiveness of humanitarian aid during this emergency. The tool will assess whether; the guidelines of Mozambique are being followed, assessed needs are being met by assistance provided, the health system of Mozambique is being strengthened. e) Establishing in collaboration with the MoH an evaluation team and organising a survey of health related humanitarian assistance to measure the quality of interventions and their impact on the environment and the country's health system. f) Developing recommendations for improving the health related humanitarian interventions. g) Formulating action plans based on evaluation results. a) b) c) d) 3- Activities a) Meetings with WCO Mozambique at the WHO office in Maputo, to discuss and analyse the emergency situation. b) Visit to the centre of operations for emergencies in the Beira and Sofala provinces where the following activities were carried out: » Participating in the daily meetings of the "Gabinete de Operaciones de Emergencia" chaired by INGC. Participants included OCHA, UN agencies, National health authorities (DPS of the 4 affected provinces) and NGOs at Beira airport. » Daily meetings with the authorities of the DPS of Sofala province to analyse the present health situation and give technical advice. » Visiting ACs in the Marromeo district (Sofala province) namely Nensa and Chupanga, with local health authorities, members of UN agencies and NGOs. » Daily meetings with UN agencies and OCHA. Staff working in the affected areas will give technical health advice and support and plan health activities for the affected populations. c) Meetings in Maputo with different health authorities (Departments of Epidemiology, Nutrition, EPI-Prevention, Drugs and INGC) in the MoH to co-ordinate many activities in relation to the emergency situation. d) Activities in Beira: 1- A joint technical mission "Mission of rapid evaluation of the alimentary situation and survival mechanisms in the districts affected by floods". formed by representatives of the Government (MoH-INGC), UN agencies (WFP, UNICEF and WHO) and the main NGOs was organised. The team evaluated: the health and sanitary conditions of the ACs, access to health services, epidemiological situation with regard to diseases like Malaria, Diarrhoea, Dysentery, ARI, Skin diseases, Cholera, Meningitis, Measles, TBC, Anaemia, Malnutrition, Bilharziosis and HIV-AIDS. The team visited ACs and isolated populations in affected districts eg. Marromeo and Chemba in the Sofala province, Chinde and Mopeia in the Zambezia province and Inhangoma in the Mutara District. Finally the team visited an area with a mixed population of IDPs and local inhanitants in Sabeta-Tambara District in the Manica province. 2- A General Information Meeting was convened at the Beira airport to present a draft of results gathered by the mission and to point out the main health needs of the affected population. 3- An official report (both in English and Portuguese) on the health conditions was presented to the head of the mission from INGC. 4- Meeting with different authorities from the DPS in the Sofala province responsible for health in the affected areas to analyse the situation and provide technical support. 5- Participating in a 4-day workshop on the Emergency Health Situation, which was held in the Mozambique Hotel, Beira city. This workshop was organised by the Ministry of Health (DNS - DHA / DEE and DPS-Sofala) and supported by WHO, Central Health Authorities, and chief medical officers of all the provinces. 6- Visiting the Cholera affected areas in the Mutarara district (Tete province), Sena, Traquino, Caia and the bigger ACs like Chupanga and Nensa, after which a report with recommendations was presented to the MOH. 7- Visiting MEDIMOC, Beira and Central stock to analyse the situation regarding provision of Cholera treatment. 8- Meeting with the responsible officer for the laboratory in the Central Hospital, Beira to analyse the situation regarding diagnosis of Cholera Vibrion. e) Meeting and planning with; Dr. Solange Kouo Epa (WR Mozambique) and Dr.Pierre Kahozi on the future actions for WHO’s emergency operations. f) Exhibiting photographs of the assessment taken over the period to expose the health situation and mobilise funds. 4-Findings a) Absence of proper co-ordination: 1- Many agencies and NGOs are working in the affected areas in an uncoordinated manner. 2- The organisations are unevenly distributed in the affected areas, with some areas receiving no attention. 3- The NGOs (instead of the MOH) usually choose the working place. 4- Some of the NGOs lack well-trained professional staff. 5- There is lack of communication between the NGO and government staff working in the ACs and with the IDPs. 6- The NGO staff is not enough in numbers to cope with the large populations of the ACs. 7- The roles of the community leaders are not well defined. 8- The DPS does not receive enough information from the various health posts in the ACs. 9- There is lack of management and co-ordination in the ACs. 10- There is lack of management and co-ordination (emergency technical co-ordinator adviser) in the Emergency Co-ordination Unit in Beira airport. 11- There is lack of health co-ordination in the affected areas. 12- The health authorities of the DPS in Sofala province are responsible for the four affected provinces. 13- The accreditation of NGOs working in emergencies is based on a general scheme, which is not appropriate in an emergency situation. 14- There is no proper co-ordination team in the MoH b) No advance plans were made to deal with the increased numbers in the ACs. The large populations present in these ACs overburdens the community health workers. In addition, since these centres are overcrowded, there is an increased risk of disease transmission. The populations in the surrounding areas are attracted to the ACs especially during food distribution. This has led to an increase in size in populations living in the ACs. c) Health problems facing populations in the ACs: 1- High population density presents an ideal environment for the development of infectious diseases transmitted direct or indirectly through the different vectors. 2- There is not enough well-trained staff in the health posts to cope with the large numbers. The provision of drugs and medical equipment and the physical conditions of work (space, hygienic conditions, etc.) are very poor. 3- The data collected is not communicated to the appropriate authorities. 4- The health posts have no referral systems in cases of emergency. 5- Malaria, Acute gastro-enteritis (bloody and non-bloody) and ARI are the most common diseases found. Other diseases found are skin diseases, conjunctivitis, intestinal worms, Bilharziosis, STD, Malnutrition and Anaemia. The prevention measures against these diseases are very poor. 6- The epidemiological data collected from the ACs is not included in the "Boletin Epidemiologico Semanal" 7- The IEC is poorly developed, with shortage of well-trained personnel and material for health education. 8- Most of the ACs have no programs on HIV/AIDS/STD prevention. 9- The Vaccination Campaigns in the ACs was started at a very late stage. Vaccination against Meningitis has not been implemented in many centres. 10- Nutritional surveys and supplementary feeding are non-existent in these centres, even though there are several cases of moderate to severe malnutrition among children under 5. 11- Efforts have been made in these ACs to provide safe drinking water, however the majority of them are still drinking water from the rivers and wells. There is very little education on safe water consumption. 12- There are very few latrines which are in poor sanitary state, resulting in cases of Acute gastro-enteritis. d) Many villages surrounding the Zambezi river have large numbers of IDPs. These IDPs have no tents and have therefore had to build huts for themselves. They have received no health assistance. e) Large numbers of isolated populations contribute to unofficial ACs. This population runs a high risk of contracting infectious diseases since they do not receive assistance in any form. There is no access to safe water, health facilities, good sanitation, waste disposal and food. f) Many ACs and health posts in the affected areas are short of drugs due to the following reasons; -lack of transportation -inaccessible roads -lack of communication between the district, ACs and central stock -very poor co-ordination among MEDIMOC Maputo, Beira and the Sofala and Central warehouses -the four affected provinces have no personnel in charge of monitoring/managing the drugs. The Sofala district however has the personnel, though their roles are not very welldefined g) Cholera. CHOLERA CASES PER PROVINCES - 2001 * Provinces Maputo City Maputo Prov. Gaza Manica Sofala Tete Total Cases 2.207 132 37 147 22 110 2.665 Deaths 20 2 0 2 0 0 24 T.L. 0.9 % 1.5 % 0 % 1.4 % 0 % 0 % 0,9 % *UCITE/MISAU-Gabinete de Epidemiologia - DNS 2001 By 25th April 2001, (16th epidemiological week), 2665 cases of cholera were officially reported. The present epidemic was detected first in Mutana (Tete province) on 5th April. The main cause of the epidemic was found to be consumption of contaminated river water. There is no laboratory in these areas. h) There were 2 confirmed cases of the Plague (Mozambicans formerly living in Zambia) 5- Recommendations 1- To create in the MoH a unit for Emergency Preparedness and Responses in Health at the same level of the Gabinete of Epidemiologia with the presence of a specialised emergency trainer/co-ordinator for at least two years. This unit would manage and coordinate health issues in emergency situations such as natural disasters and outbreak of epidemics. The co-ordinator would train the local staff in order to prepare a professional team for the unit. WHO could provide the emergency health co-ordinator to support the new co-ordinator during the training. 2- To create in the WHO office Mozambique a unit for Emergency Preparedness and Responses to co-ordinate, support and give technical advice in health in any event considered as an emergency situation to the MoH, INGC, UN Agencies and NGOs. 3- To review the accreditation of NGOs working in Emergencies and the qualifications of their health personnel. 4- In the AC: a) To plan in advance capacity building to cope with large populations. b) Avoid overcrowding. c) Ensure strict measures to limit the number of displaced entering d) Nominate a team leader e) Following the official advice in health for the population living in the AC. (Number of latrines, waste disposal, water sources, access to health, etc.) f) Improve the quality and quantity of health posts g) Provide drugs and medical equipment for the health posts h) Improve the IEC. i) Improve the implementation of massive vaccination campaigns against BCG, DPT, DT, Measles, Polio, Meningitis, and vitamin A deficiency mainly for the more vulnerable groups eg. children under 5, pregnant and lactating women. j) Implement a referral system for emergency patients to be transferred. k) Implement health education and prevention against Malaria, Acute gastroenteritis, ARI and HIV-AIDS and STD. l) Implement epidemiological surveillance. m) Identify and meet the urgent and basic needs of the unofficial ACs. n) Improve means of diagnosis and preventive measures against cholera. o) Provide safe water and good sanitary conditions. p) Implement a rapid nutrition assessment in children under 5. q) Improve communication between the ACs, the districts and the DPS. 5-To improve capacity building of the health posts in the villages with IDPs. 6-To improve vaccination coverage in the affected areas. 7-To improve national surveillance in the affected areas. 8-To nominate specific staff health personnel for emergency situations. Maputo, MOZAMBIQUE, April 30th, 2001 Dr.ARTURO SILVA MD.MPH. WHO-EHA