PUMA Step-downs and Discharges QRG
advertisement

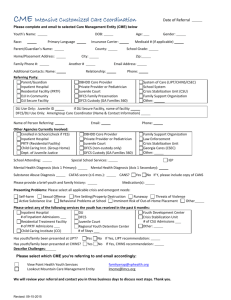
PRTF Admission template/requirements: Up/Down at Different Facility (not a discharge to OP) Scenario: Completing a pre-authorization review for the PRTF LOC. Effective Date: 12/01/2015 *Please type A valid CON must be attached Name/phone number of the requestor Name/phone number of the legal guardian Anticipated d/c plan (from PRTF) to include anticipated residential placement Anticipated family involvement (willingness to participate) History of PRTF treatment with dates (or other out of home placement i.e. TGH, NMGH, TFC, detention, etc.) History of inpatient stays/days/dates History of outpatient providers with detailed explanation of why outpt has failed (why is less restrictive LOC not indicated) Diagnosis (to include psych, SA, DD, personality, medical) Current medications Medical Hx/special needs (who is the PCP) CSOC involvement (do they support this level of care) with clear documentation from the WAA that they support PRTF Full scale IQ History of OCDD involvement/status of referral (if applicable) Risk factors (family History of MI,SA, abuse (victimization vs. perpetration), trauma, SI/HI, psychosis) Legal Hx and current legal issues Compliance related issues 1 Current mental status with most recent psych eval (within the last 30 days) Behaviorally measurable goals/expected outcomes from the PRTF stay 2 For additional days requested: Identify specific POC (what goals have been met, what goals are left, why continue at this LOC) Family involvement (family sessions held/pending/progress made) MSE/behavior/participation Med changes/compliance Change in Diagnosis School participation/attendance Specific d/c plan Anticipated LOS Coordination of care activity