Efficacy of Intralesional 5-fluorouracil and Triamcinolone
advertisement

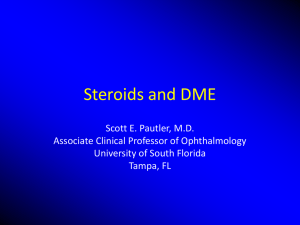
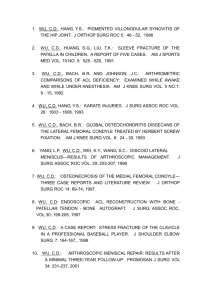
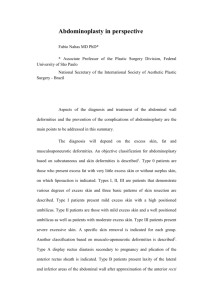
Efficacy of Intralesional 5-fluorouracil and Triamcinolone in the Treatment of Keloids Joseph H. Dayan, MD, Steven P. Davison, DDS, MD, Smitha Sonni, MD, Amy Crane, MD BACKGROUND: Keloids are a common problem with a reported incidence of 4.5 to 16 percent in darker-skinned individuals.1, 2 Intralesional triamcinolone has traditionally been the mainstay of treatment and in conjunction with excision has yielded efficacy rates between 58% and 93%.3-7 However there are a significant number of treatment failures and substantial inconsistencies with regard to the reproducibility of results. Additionally, adverse effects including hypopigmentation, atrophy, and telangiectasias have been reported to be as high as 37% in the literature.8 The purpose of this study is to evaluate the efficacy and adverse effects of a 5-fluorouracil/steroid mixture over the past seven years and compare the results with steroid alone. METHODS: All charts from 1999 to 2006 were reviewed. Patients were stratified into three groups: 5-FU/steroid without surgical excision, 5-FU/steroid with excision, and steroid with excision. The follow-up period ranged from 6 months to 6 years. Percentage size reduction and adverse effects including telangiectasia, atrophy, hypopigmentation, and dehiscence were recorded. A mixture of 75% 5-FU and 25% Kenolog 40 was most commonly used. 0.1 ml of solution per centimeter of lesion was injected. Patients undergoing concurrent excision received injections intraoperatively and again at 2, 4, and 6 weeks post-op. Non-surgical patients received injections an average of four weeks apart. RESULTS: A total of 94 patients with 102 keloids were identified. Patients who underwent excision with the 5-FU/steroid combination had a 92% average reduction in lesion size compared to 73% in the group of patients who did not receive 5-FU. Patients who received 5-FU/steroid without excision had an average size reduction of 81%. These differences were statistically significant (p = 0.05). Adverse effects were higher in the 5-FU groups compared with the steroid only group (23% and 15%, respectively), although these results were not statistically significant (p = 0.62). The most common side effect was telangiectasia. CONCLUSIONS: Although this study is limited by its retrospective nature, the results in this study, the supporting basic science data, and anecdotal reports suggest combination 5-FU/triamcinolone may be superior in efficacy compared to intralesional steroid therapy.9-16 The successes of 5-FU in those particularly intractable keloid cases where steroids have failed is significant. Interestingly, the side effect profile was not lower in the 5-FU group. However, we speculate the telangiectasias and atrophy were likely caused by the steroid component. Thus, we are prospectively studying the effects of 5-FU with a lower triamcinolone dose. Long-term prospective trials using antineoplastic agents are needed to properly establish an ideal treatment regimen for this challenging problem. Figure 1. A 43 year-old gentleman presenting with recurrent keloids after failed multimodal triamcinolone treatment. Results shown after intralesional 5-FU, excision and single-dose radiation at 20 months post-op. REFERENCES 1. Ketchum, L. D. Hypertrophic scars and keloids. Clin. Plast. Surg. 4: 301-310, 1977. 2. Oluwasanmi, J. O. Keloids in the African. Clin. Plast. Surg. 1: 179-195, 1974. 3. Al-Attar, A., Mess, S., Thomassen, J. M., et al. Keloid pathogenesis and treatment. Plast Reconstr Surg 117: 286-300, 2006. 4. Berman, B., Flores, F. Recurrence rates of excised keloids treated with postoperative triamcinolone acetonide injections or interferon alfa-2b injections. J Am Acad Dermatol 37: 755-757, 1997. 5. Griffith, B. H. The treatment of keloids with triamcinolone acetonide. Plast Reconstr Surg 38: 202-208, 1966. 6. Griffith, B. H., Monroe, C. W., McKinney, P. A follow-up study on the treatment of keloids with triamicinolone acetonide. Plast Reconstr Surg 46: 145-150, 1970. 7. Tang, Y. W. Intra- and postoperative steroid injections for keloids and hypertrophic scars. Br J Plast Surg 45: 371-373, 1992. 8. Asilian, A., Darougheh, A., Shariati, F. New combination of triamcinolone, 5Fluorouracil, and pulsed-dye laser for treatment of keloid and hypertrophic scars. Dermatol Surg 32: 907-915, 2006. 9. Apikian, M., Goodman, G. Intralesional 5-fluorouracil in the treatment of keloid scars. Australas J Dermatol 45: 140-143, 2004. 10. Benkhaial, G. S., Cheng, K. M., Shah, R. M. Effects of 5-fluorouracil on collagen synthesis during quail secondary palate development. J Craniofac Genet Dev Biol 13: 617, 1993. 11. Bulstrode, N. W., Mudera, V., McGrouther, D. A., et al. 5-fluorouracil selectively inhibits collagen synthesis. Plast Reconstr Surg 116: 209-221; discussion 222-203, 2005. 12. Fitzpatrick, R. E. Treatment of inflamed hypertrophic scars using intralesional 5FU. Dermatol Surg 25: 224-232, 1999. 13. Gupta, S., Kalra, A. Efficacy and safety of intralesional 5-fluorouracil in the treatment of keloids. Dermatology 204: 130-132, 2002. 14. Kontochristopoulos, G., Stefanaki, C., Panagiotopoulos, A., et al. Intralesional 5fluorouracil in the treatment of keloids: an open clinical and histopathologic study. J Am Acad Dermatol 52: 474-479, 2005. 15. Nanda, S., Reddy, B. S. Intralesional 5-fluorouracil as a treatment modality of keloids. Dermatol Surg 30: 54-56; discussion 56-57, 2004. 16. Uppal, R. S., Khan, U., Kakar, S., et al. The effects of a single dose of 5fluorouracil on keloid scars: a clinical trial of timed wound irrigation after extralesional excision. Plast Reconstr Surg 108: 1218-1224, 2001.