Preliminary Diagnosis To save wasted Doctor time and avoid the
advertisement

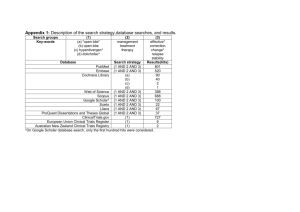
Preliminary Diagnosis To save wasted Doctor time and avoid the frustration of working on a treatment plan that is not accepted by the patient, the technique of making a preliminary diagnosis has been created. The possibilities of wasting time increase as we consider the many options of dentofacial orthodontics, surgery, and orthodontics being presented to a patient. A PRELIMINARY diagnosis should give enough basic information to do the 2nd consultation, get a decision from the patient, and start the case (get some brackets on, similar to quick start). AFTER the final decision has been made, then the treatment plan is finalized and the appliance is confirmed. If an instructor or mentor gives you a preliminary diagnosis, he/she may return the “preliminary IPsoft file” making it easier for you to order the appliance, or they may wait for your (email) reply to finalize the file, avoiding confusion with multiple files passing back and forth. EXAMPLE #1 of this approach. I have included for your information a screenshot of the picture tab for this patient only as information for you to understand what the preliminary diagnosis options. Note: the dentofacial vto is a line drawing from a ceph vto, turning off the x-ray. ** Orthodontic option: Extract upper 5s, class II molar finish, restore lower 6s. suggested: P90K + restorative of lower 6s ** Dentofacial option: more $ for ortho, no restorative. Extract upper 6s (and later 8s?), go with first molar occlusion. NO restorative, close the spaces and retract the teeth further. Zygoma bone plates to retract and intrude upper teeth. also raising her smile. Suggested: P140K Orthodontics: Ext U5s+8s Dentofacial: ext U6s (missing L6s) case can be started with Incisor torque for Ext 6/6: Li/SLi 150 grams per side upper zygoma - KH, step 3 lower to close ext space. Use UP lower 7s, tipD upper 7s. Incisor torque for Ext upper 5s, class II finish. Li/SLi+10 deg gable on lower. Step 2/3, open coil on 18x25N to upright 37/47, place small ss closed coil, allowing some retraction of the lower incisors. use Roth lower 7s, tipD upper 6s. Appliance below is for dentofacial. ______________________________________________________________________ Below are screenshots of the photo tab just for your information. Example case #2: email from McGann to the Progressive Orthodontic clinic in Manila There are several approaches to this MAJOR case, and I want your feedback before I write a treatment plan that takes me a lot of time and then find out that you/they are not doing this. So please advise from this information and I will complete the treatment plan of choice. you can start the case with these brackets 5-5, extract 4s, size bands and order later. Works for both options. Non extraction: forget it, finishes even more protrusive. Bicuspid Extraction 4/4: "orthodontics", WITH GROWTH to reduce some of the class II. no skeletal anchorage, no corticotomy. Protrusion remains, but I do not see this obvious problem on your list of complaints, nor on your list of goals. She will have a "toothy" look with excess vertical (and gingival display). 2-2.5 years Multiple extraction 6+4s: Best look. Dentofacial orthodontics, more expensive (2x orthodontic option), longer treatment time (3-3.5yrs), zygoma skeletal anchorage, no corticotomy. Solves protrusion, will NOT have a 'toothy' look since the smile will be 'raised'. lower 8s may need to be uprighted in finishing? Information to understand the case (not sent with comments)