Breakdowns - Nottingham University Hospitals NHS Trust
advertisement

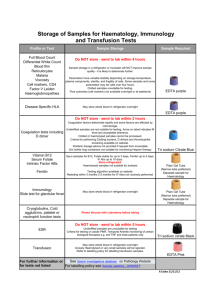
Clinical Pathology Service Directory
PUBLISHED August 2011
Revision Version 5
The electronic version of this directory is updated annually.
Uncontrolled copy if printed
NUHCLP-LI-GEN015
Page 1 of 62
Nottingham University Hospitals NHS Trust
Clinical Pathology Directory
This book contains information about the laboratory and diagnostic services
available at the City Campus and Queens Medical Centre Campus, Nottingham
University Hospitals, Nottingham. We provide a wide range of analytical and
advisory services, which are available for inpatients, outpatients and the
community at large. As you would expect from a large teaching hospital this
service is backed up with training and research programmes designed to
improve patient care.
To ensure the highest standard of work we participate in extensive internal and
external quality assurance schemes, and Clinical Pathology Accreditation (CPA)
UK Ltd.
We hope you find this directory useful and we look forward to providing you with
our services.
Page 2 of 62
Contents
Page
General Information
4
Clinical Pathology
10
a)
b)
c)
d)
e)
Clinical Chemistry
Haematology
Blood Transfusion
Immunology
Molecular Diagnostics
10
36
46
51
55
Point of Care Testing (POCT) Devices
56
Vacutainer Guide
59
Page 3 of 62
GENERAL INFORMATION
Useful Telephone Numbers
City Ext
QMC Ext
General Enquiries Clinical Pathology
Results for Clinical Chemistry,
Results for Haematology
Results for Immunology
Blood Bank
Transfusion Practitioners
General Enquiries; Pathology
55082
55591/2
55591/2
55560
55858
56195
63087/61168
63087/61168
63087/61168
63087/61168
63660
67704/65366
63592
Hospital Porters
56009
63350
SPECIMEN TRANSPORT
Within the Hospital
Please use the pneumatic tube system whenever possible, except for
emergencies, high-risk samples, blood cultures, and precious samples, such as
CSF. This is the quickest route to get samples to the laboratory. The hospital
porters will collect large specimens (e.g. 24hr urine collections) daily (Monday to
Friday) from all wards and clinics. For urgent specimens please see individual
laboratory requirements.
Reporting Faults
Any member of staff noticing a fault in the pneumatic tube system should report
it to the Property Services Department, Ext 55900 at City campus between the
hours of 8am-4.30pm Mon-Fri.
At QMC Campus bleep 84 3224 (Pathology) 9.00 till 5.00 Monday to Friday and
bleep 84 3202 (Estates Engineers) at all other times including weekends and
bank holidays.
All stations have a notice attached to the front requesting that a system failure be
reported to the Maintenance Helpdesk on Ext 55900 at City campus and bleep
the appropriate number 84 3224, or 84 3202 at Queens Medical Centre campus.
Out of hours the on call Shift Craftsman should be bleeped via switchboard.
Lost Specimens
Any member of staff who suspects that a sample is lost in the pneumatic tube
system must act as quickly as possible.
The laboratory is not responsible for samples that do not arrive in the
laboratory. (For security reasons laboratory staff are instructed not to leave
the laboratory to retrieve samples that subsequently appear at destinations
other than their own). It is the responsibility of the requester to ensure
delivery of the specimen to the laboratory.
Page 4 of 62
Ward staff should speak personally to the person who physically put the
sample into the tube, to establish which station was used to send the sample,
what time the sample was sent and to which address the sample was sent.
Ward staff should then contact the maintenance engineer giving details of
where and when the sample was sent to allow the engineer to track where
the sample is in the system by interrogating the computer operating the
system.
If the situation cannot be resolved by this means, the Property Services
Manager (Ext 56856 at City campus and BLEEP 84 3224 9.00-5.00 and 84
3202 at Queens Medical Centre campus or, if out of hours, the on-call
Property Services Manager at City Hospital Campus should be contacted via
switchboard and made aware of the situation.
Please Note: High-risk specimens and blood cultures must not be sent in
the pneumatic tube. They should be taken to Pathology Reception.
Out of hours blood cultures should be placed in the incubator in the
cupboard outside Pathology Reception.
From General Practitioners
A daily van service is available to collect samples from General Practitioners
served by the Nottingham University Hospitals. For further information on this
service please contact Specimen Reception on Ext. 56195 at City campus and
Ext 63039 at Queens Medical Centre campus.
REQUEST FORMS
For General Practitioners there is a single request form for all routine Clinical
Pathology (Chemistry, Haematology, Immunology) and Microbiology services.
Other Departments have their own request forms.
There are specific forms for certain specialised services (e.g. Antenatal Down’s
Syndrome and Haemoglobinopathy Screening), which you are strongly advised
to use.
A “High Risk" sticker must be attached to the request form for all designated
high risk samples.
Whichever form you use please:
Write clearly at all times: this prevents errors of interpretation.
Use Patient Addressograph labels whenever possible.
Page 5 of 62
Clearly identify yourself: this makes contacting you straightforward and
is essential for all transfusion requests (include telephone number/bleep
number).
Always complete the form and sample containers.
Always provide the time and date for a specimen: vital information for
interpreting some results.
Provide clinical information when requesting: saves time, helps
interpretation and may determine which analyses are performed.
Provide accurate and complete information where requested.
For Transfusion samples please write the information on the bottles
from direct questioning of patient or from the wristband. Bottles with
pre-printed identity labels will not be accepted by the Blood Transfusion
Laboratory.
For the supply of request forms please contact Specimen Reception (Tel. Ext
56195 at City campus and Ext 66512 at Queens Medical Centre campus)
BLOOD SAMPLES
An Inpatient and Out-Patient Phlebotomy Service is available:
Inpatient Phlebotomy Service
A hospital based phlebotomy service is available every day of the year except for
Christmas Day, New Years Day and Bank Holidays. The QMC Campus offers an
emergency/urgent service on New Years Day for ward based patients only.
Doctors wishing to use the inpatient phlebotomy service should request the tests
using the electronic pathology ordering system. Labels will then be printed on
the appropriate ward and available for the phlebotomists before 8.30 a.m.
The phlebotomists will visit each ward only once in a morning and will take
specimens for all pathology tests (except for blood cultures, gentamicin and
vancomycin levels) on Mondays - Saturdays, but will only take urgent Clinical
Chemistry, Haematology and Blood Transfusion specimens on Sundays and
Bank Holidays.
Outpatient Phlebotomy Service
An open access phlebotomy service is provided in the Outpatient Department,
City Campus, Monday - Thursday, from 8.00 a.m. to 5.00 p.m. and Friday from
8.00 a.m. to 2.00 p.m. (excluding Bank Holidays) and at QMC Campus, adjacent
to the Main Entrance, Monday-Wednesday 8.30am-5.30pm, Thursday 8.30am6.00pm and Friday 8.30am-2.00pm.
No prior appointment is required. Hospital Doctors and General Practitioners
who wish their patients to be bled in the Outpatient Department should give their
patients a fully and accurately completed request card(s). The patient can then
attend the hospital Outpatient Phlebotomy Department to be bled. Please refer
to the individual sections to ensure that the patient is fully aware of any special
Page 6 of 62
requirements (e.g. fasting overnight) before they attend the Outpatient
Department. GP patients should try to avoid busier times if possible, e.g.
Monday, Wednesday, Thursday or Friday mornings. Any morning between 8.00
a.m. - 9.00 a.m. is generally a quieter time. Any further information concerning
phlebotomy please contact Ann Booton, Phlebotomy Co-ordinator, Ext. No.
66579.
Taking Specimens Yourself
Please ensure that all specimens are taken under the correct conditions,
appropriate preservative used and any special requirements adhered to. All staff
who take samples for blood transfusion must be trained and competency
assessed in accordance with the requirements of the NPSA Safer Practice
Notice 14. Please contact the transfusion practitioner team to arrange training.
The individual sections of this book should give you the information you require
but if in doubt please telephone the appropriate department. We use the
vacutainer system for taking blood, and the different types of tubes available are
shown on pages 52-55 of this book.
In order to reduce the chance of cross-contamination with anticoagulants
and consequent misleading results, please take samples in the
following order:
clotted
citrate
lithium heparin,
EDTA and fluoride oxalate samples.
If taking blood cultures in addition to other samples, the blood culture bottles
should be inoculated first to prevent contamination.
LABELLING OF SAMPLES / SAMPLE ACCEPTANCE CRITERIA
Please note that samples (for BT sample labelling see Transfusion Policy) must
be labeled with at least three essential patient identification points on the sample
and the request card should have at least four essential patient identification
points before a request can be accepted for analysis. Please refer to the
following table for guidance.
Page 7 of 62
SAMPLE
ESSENTIAL
Surname
First Name (Not initial)
Plus at least one of the
following:
-Unique Identifier number
-Date of Birth
REQUEST FORM
DESIRABLE
Time sample taken
Date sample taken
Unique Identifier or Date
of Birth (When in
addition to the essential
criteria)
ESSENTIAL
DESIRABLE
Surname
First Name (Not initial)
Time sample taken
Date sample taken
Patient’s gender
Name of requesting
doctor
Signature of requesting
doctor
Clinical information
Full Address
Patient’s phone number
Consultant or GP
Destination for report
Campus
Hospital and referral lab
number (if referred
sample)
Plus at least two of the
following:
-Unique Identifier number
-Date of Birth
-1st line of address.
On rare occasions a specimen may be processed without complete information
where there would be a risk to the patient in obtaining a further sample e.g. a
CSF, pleural aspirates etc. Such specimens would be referred to a senior
member of the laboratory staff to approve for analysis; this may introduce a
delay.
UNLABELLED, MISLABELLED AND INADEQUATELY LABELLED
Samples that are inadequately labeled or mislabelled will be rejected and the
standard laboratory report will be issued with an appropriate message.
24 HOUR URINE SAMPLES
When collecting 24-hour urine samples please ensure that the correct bottles are
used (see individual sections). The bottles may be obtained from Pathology
Specimen Reception.
N.B. Important Safety Note - some bottles contain concentrated acid as
preservative, which will cause burns when in contact with skin. Make sure
this acid is not discarded and warn the patient to take care to avoid
spillage. In addition, please ensure the patient is instructed not to urinate
Page 8 of 62
directly into the bottle. Ask the patient to use a wide-necked jug or jar and
then pour the urine into the 24-hour collection bottle.
Please ensure that collections are complete (the date and time they were
started and finished should be provided) and not contaminated by faeces or
blood.
ORDERING AND REPORTING OF PATHOLOGY RESULTS
Within the hospital the quickest and most reliable process for ordering is
electronic using NotIS Orders. Electronic Ordering guarantees an electronic
report.
Electronic results are also available to General Practitioners. For
further information about this please see the ICT website (search for NotIS) or
contact the ICT helpdesk (Ext. 69000). Abnormal results (according to criteria)
are telephoned to the ward or relevant GP.
NB: If a sample is urgent the laboratory needs to be informed by telephone
before the sample is received in the laboratory. Failure to do so will mean the
results will not be telephoned unless they fulfill the criteria for telephoning
abnormal results.
RESEARCH
All Departments are involved in research projects, both academic and
commercial. If you are considering undertaking any research or trial work
involving Pathology specimens, please contact the individual Department.
VISITING DEPARTMENTS
If you wish to visit one of the Departments we will be happy for you to do this.
Simply telephone the appropriate Manager/Head of Department to arrange an
appointment.
QUALITY ASSURANCE
Every effort is taken to ensure that the correct result on the right patient is
returned to the requesting clinician with the minimum of delay. To ensure this
high quality of service all departments participate in all relevant External Quality
Assurance Schemes, and make strenuous efforts to have vigorous internal
quality control checks. In addition, all the Pathology Departments have been
accredited by CPA (Clinical Pathology Accreditation) UK Ltd.
LOCATION
Clinical Pathology is located opposite Junction P3 (Physiotherapy corridor
junction 3) at the City Campus and on A floor West Block at the Queens Medical
Centre Campus.
Page 9 of 62
CLINICAL PATHOLOGY DEPARTMENT
DEPARTMENTAL MANAGEMENT
Clinical Lead
Professor Noor Kalsheker MB, ChB, MSc, MD
Ext 78330720 noor.kalsheker@nuh.nhs.uk
Clinical Pathology Service Manager
Mrs. Karen Jones MSc, CSci, FIBMS, MinstLM
Ext 64929
Pathology Quality Manager
Ms Liz Bakowski
FIBMS
Ext 57187 City
or 62538 QMC
karen.jones@nuh.nhs.uk
liz.bakowski@nuh.nhs.uk
CLINICAL CHEMISTRY SECTION
ENQUIRIES
General Enquiries (City campus) Ext 55082 or 57271
Facsimile
Direct 0115 8402664
Clinical Pathology Helpdesk
Ext 63087/61168
LABORATORY ENQUIRIES
Results Enquiries (City campus) Ext 55592
(QMC campus) Ext 63087
Urgent Requests
City campus (24 hours)
QMC campus (24 hours)
Ext 55592
Ext 64932
Bleep 7053
Bleep 1360
Duty Biochemist (Clinical Advice)
City campus
Ext 59729
QMC campus
Ext 63087
Bleep 7796
Consultant on-call (out-of-hours) via Switchboard
Consultant Chemical Pathologists
Professor Noor Kalsheker MB, ChB, MSc, MD
Ext 78330720 noor.kalsheker@nuh.nhs.uk
Dr Peter Prinsloo, MBCHB, MRCP, FRCPath
Ext 55079
peter.prinsloo@nuh.nhs.uk
Page 10 of 62
Consultant Clinical Scientists
Dr Tony Hitch MA, PhD, FRCPath, CSci
Ext 55087
Principal Clinical Scientists
Dr Stephanie Barber BSc, PhD, FRCPath
Ext 63094
Mrs Angela Whitehurst MSc, DipRCPath
Ext 55080
Dr Marian Hill BSc (Hons), PhD
Ext 66593
tony.hitch@nuh.nhs.uk
stephanie.barber@nuh.nhs.uk
angela.Whitehurst@nuh.nhs.uk
marian.hill@nuh.nhs.uk
LABORATORY SECTION HEADS
Automated
Mr. David Ingram
FIBMS DMLM
Ext 64447
Mr Alan Grey, FIBMS
Ext 64900
david.ingram@nuh.nhs.uk
Mr Nigel Dennis MSc, FIBMS
Ext 55592
nigel.dennis@nuh.nhs.uk
Immunochemistry
Ms Susan Taylor MSc, FIBMS, CSci
Ext 57021
Chromatography
Mr Fin Hollingworth MSc, FIBMS Ext 55581
susan.taylor@nuh.nhs.uk
Toxicology
Mr Kevin Quilter FIBMS
Ext 63411
Immunology
Mr Simon Martin BA (Hons), FIBMS, CSci
Ext 61654
alan.grey@nuh.nhs.uk
finlay.hollingworth@nuh.nhs.uk
kevin.quilter@nuh.nhs.uk
simon.martin2@nuh.nhs.uk
GENERAL INFORMATION
Clinical Chemistry provides a comprehensive diagnostic service and also
provides some specialised services to the whole of the UK. A summary of the
more common tests routinely performed, including reference ranges and
collection details is given on pages 20-29. Details on more specialised tests
undertaken are available via the Duty Biochemist (Bleep 7796) at City campus
and Ext 63087 at Queens Medical Centre campus.
Page 11 of 62
LABORATORY OPENING HOURS
A 24 hours shift system is in operation for general chemistry tests and consultant
advice is available, out of hours, via switchboard. The following routine tests are
available 24 hours per day:U&E’s, Liver Function Tests, CK, LDH, Calcium, Phosphate, Glucose, Amylase,
Osmolality,
CRP,
Protein,
Salicylate,
Paracetamol,
Theophylline,
Carbamazepine, Phenytoin, Magnesium, Urate, Bicarbonate, Chloride,
Pregnancy Tests, Iron (suspected poisoning only), Lactate, Ammonia, Lithium,
Troponin I, Digoxin, Glucose,CSF Protein and Bile Acids.
It is not necessary to bleep or telephone if the results are required within 2 – 3
hours. The results will be routinely available as provisional reports on Notis as
soon as they have been technically validated. If results are required more
urgently please follow the instructions in the next section.
Please note: It is departmental policy that all grossly abnormal results which
may affect immediate clinical management are telephoned to the requesting
doctor if a bleep number or telephone extension is written on the request form,
otherwise they will be telephoned to the ward or consultant’s secretary. For GP
patients the abnormal results will be telephoned to the surgery.
The laboratory on the City Campus is located opposite Junction P3
(Physiotherapy corridor junction 3). Please see www.ncht.org.uk/clinpath or
http://citynet/clinpath for further details.
The laboratory on the Queens Medical Centre Campus is located on A Floor
West Block.
URGENT REQUESTS
There is a limited repertoire for urgent tests available 24 hours per day with most
of the test results being available in approximately 30 minutes after receipt of the
specimen. This service is only available to medically qualified staff, who MUST
telephone (Ext 55592 at City campus or Ext 64932 at Queens Medical Centre
campus before the sample arrives in the laboratory. Unless this procedure is
adopted the sample will not be treated urgently. Requests including those
received from GPs. will not usually be telephoned unless the results are grossly
abnormal and fall outside our telephone limits. Please do not abuse this service
as it stretches the resources of the department, and most routine test results are
ready within 2 – 3 hours of receipt. The list of tests available urgently is the
same as that in the previous section. Other tests may be performed urgently at
the discretion of the Duty Biochemist (during core hours) or Consultant on-call
(out of hours).
Page 12 of 62
HIGH RISK SPECIMENS
If the patient is known to be, or suspected of being, HIV, Hepatitis B or C
positive, or falls into a high risk category please use a BIOHAZARD bag for the
transportation of the sample to the laboratory. A limited repertoire of tests is
available for high-risk samples. DO NOT USE THE PNEUMATIC TUBE FOR
HIGH RISK SAMPLES.
ADVICE ON INTERPRETATION AND INVESTIGATIONS
During CORE hours (9.00am – 6.00pm at City campus, 9.00- 5.30pm at QMC
campus) a Duty Biochemist is available to give advice on appropriate testing and
the interpretation of results (Ext 59729/Bleep 7796 at City campus or Ext 63087
at QMC campus). There is an out of hours Consultant Advisory Service available
via the Hospital Switchboard. Guidelines are available for the investigation of
certain metabolic and endocrine disorders. Copies of these protocols are
available on the departmental website or by contacting Ext 55082.
SPECIALISED TESTS
A wide range of additional tests is available to investigate metabolic, endocrine,
gastroenterological and paediatric problems. Further information about these
tests can be obtained by contacting the Duty Biochemist (Ext 59729/Bleep 7796
at City campus or 63087 at QMC campus).
RESEARCH STUDIES AND CLINICAL TRIALS
A wide range of analyses are performed for research studies, ranging from
molecular biology, receptor analysis, endocrinology, bone metabolism, lipids and
cancer studies. Please contact Ext 55082.
PAEDIATRIC SERVICE
All the tests listed on pages 19-27 are available on children, and where known,
any paediatric reference ranges are included in the alphabetical list. If several
tests are to be performed on a single specimen, please try and provide 1 mL of
blood. If you can only provide very small quantities of blood, please indicate
the priority of the tests to be performed.
INVESTIGATIONS OF INBORN ERRORS OF METABOLISM
Routine screens for Inborn Errors of Metabolism (IEM) are performed at the City
campus. The tests are performed throughout the week and the results of all the
tests are usually reported on Thursday and Friday. For urgent tests please
contact the Duty Biochemist (Ext 59729). In an emergency investigations may
also be carried out at other times (weekends, evenings and bank holidays). This
requires discussion with the On-Call Consultant. The Department is fully
committed to Quality Assurance and participates in all the appropriate National
and European External Quality Assurance Programmes.
Page 13 of 62
Apart from a comprehensive analytical service the Department provides an
interpretative and advisory service giving expert advice on the interpretation of
results and appropriate investigations.
Contact numbers:
Dr Peter Prinsloo (Consultant Chemical Pathologist)
Angela Whitehurst (Principal Biochemist)
Donna Fullerton (Senior Biochemist)
Inborn Error Laboratory
Duty Biochemist
Ext 57271
Ext 55080
Ext 55080
Ext 57031
Ext 59729
IEM INVESTIGATIONS
The Department undertakes a comprehensive range of tests on each sample
sent for a IEM screen, which will enable the majority of disorders to be detected,
ranging from urea cycle disorders, amino acid metabolism defects and numerous
organic acid disorders through to mucopolysaccharide abnormalities, sugar
disorders and storage diseases.
If an inborn error of metabolism is suspected please send a fresh urine sample
(at least 5mL) for an IEM Screen along with a 1mL Lithium Heparin plasma
sample for plasma amino acids. Clinical details are vital to enable interpretation
of results.
The following tests are done on all urine specimens sent for an IEM screen;
-
Spot tests
Dipstix
pH, Protein, Glucose, Ketones, Blood, Sulphite
Reducing Substances
2,4 DNP
Nitroprusside
FeCl₃
DMB (Total glycosamino glycans)
Creatinine (urate:creatinine + GAG: creatinine ratios)
Amino Acids: 2D TLC & Full Quantitation by amino acids analyser
Organic acids: GCMS qualitative analysis
Sugar chromatography
Oligosaccharide chromatography
Sialic acid chromatography
Mucopolysaccharide 1D electrophoresis
Remember: A 6mL sample of fresh urine is required for all of the above
analyses.
Routine Blood/Plasma tests available include:
Page 14 of 62
-
Plasma amino acids (2D TLC and quantitation)
Gal-1-PUT (Galactosaemia screen)
Biotinidase
Free fatty acids/3-OH Butyrate
Insulin/C-Peptide
A 1mL lithium heparin sample is required for PAA analysis
A 1mL lithium heparin sample is required for Gal-1-PUT analysis
A 1mL lithium heparin or clotted sample is required for biotinidase analysis
A 1mL fluoride oxalate sample is required for FFA/3-OH Butyrate analysis
A 1mL clotted sample is required for Insulin/C-Peptide analysis
Occasionally the analysis of faeces may be required. We provide the following
tests routinely:
-
Faecal pH
Faecal sugar chromatography
A pea sized amount of faeces is required for the above analysis.
Referred Investigations
We enjoy close working relationships with the National Centres for the
investigations of IEM, and regularly liaise with Birmingham, Sheffield, Leeds,
Great Ormond Street and Manchester for certain investigations or for the
confirmation of our own findings. Many of these tests require specific sample
types, collection details etc, therefore prior contact with the laboratory is advised.
IMMUNOSUPPRESSANT DRUG MONITORING
Sample requirements
-
Ciclosporin and FK506 (Tacrolimus) analyses are available every
weekday (Monday – Friday).
Samples should be in the Clinical Pathology Department at the City
Campus by 12:00noon Monday to Friday for analysis on the same day.
-
An EDTA plasma sample is required with a minimum sample volume
of 100 uL whole blood.
-
Every effort will be made to obtain a result on small, paediatric
samples
-
Please state on the request form if the sample is a trough or 2 hour
post-dose sample and also if the patient is on IV
Ciclosporin/Tacrolimus.
Page 15 of 62
-
Analysis is not routinely available at the weekend. Requests for the
analysis of urgent samples at the weekend need to be made on a
Consultant to Consultant basis by 5.00pm on Friday.
Adult Target Ranges - Ciclosporin
Purpose
Sampling
Adult renal
Transplant
Range
(ng/ml)
Reference
Trough
95-205
2hr post-dose (C2)
(Target)
1month
2months
3months
4-6months
>6months
1500
1300
1100
900
700
Neoral C2 Consensus meeting
London, December 2003. Based on
Modified MO2ART Trial ranges
Trough
Trough
95-200
150-250
NCH Clinical Guideline No. 600
Author Dr J. Byrne
Trough
IV
300-400
250-450
Gastroenterology, 118 (2)
p572,2000 and 120 (6); P13231329,2001.
Trough
100-200
<200
Expert Opinion
BJD 2002; 147; 122-129
1000
800
600
Biodrugs, 15; p279-290, 2001
Haematology
Sibling allograft
MUD patients
Gastroenterology
Ulcerative
Colitis
Dermatology
Chronic urticaria
Psoriasis
Liver Transplant
2hr post-dose (C2)
0-3 months
4-6 months
>6 months
Adult Target Ranges – Tacrolimus (FK506)
Purpose
Sampling
Adult renal
Transplant
Trough
Range (ug/L)
5-15
Page 16 of 62
Reference
A ORAL GLUCOSE TOLERANCE TEST
A glucose tolerance test can be performed on the ward, or in general practice.
The patient should have fasted for 12 hours prior to the start of the test and the
GTT baseline blood specimen should be taken before 10.00 a.m. A 75g glucose
load is then given, and a further blood specimen taken 2 hours later.
Important points:
The patient should eat a normal diet (>150 g carbohydrate daily) for at least 3
days prior to the test, and undertake normal physical activity.
In adults, the glucose load (75g) can be given as 410ml of Lucozade Energy
Original (to check that you have the correct formulation, check the Nutritional
Information label, the drink should contain 70kcal/100ml). Using this exact
type of Lucozade is vital; other Lucozade drinks are not suitable.
The patient should have fasted for at least 12 hours immediately prior to the
test. Water as required is permitted.
Ensure that the patient then remains seated for 2 hours, without eating,
drinking or smoking. The test is invalid if these conditions are not imposed.
2 hours after administering the glucose/Lucozade, collect a second venous
blood sample for glucose.
Please ensure that all staff involved in undertaking any elements of this test
have been provided with suitable training and are assessed to be competent.
Complications and Limitations
If the patient vomits during the 2 hour period, the test cannot be completed
unless this happens towards the end of the test (after 1 hour).
A low sugar diet prior to the OGTT may lead to a more normal result than that
obtained on a normal diet.
Interpretation
Fasting glucose
2-hour
glucose
Normal
< 6.1mmol/L
and
< 7.8 mmol/L
Impaired fasting glycaemia
(IFG)
≥ 6.1 and < 7.0 and
mmol/L
< 7.8 mmol/L
Impaired glucose tolerance
(IGT)
< 7.0 mmol/L
and
≥ 7.8 and < 11.1
mmol/L
Diabetes mellitus
≥ 7.0 mmol/L
and/or
≥ 11.1 mmol/L
Diabetes: All diagnoses need confirmation by a second diagnostic result on
another day (previous or subsequent to the OGTT); unless the patient is
symptomatic.
Page 17 of 62
Impaired fasting glycaemia and impaired glucose tolerance: Are regarded as risk
factors indicating an increased long-term probability of developing diabetes,
rather than diagnoses in their own right.
For further advice or interpretation of OGTT results please contact the Duty
Biochemist on: 0115 969 1169 extension 59729 (City Hospital) or
0115 924 9924 extension 63087 (Queen’s Medical Centre).
MYELOMA
We measure IgG, IgA and IgM quantitatively, plus perform capillary zone
electrophoresis on all specimens requesting immunoglobulins or protein
electrophoresis. Any new positive paraprotein screen results will automatically
have immunofixation performed to type the paraprotein which will also be
quantitated. When considering myeloma as a diagnosis please remember to
send a plain urine sample (25mL in a Universal container) for Bence-Jones
Protein. In some patients both the plasma and urine screens may be negative,
in these cases please consider the possibility of a non-secreting myeloma.
These can be diagnosed by examination of Bone Marrow Aspirate/Trephine.
If cryoglobulinaemia is suspected, and the plasma and urine screens are both
negative please take a 5mL clotted blood sample and send to the laboratory
under special conditions to keep the sample warm (see page 20 for further
details).
TUMOUR MARKERS
The Department offers a number of different assays that are used as ‘tumour
markers’. Whilst the measurement of a wide range of analytes can be useful in
certain circumstances, the term ‘tumour marker’ is usually applied to a specific
set of circulating molecules. Assays available during routine Laboratory hours
are; AFP (alpha fetoprotein),CEA (carcinoembryonic antigen), CA125, CA153,
CA199, HCG (human chorionic gonadotrophin) and PSA (Prostatic Specific
Antigen). The laboratory also measures Immunoglobulins and Bence Jones
Protein (for myeloma screening), Urine Catecholamines and Urine
Metanephrines
(for
screening
for
phaeochromocytoma)
and
5
hydroxyindoleacetic acid (screening for carcinoid syndrome) and Thyroglobulin.
The measurement and interpretation of tumour marker levels is not
straightforward. The following general points should be considered when
requesting any tumour marker.
-
-
Requesting of multiple markers (such as CEA and the CA series of
antigens) in an attempt to identify primary cancer is rarely indicated.
No serum marker currently in use is specific for malignancy.
Serum marker levels are rarely elevated in patients with early
malignancy. High levels are usually found only when patients have
advanced disease.
No cancer marker has absolute organ specificity. PSA however,
appears to be relatively specific for prostate tissue.
Page 18 of 62
-
Apart from possibly HCG in choriocarcinoma, no marker is elevated in
100% of patients with a particular malignancy.
Reference ranges for cancer markers are not well defined and are
used only for guidance in serum samples. Please note that a level
below the reference range does NOT exclude malignancy while
concentrations above the reference range does not mean malignancy
is present. Changes in levels over time are more clinically useful than
absolute levels at one point in time.
DOWN’S SYNDROME (21) screening
Markers are measured in the serum of pregnant women to provide a risk
estimate for Down’s Syndrome (Trisomy 21) in the first or second Trimester of
pregnancy. Testing for neural tube defects (NTD) should be by ultrasound scan.
For Down’s syndrome screening please use the special forms available;
information relating to the pregnancy is absolutely required to calculate the risk.
Please complete the forms as accurately and completely as possible – failure to
provide sufficient information will result in testing not being performed. We are
part of the Nottingham Antenatal Screening Steering Group, and follow the
National Screening Committee’s (NSC) Guidelines for Laboratories performing
Downs Syndrome Screening. Users will be alerted to changes to the screening
program in line with NSC Guidelines.
SCREENING FOR PORPHYRIA
Suspected Acute Attack
Fresh urine for PBG screen
and total porphyrins
Suspected
cutaneous Fresh urine for PBG screen
porphyria
and
faeces
for
total
porphyrins.
Suspected
Erythropoietic Fresh urine for PBG screen
Protoporhyria
and
faeces
for
total
porphyrins
5ml
EDTA
specimen
for
total
plasma/erythrocyte
porphyrins
Family Studies
Fresh urine, faeces and
EDTA
whole
blood
depending on type
Page 19 of 62
Protect from light
Protect from light
Protect from light
Please
contact
laboratory
the
TESTS AND TURNAROUND TIMES
Investigation
Sample Type
Turnaround Times
Reference Range
Comments
Unless otherwise stated assays are performed daily. Out aim is to report 97.5% of ED tests within 60
minutes and 85% of P1 / urgent automated results within 60 minutes. 85% of routine automated
results from inpatients within 120 minutes and 85% of GP / OPD tests within 180 minutes. For the
correct tube type please see tube guide.
ACTH
5mL EDTA
7 days
Up to 46 ng/L
Acylcarnitine
21 days Urgent
500L plasma or
analysis can be
1mL blood or 4
done within 7 days.
spots min
For urgent analysis
contact laboratory.
Sample referred
Alanine Transaminase
2mL Serum/SST
180 minutes
Female Up to 35U/L
(ALT)
Male
Up to 45U/L
Albumin
2mL Serum/SST
180 minutes
30 – 50 g/L
Alcohol
2mL Serum/SST
180 minutes
Aldosterone & Renin
5mL EDTA + 5mL 14 days
Aldosterone
clotted
Upright
111-860pmol/L
Supine
55-440 pmol/L
Do not send
Higher values seen in children
samples on ice
Up to 1yr
140-3660pmol/L
1-8y
110-2110pmol/L.
Also see Renin
Alkaline Phosphatase
2mLSerum/
180 minutes
Adults 40 - 130 U/L
(ALP)
5mLSST
Children 100-400I/L
Alkaline Phosphatase
2mL Serum/
7 days
Isoenzymes
5mL SST
Alpha-1-Antitrypsin
5mL Serum/EDTA 24 hours
1.1-2.1g/L
Alpha fetoprotein
5mL Serum/
24 hours
Tumour marker: Up to 10kU/L
(AFP)
5mL SST
Alpha 1 Acid
5mL SST
7 days
0.5-1.4 g/L
Glycoprotein
a-Galactosidase
5mL EDTA or
21 days
Please contact laboratory before
2mL Plasma
Sample referred
sending. An EDTA whole blood
sample is required, with specific
sending and storage conditions to a
referral laboratory.
Aluminium
Z5/Z10
21 days
Up to 60 µg/L - little risk of toxicity in
Polypropylene
Sample referred
chronic renal failure.
Over 60 µg/L - excessive
accumulation, risk of toxicity in
children.
Over 100 µg/L - cause for concern,
high risk of toxicity in children.
Over 200 µg/L - high risk of toxicity in
all patients.
Amino Acids
1mL Li-Hep
7 days
For urgent analysis
contact laboratory
Amino Acids (urine)
Minimum 6mL
7 days
fresh urine
For urgent analysis
contact laboratory
Ammonia
5mL Li-Hep
60 minutes
Up to 4 weeks
Up to 100 µmol/L
Notify laboratory
5 weeks and older Up to 40 µmol/L
prior to collection
Amylase
2mL Serum/
180 minutes
Up to 110 U/L
5mL SST
Androstenedione
5mL Clotted
7 days
Adults: Up to 10.8 nmol/L
Pre-pubertal: Up to 1.8 nmol/L
Pubertal: Up to 7.7 nmol/L
Angiotensin
5mL Clotted
7 days
8-52 U/L
Converting
5mL SST
Enzyme (ACE)
Page 20 of 62
60 – 120 minutes
depending on
status. Contact lab
if urgently
required out-ofhours
7 days
180 minutes
Anti-Glomerular
Basement Membrane
Abs (Anti GBM)
Screening Test (See
Immunology Table)
5mL Clotted
Anti TPO
Asparate
Transaminase (AST)
Arsenic
5ml Clotted
2mL Clotted
5mL SST
Arylsulphatase A
5mL Li-Hep whole
blood
Beta-2-microglobulin
Bence Jones Protein
Bicarbonate
Bilirubin
Bile Acids
Bilirubin (Total and
Conjugated)
Biotinidase
Blood Gases
Bone Profile
CA 125
CA 153
CA199
Caeruloplasmin
25mL Urine or
24hour collection
if quantitation
required
2mL Clotted
5mL SST
2mL Clotted
5mL Clotted/
5mL SST
2mL Clotted/
5mL SST
500l Serum/LiHep plasma
5mL Clotted/
5mL SST
5mL Clotted/
5mL SST
5mL Clotted/
5mL SST
5mL Clotted/
5mL SST
5mL Clotted
5mL SST
28 days
Sample referred
Contact lab to
discuss
8 weeks
Sample referred
7 days
3 days
Results reported as positive,
negative or equivocal. Positive and
equivocal samples are quantitatively
analysed by ELISA following working
day
Up to 60 kU/L
Female up to 30 U/L
Male
up to 35 U/L
1.8-24µmol/hr/mg protein
180 minutes
19 – 28 mmol/L
180 minutes
24 hours
Up to 21 µmol/L
Up to 6 mol/L.
Action limit Over 14 mol/L.
Total Bilirubin Up to 21 mol/L
Conjugated Bilirubin Up to 6 mol /L
180 minutes
7 days. For urgent
analysis please
contact laboratory
Must be received
within 30 mins of
sampling
Please Use Blood Gas Machines in Ward Areas
180 minutes
Profile Includes Albumin, Calcium,
Phosphate and Alkaline phosphatase
24 hours
Up to 35 kU/L
24 hours
Up to 35 kU/L
24 hours
Up to 35 kU/L
7 days
0.2-0.6 g/L
Therapeutic Range 25-40mg/L
Toxicity generally does not occur
until level exceeds 80mg/L.
Diet Dependent 2.5 - 7.5 mmol/24h
on normal diet (20mmol/L Ca per
day)
Up to 15 ng/L
Caffeine
2mL Clotted
Calcium
2mL Clotted
7 days
For urgent analysis
please contact
laboratory
180 minutes
Calcium (Urine)
24h Acid or Plain
24 hours
Calcitonin
5mL Li-Hep
Carbamazepine
2mL Clotted
21 days
Sample referred
Contact Lab First
180 minutes
Page 21 of 62
Adult adjusted calcium reference
range
2.2 – 2.6 mmol/L
Children’s adjusted calcium
reference range
0 to 1 month 2.00 – 3.00 mmol/L
1 mon to 1 yr 2.10 – 2.90 mmol/L
1 yr to 16 yrs 2.20 – 2.70 mmol/L
Therapeutic
Toxic
4 – 12 mg/L
Over 15 mg/L
Carbon Monoxide
5mL Li-Hep
IN house use blood
gas analyzer.
Outside hospital for
urgent analysis
please contact
laboratory
21 Days
Sample referred
Non-smokers - Up to 1.5 %
Smokers (1-2 packs/day) Up to 5.0%
Heavy Smokers (>2 packs/day) Up to
9.0%. Symptoms of toxicity may be
expected at levels greater than 20%.
Carbohydrate Deficient
Glycoprotein
Syndrome
Carcinoembryonic
Antigen (CEA)
2ml Serum
5mL Clotted/
5mL SST
24 hours
Up to 2.5 µg/L
Please note values up to 10.0 g/L
can be frequently seen in smokers
and patients with non-malignant GI
and liver disease.
Carnitine
300L Plasma
Catecholamines
(Urine)
24h Acidified
urine sample
21 Days
Sample referred
7 days
CCP antibodies
5ml SST
Chloride
2mL Clotted
5mL SST
24h Plain
180 minutes
96 – 109 mmol/L
24 hours
110 – 250 mmol/24h
5mL Clotted/
5mL SST
4mL Whole Blood/
0.5ml
serum/plasma
4mL EDTA Whole
Blood
5mL
serum/clotted
180 minutes
Please see guidelines
5mL Li-Hep
14 days
Contact Lab First
5mL EDTA
See C3, C4 &
C3D
5mL Clotted
5mL Clotted
5mL Clotted
Not SST tube
12 hours
See section on immunosuppressants
24 hours
24 hours
7 days
0.75 – 1.65 g/L
0.14 – 0.54 g/L
Male
12-22 mol/L
Female
13-30 mol/L
Patients on oral contraceptives or
HRT
22-40 mol/L
Copper in Urine
Cortisol (serum)
24 hr urine
5mL Clotted/
5mL SST
21 days
24 hours
Please note time
on form and if
patient on steroid
therapy or if it is a
dexamethasone
suppression test
Cortisol (Urine)
24h Plain
14 days
Chloride (Urine)
Cholesterol
Cholinesterase
Phenotype/activity
Cholinesterase
Genotype
Cholinesterase for
Suxamethonium
Sensitivity
Cholinesterase for
Organophosphate
Poisoning
Ciclosporin
Complement
C3
C4
Copper
7 day TAT
Results reported as Positive /
Negative with interpretative comment
Normotensive Ref.Range
Noradrenaline Up to 430 nmol/24h
Adrenaline Up to 70 nmol/24h
Dopamine Up to 2700 nmol/24h
<4 units per ml
28 Days
Sample referred
28 Days
Sample referred
14 Days
Sample referred
Page 22 of 62
8.00 to 9.00 a.m. 110 – 530 nmol/L
Midnight
Up to 250 nmol/L
Lower levels expected later in the
day "Please note lower cortisol
reference range in GC-MS aligned
assay from 19/04/2010. lower values
are expected later in the day. Cortisol
less than 420 nmol/L 30 minutes
post-Synacthen
suggests
an
inadequate response".
50 – 250 nmol/24hr
C Peptide
5mL Clotted
Creatine Kinase (CK)
2mL Clotted /
2ml Li-Hep /
5mL SST
2mL Clotted /
2ml Li-Hep /
5mL SST
Creatinine
Creatinine (Urine)
Creatinine Clearance
C-Reactive Protein
(CRP)
CSF Neurotransmitters
CTX
Cystine (Urine)
Dehydroepiandrosterone sulphate (DHEAS)
2mL Clotted
Drug Screen (Urine)
Ethanediol (Ethylene
Glycol)
25mL Random
2mL
Fluoride/oxalate
Elastase
(Faecal/Pancreatic)
Ethanol (see Alcohol)
1g Faeces
Faecal Sugars
(See Reducing
Substances Faeces)
Ferritin
364 – 1655 pmol/L
180 minutes
Male
Female
Newborn
Infant1
Child
Adolescent
Male
Female
Female
Male
24h Plain/
24 hours
10mL random
24h Urine collection plus 2mL Clotted/LiHep or 5mL SST at time of the urine
collection
5mL Clotted
180 minutes
5ml Li-Hep
Specific
28 days
containers
Sample referred
obtained from
Contact lab to
providing lab
discuss
5mL Clotted
7 days
Fasting Sample
must be in lab
within 3 hours.
24hr Plain
7 days
5mL Clotted
7 days
Digoxin
Faecal Occult Blood
7 days
Collect sample for
insulin and blood
glucose at the
same time.
To lab promptly!
180 minutes
2mL
Fluoride/oxalate
Pea size amount
of fresh faeces
Pea size amount
of fresh faeces
180 minutes
NB: Specimen
must be taken at
least 6h after dose
3 days
24 hours
Contact lab to
discuss
28 Days
Sample referred
2-3 days
7 days
24 – 170 U/L
24 – 145 U/L
Male
Female
70 – 120 µmol/L
55 – 100 µmol/L
27 - 88 mol/L
8 - 35 mol/L
27 – 62 mol/L
44 – 88 mol/L
7.1-17.7 mmol/24h
5.3-16.9 mmol/24h
80 – 125 mL/min
90 – 140 mL/min
Up to 10 mg/L
Male
Female
Pre-menopausal
Post-menopausal
Up to 0.64 g/L
Up to 0.57 g/L
Up to 0.92 ug/L.
Male
2.2-15.2 mol/L
Female
Pre-menopausal
0.9-11.6 mol/L
Post-menopausal 0.8-7.0 mol/L
NB: In children less than 10yrs
values up to 4.0mol/L expected.
Therapeutic level
0.5-1.0 g/L
Toxic level
>2.5 g/L
Qualitative assay
Confirmation by GC-FID
Qualitative assay
7 days
2mL Clotted/
5mL SST
24 hours
FK506
(Tacrolimus)
5mL EDTA
Folate
Folate (Red cell)
Follicle Stimulating
5mL Clotted
5mL EDTA
5mL Clotted/
12 hours
NB:Collect sample
immediately
before next dose
24 hours
7 days
24 hours
Page 23 of 62
Male
Female
9mths – 16yrs
Target Range
3.9 – 14ug/L
Up to 220ug/L
Follicular
25 – 350 µg/L
12 – 300µg/L
10 – 89 g/L
5 – 15 µg/L
1.5 – 11.4 U/L
Hormone (FSH)
5mL SST
GAL-1-PUT Screen
(Galactosaemia
screen)
1mL Li-Hep
Whole Blood
-Glutamyl Transferase
(GT)
Gastrin
2mL Clotted/
5mL SST
5mL Clotted
Send promptly to
lab
Glucose
2 mL
Fluoride/oxalate
See Separate
section
2mL
Fluoride/oxalate
Glucose Tolerance
Tests ( OGTT)
Glucose (CSF)
Gonadotrophins
Glycated Haemoglobin
Human Chorionic
Gonadotrophin (HCG)
5mL Clotted
5mL Whole Blood
EDTA / Li-Hep
5mL Clotted
5mL SST
Ovulatory
Luteal phase
PostMenopausal
Pregnant
Male
3.4 – 34.2 U/L
1.1 - 9.5 U/L
23.0-132.9 U/L
Up to 0.3U/L
1.4 - 18.1 U/L
7 days
Female
Male
Fasting levels
Up to 40U/L
Up to 55U/L
25 – 115 mU/L
180 minutes
Fasting
3 days
If required
urgently please
contact Duty
Biochemist
180 minutes
180 minutes
180 minutes
Blood Glucose
should be sent as
well
See FSH & LH
24 hours
Growth Hormone
5mL Clotted
24 hours
Can be done within
90 minutes if
urgently required
7 days
Gut Hormone Screen
(VIP, Pancreatic
polypeptide, GAWK,
Gastrin, Somatostatin)
Haptoglobin
HbA1c
Contact lab first
for special tubes
28 days
Sample referred
5mL Clotted
5mL Whole Blood
EDTA / Li-Hep
5mL Clotted/
5mL SST
5ml EDTA Whole
Blood
5ml EDTA – to lab
within 30 mins
Fluoride-oxalate
during
hypoglycaemic
episode
24 hours
24 hours
High-Density
Lipoprotein (HDL)
Hexosaminidase A
Homocysteine
3-Hydroxybutyrate &
Free fatty acids
5-Hydroxyindole-acetic
acid (5-HIAA)
7-Dehydrocholesterol
24h urine
Plain or Acid
5 mL Li-Hep
17- OH-progesterone
(17-OHP)
5mL Clotted/
5mL SST
If required
urgently please
contact Duty
Biochemist
24hr urine
Hydroxyproline
3.0 – 6.0 mmol/L
180 minutes
28 Days
Sample referred
7 days
7 days
If required
urgently please
contact Duty
Biochemist
14 days
28 days
Sample referred
14 days
Sample referred
28 days
Sample referred
Page 24 of 62
2.8-4.4 mmol/L (approx 60-80% of
Plasma glucose value.
Non-Diabetics
4 -5.9 %
Diabetes–Good Control Up to 7 %
Tumor marker
Up to 2U/L
Also see section on antenatal
screening for further information
Random growth hormone levels are
variable. If an abnormality is
suspected stimulation / suppression
tests are indicated.
0.3-2.0 g/L
Non-Diabetics
4 -5.9 %
Diabetes–Good Control Up to 7 %
Male
Over 0.9 mmol/L
Female
Over 1.3 mmol/L
Age related reference ranges on
reports
Up to 50 µmol/24h
Normal Neonates Up to 13 nmol/L
Stressed/Preterm Up to 40 nmol/L
Adults (basal)
Up to 13 nmol/L
Adults (60 min post Synacthen)
Up to 20 nmol/L
CAH values
over 100 nmol/L
Up to 300 mol/24h
Immunoglobulins
IgG
IgA
IgM
5mL Clotted
24 hours
Adult Ref Range
IgG
5.3 - 16.5 g/L
IgA
0.7 – 4.0 g/L
IgM
0.5 - 1.9 g/L
IgG/Albumin Ratios
7 days
Paired serum and
CSF required.
5 days
IgG/Albumin Ratios
Immunofixation
(serum and urine)
Inborn Error Screen
7 days
Urgently by
arrangement
Insulin-like Growth
Factor 1 (IGF-1)
Minimum 6mL
fresh random
urine and
1mL Li/Hep blood
5mL Clotted send
promptly to lab
Insulin
5mL Clotted
Iron
5mL Clotted/
5mL SST
Iron Binding Capacity
Lactate
5mL Clotted
2mL
Fluoride/oxalate
0.5mL
Fluoride/oxalate
2mL Clotted
5mL SST
7days
Collect sample for
blood glucose at
the same time
180 minutes
(Toxicity screening
only)
24 hours
90 minutes
Lactate in CSF
Lactate
Dehydrogenase
(LDH)
Lamotrigine
Laxative Screen
Lead
Lipase
Lipids
Lithium
5mL Clotted
20mL fresh urine
5mL EDTA
5mL SST
2mL Clotted/
5mL SST
5mL Clotted/
5mL SST
7 days
Performed automatically if suspicious
band seen on protein electrophoresis
or BJP analysis
0-6 years 31-154 g/L
7-9 years 54-308 g/L
10 years
92-385 g/L
11 years
131-462 g/L
19-39yrs
122-400 g/L
40-54yrs
75 – 306 g/L
55yrs and older 48-225 g/L
6-25 mU/L
Female
9-31 µmol/L
Male
12-31 µmol/L
Toxicity
Over 50
45 – 76 µmol/L
Venous 0.5 - 2.0 mmol/L
Arterial
0.5- 1.6 mmol/L
90 minutes
180 minutes
220 - 450 U/L
7 days
14 days
14 days
Contact lab to
discuss
180 minutes
180 minutes
Therapeutic
Qualitative
Children
Adults
180 minutes
12h-Post Dose
Prophylactic
0.4-1.2 mmol/L
Chronic use
0.4-1.2 mmol/L
Acute Mania
Up to 1.3 mmol/L
Up to 15 mg/L
Up to 0.5 µmol/L
Up to 0.9 µmol/L
Up to 300 U/L
See Cholesterol and Triglycerides
Liver Function Tests
(LFTs)Includes
ALT/GGT/ALP/Bili/Alb/
Total Protein
Luteinising Hormone
(LH)
2mL Clotted/
5mL SST
180 minutes
5mL Clotted/
5mL SST
24 hours
Lysosomal enzymes
5mL EDTA
28 Days
Whole Blood
Sample referred
2mL Clotted/
180 minutes
0.7 - 1.0 mmol/L
5mL SST
Clotted Sample. FSH and Oestradiol combined are the best markers of the
Magnesium
Menopause Testing
Page 25 of 62
Follicular
0.8 – 12.5 U/L
Midycle
8.6 – 76.3 U/L
Luteal phase
0.5 – 16.9 U/L
Pregnant
Up to 1.5 U/L
Post Menopausal 15.9 – 72.6 U/L
Male
1.5 - 18.1 U/L
Children
Up to 6.0 U/L
Mercury
Metanephrines
Methanol
Methotrexate
Microalbumin
Albumin:Creatinine
Ratio(ACR)
Mucopolysaccharide
Electrophoresis and
Glycosaminoglycans
Myeloma Screen
Myosis Screen
Neopterin
Neuroblastoma screen
Oestradiol
Oligosaccharides
(Urine)
Osmolality (Serum)
Osmolality (Urine)
Oxalate (Urine)
Paracetamol
Paraprotein
quantitation
(serum + urine)
Parathyroid Hormone
(PTH)
Paraquat (Diquat)
Peroxisomal Enzymes
Phenobarbitone
Phenylalanine/
Tyrosine
Phenytoin
Phosphate
Phosphate (Urine)
Porphobilinogen
(Urine)
menopause. LH is not useful. If on HRT, oestradiol assays are only of use when
monitoring implant therapy with oestradiol itself - gonadotrophin assays do not
offer much information.
5mL Li-Hep whole 28 days
blood or urine
Contact lab to
discuss
24hr Urine Acidif
14 days
collection
2mL
3 days
Fluoride/oxalate
If required
urgently please
contact Duty
Biochemist
5mL Clotted
2 days
Contact Lab First.
OOH request
through
consultant ONLY
10mL Fresh urine
24 hours
Male Up to2.5 mg/mmol creat
Female Up to 3.5 mg/mmol creat
Minimum 6mL
fresh random
urine
5 mL Clotted + 25
mL Urine
10mL fresh urine
5mL acidified
random urine
5mL Clotted/
5mL SST
7 days
48 hours
ON Request
14 days
Protect from Light
14 days
Urgent if required
24 hours
6mL Fresh Urine
7 days
2mL Clotted/
5mL SST
20mL Fresh Urine
24h acidified urine
180 minutes
5mL SST
24 hours
28 days
Sample referred
180 minutes
5 days
5mL EDTA
24 hours
10mL fresh urine
within 4 hours of
ingestion
5mL EDTA Whole
Blood
5mL Clotted/SST
100L Lith-Hep
Plasma
2mL Clotted
2mL Clotted/
5mL SST
24h Acid or Plain
20mL for full
screen
180 minutes
Contact Lab First
28 days
Sample referred
3 days
3 days
180 minutes
180 minutes
24 hours
24 hours
Contact Lab if
required out-of-
Page 26 of 62
Request IG / Protein
Electrophoresis(serum)
+ BJP (urine)
Follicular
40 – 606 pmol/L
Midcycle
253 – 1930 pmol/L
Luteal phase
121 – 804 pmol/L
Post Menopausal up to172 pmol/L
Male
up to 191 pmol/L
Female
275 - 295 mOsmol/kg
Male
280 - 300 mOsmol/kg
50 - 1200 mOsmol/kg
100-460 mol/24h
Performed when monoclonal band
identified on protein electrophoresis
or BJP analysis
14 – 72 ng/L
Qualitative
Therapeutic
Up to 45 mg/L
Therapeutic
10 – 20 mg/L
Adults 0.8-1.4 mmol/L
Children’s ref range on report form
13 – 42 mmol/24h
Porphyria Tests
Porphyrins (Blood)
Porphyrins (Faeces)
Porphyrins (Urine)
Potassium
See section on
investigation for
porphyria
5ml EDTA
Sample must be
protected from
light
5g Faeces
Sample must be
protected from
light
10mL Urine
Sample must be
protected from
light
2mL Clotted/5mL
SST
hours
21-28 days
Samples referred
21 Days
Sample referred
7 days
7 days
Potassium (Whole
blood)
Potassium (Urine)
Pregnancy Test (Urine)
Pregnancy Test
(Blood)
P1NP (Procollagen I
Extension Peptide)
P3NP(Procollagen III
N-terminal Peptide
Progesterone
Prolactin
2mL Li-Hep
180 minutes
Do not store
unseparated
samples in fridge
180 minutes
24h Plain
10mL Fresh Urine
2mL Clotted/SST
24 hours
24 hours
24 hours
25 – 125 mmol/24hr
5mL Clotted
14 days
5mL SST
14 days
Male
Female
2.3-6.4 g/L
5mL SST
5mL Clotted/
5mL SST
24 hours
24 hours
Prostate Specific
Antigen (PSA)
5mL Clotted/
5mL SST
24 hours
Purine and Pyrimidine
Screen
Purine and Pyrimidine
Confirmation
1mL urine
28 Days
Sample referred
28 Days
Sample referred
5mLThymol
preserved urine
5ml EDTA Blood
Pyruvate
Reducing substances
(in Faeces) –
Qualitative analysis for
faecal sugars
Reducing substances
(in Urine) - Qualitative
analysis for urine
sugars
Renin
Rheumatoid Factor
Salicylate
Selenium
Pea size amount
of fresh faeces
3.5 - 5.3 mmol/L
Haemolysis and old specimens will
give falsely high values
19-84 g/L
20-76 g/L
7 days post-ovulation over 40 nmol/L
Females
Non-pregnant
60-620 mU/L
Pregnant
206-4420 mU/L
Post Menopausal
38-430 mU/L
Male
45-375 mU/L
Up to 50 Years
Up to 2.5 g/L
50 - 59 Years
Up to 3.0 g/L
60 – 69 Years
Up to 4.0 g/L
70 – 79 Years
Up to 5.0 g/L
Not routinely
available. Discuss
with Paediatric
Biochemist
7 days
6mL fresh random
urine
7 days
5mL EDTA/5mL
Li-Hep
Fresh sample
Do not send
sample on ice
5ml Clotted/ SST
2mL Clotted/ SST
5mL Clotted
14 days
8.3 – 46.3mU/L
See Aldo / Renin
24 hours
180 minutes
7 days
Page 27 of 62
Up to 1 Year
0.36-1.00 mol/L
Sex Hormone Binding
Globulin (SHBG)
5mL Clotted
7 days
Sirolimus
Sodium
5mL EDTA
2mL Clotted/
5mL SST
24h Plain
7 days (referred)
180 minutes
Sodium (Urine)
Renal Stone Analysis
Sweat Test
Tacrolimus
Testosterone
24 hours
2-15 years
0.60-1.80 mol/L
16yrs & Older 0.80-2.00 mol/L
Female
19-131 nmol/L
Male
12.9-61.7 nmol/L
NB: Higher values (up to 200 nmol/L)
may be seen in women on HRT, Oral
Contraceptives or during pregnancy.
134 - 145 mmol/L
40-220 mmol/24h
Drug and dietary dependent
Qualitative
Stone in universal 14-21 days
container
Sample referred
Performed as required: Please telephone ext 57271 or55082 for appointment
5mL EDTA
12 hour
(Whole Blood)
Collect sample
immediately before
next dose
5mL Clotted
24 hours
Female
Up to 2.8 nmol/L
Male
8 – 27 nmol/L
Theophylline
2mL Clotted
180 minutes
Collect sample at
least 8hours post
dose or immediately
before the next
dose.
7 days
24 hours
Therapeutic Adults
Neonates
Thyroglobulin
Thyroid Function Tests
(TFT)
Thyroid Stimulating
Hormone (TSH)
Free Triiodothyronine
(Free T3)
Free Thyroxine
(Free T4)
Total Protein
5mL Clotted/SST
5mL Clotted/SST
2mL Clotted/
5mL SST
180 minutes
Total Protein (CSF)
Total Protein (Other
Fluids)
Total Protein (Random
Urine) –
Protein:Creatinine
Ratio(PCR)
Total Protein (Urine)
Transferrin Iso-electric
Focusing
Triglycerides
0.5mL Plain Tube
Fresh specimen
In Universal –5mL
20mL Fresh Urine
180 minutes
180 minutes
Up to 1 month
50-70 g/L
1-12 months
52-75 g/L
1 year and older
60-80 g/L
150-450 mg/L
See Light’s criteria on report
24h Plain
2mL Clotted or LiHep
5mL Clotted/SST
24 hours
21 days
Sample referred
180 minutes
Troponin I
180 minutes
Urea
5ml Clotted/SST
(12x hours after
onset of chest
pain)
5mL Clotted/SST
Urea (Urine)
Uric Acid (Urate)
24h Plain
5mL Clotted
24 hours
90 minutes
Uric Acid (Urate)
(Urine)
24h Neutral
24 hours
24 hours
180 minutes
Page 28 of 62
10 - 20 mg/L
5 - 10 mg/L
Up to 0.9g/L
Free T4
10.0-19.8 pmol/L
TSH
0.3 – 5.50 mU/L
Free T3
3.5-6.7 pmol/L
Normal
Up to 15 mg /mmol creat
Trace
15-44 mg/mmol creat
Proteinuria 45-299 mg/mmol creat
Nephrotic >300 mg/mmol creat
Up to 0.15 g/24hr
Fasting Female 0.4 – 1.53 mmol/L
Fasting Male 0.45 – 1.81mmol/L
0 – 0.04 µg/L
Adults
Up to 60yr
2.0-6.5 mmol/L
Over 60yr
2.9-7.5 mmol/L
Children
Up to 1 month 1.4-4.3 mmol/L
430 – 710 mmol/24h
Female
150 – 350 mol/L
Male
200 - 420 mol/L
1.5 - 4.5 mmol/24h
Valproate
Urine Thiosulphate
Vasoactive Intestinal
Peptide (VIP)
Very Long Chain
Fatty Acids (VLCFA)
Vitamin A
Vitamin B12
Vitamin B 1 (Thiamine)
5mL Clotted
6mL fresh random
urine
Contact lab first
for special
trasylol tubes
500L Li-Hep
2mL Clotted
Sample must be
protected from
light
5mL Clotted
Contact Lab First
Vitamin B 3
(Riboflavin)
Vitamin B 6
(Pyridoxine)
Vitamin C
Contact Lab First
25 OH Vitamin D
5mL Clotted
Vitamin E
2mL Clotted
Sample must be
protected from
light
5mL Li-Hep
Whole blood
White Cell Cystine
Contact Lab First
Contact Lab
First
White Cell Enzymes
5mL EDTA Whole
blood.
Xanthochromia in CSF
Sample must be
protected from
light
5mL Clotted
Not SST tube
Zinc
24 hours
14-21 days
Sample referred
28 days
Sample referred
21 Days
Sample referred
7 days
24 hours
28 days
Sample referred
28 days
Sample referred
28 days
Sample referred
56 days
This assay is not
routinely available
7 days
7 days
Therapeutic
Up to 100mg/L
<30 pmol/L
Up to 5years
5 -10 years
Adult
0.5 - 1.7 µmol/L
0.7 - 1.7 µmol/L
1.3 - 2.9 µmol/L
190 - 800 ng/L
24 – 167 nmol/L
Values of less than 30 nmol/L are
considered insufficient.
Values of less than 15 nmol/L are
considered deficient.
Up to 5years
12.5-24.5 mol/L
5-10years
12.0-22.5 mol/L
Adult:
14.0-30.0 mol/L
48 days
Sample referred
Sample must
reach the lab by
4pm Monday to
Thursday only
30 days
Sample referred
Collect sample
Mondays to
Wednesdays only
180 minutes
Contact Lab first
CSF Xanthchromia Service (see
below)
7 days
10 - 18 µmol/L
Page 29 of 62
Gentamycin
Take a blood sample (gold top serum separator tubes (preferred) or red
top) 18-24 hours after the 1st dose of 5 mg/kg.
o
This timing is crucial.
This sample should be labelled as a "Pre-dose"
Tobramycin
Take a venous blood sample (gold top serum separator tubes (preferred)
or red top clotted) immediately before the 2nd dose.
o
Capillary blood samples should NOT be used as they produce
unreliable results.
o
The timing is crucial.
This sample should be labelled as a "Pre-dose"
Vancomycin
Take a pre-dose sample (gold top serum separator tubes (preferred) or
red top tube 5ml). Post dose samples are NOT required.
The first assay should be taken just before the 3rd or 4th dose is due. The
sample should be labelled as a "pre-dose"
Specific requesting information for Antibiotics request forms will also need to be
set up with:
Antibiotic assays: Request cards.
These must include the following information to allow accurate
interpretation of the assay result:
Patient details
o
Name
o
Hospital number
o
Date of birth
o
Latest creatinine (& date)
Drug details
o
Antibiotic name
o
Dose of antibiotic prescribed
o
Frequency of dosing (once daily, twice daily..)
o
Times of doses
o
Indication
Page 30 of 62
Sample details
o
Date and time sample taken
o
Type of sample (pre-dose, post-dose, or random sample?)
o
Date and time of last dose of antibiotic
Failure to provide this information may result in the sample being rejected by the
lab, or incorrect interpretation of the assay result
CSF Xanthochromia Service
The protocol below is based upon the Revised National Guidelines for Analysis
of CSF for Bilirubin in Suspected Subarachnoid Haemorrhage (UK National
External Quality Assessment Scheme Specialist Advisory Group. Ann Clin
Biochem 2008; 45: 238-244) and the National Clinical Guidelines for Stroke,
(Royal College of Physicians. 2nd Edition 2004).
Subarachnoid haemorrhage should be considered in any patient presenting with
sudden-onset (“thunder-clap”), severe and unusual headache with or without
associated alteration in consciousness.
If SAH is suspected: 1. CT brain scan should be undertaken immediately if the patient has an
impaired level of consciousness and within 12 hours in all patients.
2. If the CT scan is negative or equivocal lumbar puncture should be
undertaken 12 or more hours after onset. (CSF for xanthochromia
screening must not be collected less than 12 hours after onset as
potentially misleading negative results may be obtained)
Sample Requirements
(Tubes must be sequentially numbered)
Tube No
Test required
Sample / tube
Minimum volume
1
CSF glucose
Fluoride tube
0.4mL
2
Microbiology
Plain Universal
2.5mL
3
Microbiology
Plain Universal
2.5mL
4
CSF protein
0.4 mL
5
CSF protein +
xanthochromia
CSF in plain
universal
CSF in plain
universal
1.0 mL
NB: Protect from
light
A blood specimen for glucose must be collected if CSF glucose estimation
is required.
All CSF samples from patients that do not require xanthochromia
screening should be sent to Clinical Pathology on either the City or QMC
Campus.
Page 31 of 62
If a xanthochromia screen is required, the CSF protein and CSF
xanthochromia will both be done at QMC Campus to conserve the
sample.
NB: CSF protein results on bloodstained CSF samples are unreliable.
A simultaneous blood specimen should be taken for serum bilirubin and
total protein measurement
Request Form
If CSF xanthochromia is required, it must state so on the request form, i.e.
a request for “CSF protein” will not automatically be sent for
xanthochromia.
Please indicate on the request form:
o
Clinical indication for request
o
Result of CT scan
o
Time of onset of symptoms/events
o
Time of lumbar puncture (Must be >12h post ictus)
If no order of priority is stated on the request form, CSF protein will be
measured first on the plain universal sample. If there is then insufficient
sample for xanthochromia, this will be reported as “insufficient”.
Transporting of samples to the laboratory
Samples for xanthochromia screening must be protected from light by
placing them within the normal plastic bag and then into a thick, brown
envelope addressed to Clinical Pathology at QMC / City Campus.
Pneumatic tube delivery systems should NOT be used to transport CSF
samples for xanthochromia screening to the laboratory.
Samples for xanthochromia screening must reach the laboratory within 1
hour of being collected.
Out-of-hour xanthochromia screening requests
QMC campus (out-of-hours)
Samples should be transported directly from the requesting ward to
Clinical Pathology at QMC Campus.
Do not use the pneumatic tube to transport these samples.
Please contact QMC Clinical Pathology laboratory on ext 64932 or page
the biomedical scientist in the laboratory prior to delivering the sample
City Campus (out-of-hours)
Page 32 of 62
Samples should be transported directly from the requesting ward at the
City Campus to Clinical Pathology at QMC Campus by taxi or other
transport arranged by the ward.
Please contact QMC Clinical Pathology laboratory on ext 64932 or page
the Biomedical Scientist in the laboratory prior to delivering the sample.
Samples should be delivered to the QMC Emergency Department
Reception on A floor with a request to contact Clinical Pathology on ext
64932 to notify them that the sample has arrived.
Xanthochromia Screening Service
The CSF xanthochromia service is provided on an “AS SOON AS
PRACTICABLE” basis on samples received in the laboratory.
The service is available for samples received at QMC Clinical Pathology
before 16h30 on weekdays, and before 12h30 on Saturdays, Sundays
and Bank Holidays.
On Saturdays, Sundays and Bank holidays it may occasionally be
necessary to contact the duty Biomedical Scientist via QMC switchboard
(61800) to arrange processing of the sample (only if the person is out of
the main laboratory at that point and is not able to answer on ext 64932)
Please state clearly the name and contact detail of the person to whom
the report should be phoned if required
Microbiology
Calls from users may also require information about testing in
Microbiology (including white cell counts)
Calls should be directed to the Microbiology Department for bacteriology
advice. The sample requirements are available from the microbiology
intra- and internet sites.
PAEDIATRIC IMMUNOGLOBULINS
Expected Immunoglobulin levels (g/L) (from PRU data)
Age
IgA g/L
IgG g/L
IgM g/L
Cord
<0.02
5.2-18.0
0.02-0.2
Weeks
0-2
2-6
6-12
0.01-0.08
0.02-0.15
0.05-0.40
5.0-17.0
3.9-13.0
2.1-7.70
0.05-0.2
0.08-0.4
0.15-0.7
Months
3-6
6-9
9-12
0.10-0.5
0.15-0.7
0.20-0.7
2.4-8.8
3.0-9.0
3.0-10.9
0.2-1.0
0.4-1.6
0.6-2.1
Years
1-2
2-3
3-6
0.3-1.2
0.3-1.3
0.4-2.0
3.1-13.8
3.7-15.8
4.9-16.1
0.5-2.2
0.5-2.2
0.5-2.0
Page 33 of 62
6-9
9-12
12-15
>15
0.5-2.4
0.7-2.5
0.8-2.8
0.75-3.9
5.4-16.1
5.4-16.1
5.4-16.1
6.0-15.0
0.5-1.8
0.5-1.8
0.5-1.9
0.4-2.7
PAEDIATRIC IMMUNOGLOBULINS
Expected Immunoglobulin levels (g/L) (from PRU data)
Age
IgA g/L
IgG g/L
IgM g/L
Cord
<0.02
5.2-18.0
0.02-0.2
Weeks
0-2
2-6
6-12
0.01-0.08
0.02-0.15
0.05-0.40
5.0-17.0
3.9-13.0
2.1-7.70
0.05-0.2
0.08-0.4
0.15-0.7
Months
3-6
6-9
9-12
0.10-0.5
0.15-0.7
0.20-0.7
2.4-8.8
3.0-9.0
3.0-10.9
0.2-1.0
0.4-1.6
0.6-2.1
Years
1-2
2-3
3-6
6-9
9-12
12-15
>15
0.3-1.2
0.3-1.3
0.4-2.0
0.5-2.4
0.7-2.5
0.8-2.8
0.75-3.9
3.1-13.8
3.7-15.8
4.9-16.1
5.4-16.1
5.4-16.1
5.4-16.1
6.0-15.0
0.5-2.2
0.5-2.2
0.5-2.0
0.5-1.8
0.5-1.8
0.5-1.9
0.4-2.7
ADD ON TESTS
It is our policy that where practicable, written add-on tests will be accepted to
reduce unnecessary phlebotomy for patients. A new request form must be
completed, including the requesting clinician, the test required, and the sample
number (obtainable from the results page on NotIS: lab numbers appear in the
form 0009M123456, where 9 is the current year, and "M" may be MNOPQ or R,
depending on the campus of origin). Requesters are advised to check with the
laboratory on issues of sample stability BEFORE making add-on requests. Only
critical add-on requests which affect immediate patient management will be
accepted by telephone. Full revised version now on Q Pulse
Tests
Maximum age of samples for analysis (assuming
previously centrifuged)
Tubes without gel (red top)
Amylase
4 days
Bicarbonate
1 hour
Bone
3 days (phosphate most
unstable)
Calcium
4 days
Page 34 of 62
Tubes with gel (gold top)
4 days
CK
4 days
CRP
7 days
Ferritin
2 days
Glucose
2 days (grey top only)
Iron
7 days
Lactate
LDH
LFT
Lipids
Phosphate
1 day (grey top only)
3 days
4 days
1 day (bilirubin most unstable)
2 days (HDL most unstable)
3 days
4 days
PSA
2 days
TFT
5 days (FT4 most unstable)
Troponin I
U&E
U&E (without K+)
12 hours
12 hours (K+ most unstable)
3 days
3 days
4 days
Page 35 of 62
CLINICAL PATHOLOGY DEPARTMENT
DEPARTMENTAL MANAGEMENT
Clinical Lead
Professor Noor Kalsheker MB, ChB, MSc, MD
Ext 78330720 noor.kalsheker@nuh.nhs.uk
Clinical Pathology Service Manager
Mrs. Karen Jones MSc, CSci, FIBMS, MinstLM
Ext 64929
Pathology Quality Manager
Ms Liz Bakowski
FIBMS
Ext 57187 City
or 62538 QMC
karen.jones@nuh.nhs.uk
liz.bakowski@nuh.nhs.uk
HAEMATOLOGY SECTION
Enquiries should normally be made to the “General Enquiries and Results”
numbers but specialised advice can be obtained from the following numbers:Ext
Direct Line
General Enquiries (City campus)
56037
0115 9628029
0115 9628037
QMC campus
63312
Result Enquiries (City campus)
55591
Bleep 7134 (5.30pm – 10.00pm
Mon – Fri and 9.00
– 5.30 weekends)
After 10.00pm please bleep 7054
(QMC campus)
63087
bleep 1340
Blood Transfusion (City campus)
55600/1
out of core hours
0115 9627770 or
0115 9627902 or
out of core hours
bleep 7054
63660
Bleep 1340 out of core hours
Transfusion Practitioner
55858 City
67704 QMC
Bleep via switch
Consultant Haematologists
Ext
Professor N H Russell, MD, FRCP, FRCPath
55564/55555
Dr J Byrne MRCP, MRCPath, PhD
55182/55152
Dr A P Haynes MD, MRCP, MRCPath
56704/55597
Dr A McMillan FRCP, FRCPath
54666
Dr E Das-Gupta BSc, DM, MRCP, FRCPath
54666 / Bleep 7095
Dr M Donohue MRCP, FRCPath
56704
Dr G Dolan MB,ChB, FRCP(Edin),FRCP(London),FRCPath 61187
Dr C Williams
54666
Dr. C Fox
(QMC campus)
Page 36 of 62
Consultant Paediatric Haematologist
Dr K Forman MB, ChB, MRCP, MRCPath
63637
Associate Specialist
Dr C Grimley BSc, MB, ChB, MRCP
67178
LABORATORY SECTION HEADS
Automated QMC Campus
Mr Alan Grey, FIBMS
64900
Automated City Campus
Mr David Anderson, MSc, FIBMS
61025
Blood Transfusion City Campus
Miss Linda Hoyland, MSc, FIBMS
55600
Blood Transfusion QMC Campus
Miss Linda Hoyland MSC FIBMS
63143
GENERAL INFORMATION
The Haematology Section provides a clinical and laboratory service for the
screening, diagnosis and management of blood disorders. This includes
Routine haematology
Coagulation investigations
Red cell investigations
White cell investigations
Blood transfusion
Routine tests are provided at both City Campus and QMC Campus laboratories.
The laboratories collaborate for specialist tests. Samples for all haematology
tests may be sent to either laboratory.
ADVICE ON INTERPRETATION, INVESTIGATION AND REFERRAL
The laboratory staff are happy to provide advice on interpretation of results.
Please telephone the laboratory at which the sample was analysed (City Campus
or QMC Campus) and ask to speak to the relevant Section Head. Medical staff
are available to help with clinical advice and further investigations. Please
contact the Haematology registrar on duty via switchboard in the first instance.
There is a registrar based at both City Campus and QMC campus (0900-1700
Mon-Fri). For out of hours advice contact the Haematology registrar on-call via
the switchboard of either campus. Haematology Consultants may be contacted
through the Haematology secretaries.
Page 37 of 62
TRAINING AND RESEARCH
The department is recognized by the Royal College of Pathologists and the
Health Professions Council, Council for Professions Supplementary to Medicine
for the training of both medical and scientific staff.
The participation of the laboratory in research studies and investigations for
clinical trials is a well established and actively encouraged process. Clinical Staff
wishing to make use of haematological investigations, as part of a research study
or clinical trial, must first contact the Clinical Lead (Prof N Kalsheker) or the
Laboratory Services Managers (Mrs. Karen Jones).
TEST AVAILABILITY
The laboratory provides a 24 hour, 7 day a week service for FBC, ESR,
coagulation screens, fibrinogen, D Dimers, malaria screens, sickle cell screens
and blood transfusion. Routine blood films are usually reviewed by completion of
the next working day. Films will be examined out of hours only if the
haematological results are grossly abnormal or the clinical urgency dictates.
Urgent blood films may be requested at any time. Results of requests are
transferred to the electronic results reporting system (NOTIS) shortly after
testing. Urgent requests should be telephoned to the laboratory.
Investigations requiring more technical expertise may be batched and performed
two to three times a week. If a test other than those listed above is required more
urgently this must be discussed with a member of the laboratory or Haematology
medical staff.
TELEPHONING RESULTS
The laboratory will automatically telephone results meeting the following criteria:
-
Unexpected Haemoglobin less than 8g/dL
All positive malaria screens
Newly diagnosed haematological abnormalities
All INR results >8.0
Other abnormal results will also be telephoned but will depend on the degree of
abnormality and clinical details of patients. If a GP surgery is closed results will
be telephoned to the Out of Hours service (NEMS/DEMS).
HIGH RISK SPECIMENS
If the patient is known to be, or suspected of being, HIV, Hepatitis B or C
positive, or falls into a high risk category please use a BIOHAZARD bag for the
transportation of the sample to the laboratory. DO NOT USE THE PNEUMATIC
TUBE FOR HIGH RISK SAMPLES.
Page 38 of 62
SPECIAL TESTS
Preparation and processing times for some special investigations are lengthy
and the laboratory staff need time to organise these. In these circumstances
please telephone the laboratory to arrange a specific time for the analysis.
BLOOD FILMS
The request for a blood film can either be initiated by the laboratory or the
clinician. The laboratory initiated request is usually in response to ‘flags’
produced by the automated machine. These ‘flags’ are set at different levels for
different patient groups. There is also a system in place to ensure a blood film is
made irrespective of the full blood count if the diagnosis, relevant history or
treatment record on the request form indicate this is required.
It is possible to make a definitive diagnosis from a blood film but more often it
aids in the differential diagnosis and indicates further tests that may be
necessary.
Some of the clinical indications for examination of a blood film include clinical
features suggestive of the following:
Unexplained anaemia or jaundice
Sickle cell disease or other haemoglobinopathy
Thrombocytopenia or neutropenia
Lymphoma or lymphoproliferative disorder
Myeloproliferative disorder
Disseminated intravascular coagulation
Acute or recent onset renal failure especially in a child
Signs of hyperviscosity or optic atrophy on retinal examination
Suspicion of bacterial or parasitic infection that can be diagnosed from a
peripheral blood film
Disseminated non haematopoietic cancer
Infectious mononucleosis, other viral infection
Inflammatory or malignant disease
Pyrexia of unknown origin
HAEMATINIC TESTS
Advice on the interpretation of results and management is provided by
Haematology medical staff.
MALARIA TESTING
Diagnosis of malaria is by microscopic identification of malarial parasites in thick
and thin blood films. In addition all first requests for malaria testing have a
malaria antigen screening test performed.
Page 39 of 62
Points to remember:
1. Request malarial parasites in all cases of fever and history of travel to, or
residence in, malarial zone.
2. Samples for malarial parasites can be taken at any time. One does not
have to wait for typical signs or symptoms – samples do not need to
coincide with rigors.
3. It is very important to send the sample to the laboratory promptly as false
negatives can occur if the films are made more than 4 hours after
venepuncture.
4. A negative test DOES NOT rule out malaria. A low level of parasitaemia
may not be seen on a single film examination.
5. Malaria antigen tests may give a false negative result, particularly in cases
of non-falciparum malaria.
6. Malaria antigen tests cannot differentiate between plasmodium vivax,
ovale and malariae.
7. All positive malaria samples are sent to reference laboratory for
confirmation.
COAGULATION
The coagulation section provides a comprehensive service for all aspects of
haemostasis and thrombosis.
Responsibility of interpretation of results lies with the requesting physician.
Haematology medical staff are happy to advise with interpretation of results,
assessing risk of haemorrhage or thrombosis, anticoagulation matters and use of
blood products/coagulation factors for correcting haemostasis.
Coagulation Screen
A basic coagulation screen is made up of an activated partial thromboplastin
time) APTT prothrombin time PT and a Thrombin Time (TT). Fibrinogen and DDimers are not measured routinely. These tests may be performed on the same
sample as the coagulation screen but should be requested separately. A blue
topped citrate tube is required for analysis.
Points to remember:
1. The citrate bottle needs to be filled to the line on the bottle.
2. Always state on request form if patient is receiving anticoagulants
3. An INR is only reported if the patient is on Warfarin. It is not reported as
part of a routine coagulation screen.
4. Neonates have different normal ranges
Page 40 of 62
D-DIMERS
D-Dimers are primarily used for assisting in the exclusion of venous
thromboembolism. They must only be interpreted in conjunction with a clinical
probability assessment (eg. Wells Score). An elevated D-dimer result may be
seen in numerous clinical situations and may not necessarily indicate
thrombosis. The test may also be of value in the assessment of disseminated
intravascular coagulation (DIC).
INR
Anticoagulation guidelines can be accessed on the trust intranet.
http://intranet/Divisions/Medicine/Anticoagulation/default.htm
FIBRINOGEN
Fibrinogen is measured by functional assay (Clauss). It is of value in assessment
of DIC, consumptive coagulopathies, massive transfusion coagulopathy and
investigating dysfibrinogenaemia.
THROMBOPHILIA TESTING
Clinical details must be included on the request form to enable the appropriate
tests to be performed. Requests may be rejected if testing is not indicated from
the clinical details supplied.
Three blue topped (citrate) tubes and 1 clotted (red) should be sent to Clinical
Pathology (haematology).
The thrombophilia screen is made up of the following panel:
Protein C
Protein S
Antithrombin
Factor V Leiden
Prothrombin gene 20210 mutation
Full coagulation screen
Lupus anticoagulant
Anticardiolipin antibodies
Testing of the full screen should not be done around the time of an acute venous
thromboembolic event or whilst the patient is on anticoagulants (tests should wait
until at least 6 weeks off warfarin). The results will rarely influence the
management. In the majority of cases management can be determined by
history alone.
Thrombophilia testing should be avoided in children unless there is a very strong
clinical indication for it. Testing parents may be an acceptable alternative.
A specialist thrombosis clinic for thrombophilia assessment and management is
held at the QMC. Referrals should be made to Dr Dolan or Dr Myers.
Page 41 of 62
Factor Assays
This is a specialist service used predominantly to assist with haemophilia
diagnosis and management. Requests for factor assays should be made through
the Haematology medical staff.
Heparin Induced Thrombocytopenia (HIT)
The diagnosis of HIT may be supported by detecting HIT antibodies in a patient’s
serum. All requests must be submitted with a completed HIT form (available from
coagulation laboratory) and be discussed with a member of the Haematology
medical staff.
Platelet Function Studies
Investigation of suspected platelet function disorders can be performed (PFA
100, platelet aggregometry). For details please discuss with a member of the
Haematology medical staff.
RED CELL INVESTIGATIONS
This section provides an extensive range of tests to support the diagnosis of
haemolytic disorders, haemoglonopathies and red cell enzymopathies.
Haemoglobinopathy Diagnosis
High performance liquid chromatography (HPLC), haemoglobin electrophoresis
and isoelectric focusing (IEF) are the techniques currently employed.
Haemoglobinopathy screening occurs in the following situations:
Universal antenatal screening is offered as part of National Sickle Cell and
Thalassaemia screening programme. Testing of the baby’s father is
sometimes required.
Neonatal (Guthrie test) taken around six days of age and processed in the
Neonatal screening laboratory in Sheffield.
Pre-operatively for patients of non-Northern Europe origin. For emergency
surgery a full blood count and sickle solubility test are performed. If the
solubility test is positive and the full blood count normal a major sickling
disorder such as homozygous sickle cell disease or sickle/ thalassaemia
is ruled out.
When blood film features are suggestive of a haemoglobinopathy
When requested in anyone of non-Northern European origin.
The following points should be borne in mind:
All patients tested for haemoglobinopathy must be consented for that test.
It is not possible to give a definitive diagnosis in all cases as some abnormalities
cannot be detected on routine laboratory tests currently available.
Page 42 of 62
Opportunistic screening of women of childbearing age prior to conception can
avoid distress associated with abnormality detected when pregnancy is
underway.
All new abnormalities will receive confirmatory testing using an alternative
technique.
Red Cell Membrane Disorders
A FBC, blood film and family history should be performed in the first instance.
EMA binding is performed when the diagnosis is not clear.
WHITE CELL INVESTIGATIONS
A complete range of techniques supporting the diagnosis of haematological
malignancies is provided. For further details contact the Haematology
Department.
Immunophenotyping and molecular studies
Immunophenotyping is performed in Clinical Pathology at the QMC Campus for
paediatric cases only. All adult immunophenotyping and molecular testing is
performed in the molecular diagnostics section of Cellular Pathology at the City
Campus. Samples sent to Clinical Pathology will be forwarded to molecular
diagnostics. Samples should only be sent after discussion with the Haematology
medical staff. Samples for testing should be less than 24 hours old.
Bone Marrow Tests
All requests for bone marrow tests should be made through the duty
Haematology registrar.
Page 43 of 62
Investigation
Investigation
Investigation
Investigation
Unless otherwise stated assays are performed daily. Out aim is to report 97.5% of ED tests within 60
minutes and 85% of P1 / urgent automated results within 60 minutes. 85% of routine automated
results from inpatients within 120 minutes and 85% of GP / OPD tests within 180 minutes. For the
correct tube type please see tube guide.
Anti Factor Xa
Contact Laboratory First
Antithrombin III
4 x 2.7mL Citrate 7 days
>80
APC Resistance
2.7mL Citrate
7 days
>2.5
Bleeding Time
2 - 9 minutes
Contact Laboratory to
arrange
Blood Count
4mL EDTA
180 minutes
Haemoglobin (Hb)
Male
13.0 – 18.0 g/dL
Female
11.5 - 16.5 g/dL
Male
0.40 - 0.54
Haematocrit ({PCV)
Female
0.37 - 0.47
Male
4.2 - 6.5 x 1012/L
Red Blood Cells (RBC)
Female
3.8 - 5.8 x 1012/L
84 - 102 fL
Mean Cell Volume (MCV)
28 - 33 pg
Mean Cell Hb (MCH)
30 - 35 g/dL
MCH Conc. (MCHC)
150 - 450 x 109/L
Platelets
4.0 - 11.0 x 109/L
White Blood Cells (WBC)
2.0 - 7.5 x 109/L
Neutrophils
0.04 - 0.40 x109/L
Eosinophils
0.01-0.15x109/L
Basophils
1.0-4.0x109/L
Lymphocytes
0.1 – 1.5 x 109/L
Monocytes
Vitamin B12 and Folate:
- Vitamin B12
5mL Clotted
24 hours
B 12
190 - 800 ng/L
- Folate
5mL Clotted
24 hours
Folate
3.9–14.0 µg/L
- Red Cell Folate
4mL EDTA whole 7 days
Red Cell
blood
Folate
Up to 220 µg/L
Coagulation Factor
Contact Laboratory First
Assays
2 x 2.7mL Citrate
D-dimers
2.7mL Citrate
4 hours
20-180 µg/L
Erythrocyte
4mL EDTA
24 hours
Male
1-7 mm/h
Sedimentation Rate
Female
1-13 mm/h
(ESR)
Factor V Leiden
2.7mL Citrate or
2 weeks
(prothrombin
4mL EDTA
g.20210G>A’ tested at
same time)
Ferritin
5mL Clotted
24 hours
Male
25-350 µg/L
Female
12-300 µg/L
Children
(9mths – 16yrs) 10-89 µg/L
Fibrinogen
2.7mL Citrate
4 hours
1.8 - 4.0 g/L
Glandular Fever Screen
4mL EDTA
24 hours
Glucose 6 - Phosphate
4mL EDTA
24 hours
4.6- 13.5 U/g Hb (at 37oC)
Dehydrogenase screen
G6PD assay
Haemoglobin A2 %
4mL EDTA
24 hours
1.5 - 3.5%
Haemoglobin F%
4mL EDTA
24 hours
1.5 - 3.5%
Haemoglobin S%
4mL EDTA
24 hours
Haemoglobinopathy
4mL EDTA
3 days
screen
Ham’s Test
Heinz Bodies
Heparin Induced
Thrombocytopenia (HIT)
screen
Immunophenotyping
INR
4mL EDTA
5mL Clotted
2.7mL Citrate
See PNH antibody
screen
24 hours
Discuss with Medical
Haematology Staff
Contact Laboratory First
4 hours
Page 44 of 62
Lupus Anticoagulant
Malaria parasites
Osmotic Fragility
(APTT) Activated Partial
Thromboplastin Time
Plasma Viscosity
2 x 2.7mL Citrate
4mL EDTA
2.7mL Citrate
7 days
4 hours
Contact Laboratory First
4 hours
Refer to report
4mL EDTA
24 hours
1.50 – 1.72cP
Investigation
Investigation
Investigation
Investigation
Unless otherwise stated assays are performed daily. Out aim is to report 97.5% of ED tests within 60
minutes and 85% of P1 / urgent automated results within 60 minutes. 85% of routine automated results
from inpatients within 120 minutes and 85% of GP / OPD tests within 180 minutes. For the correct tube
type please see tube guide.
Platelet function assay
Contact Laboratory First
(PFA 100)
PNH antibody screen
4mL EDTA
Contact Laboratory First
Protein C
2.7mL Citrate
7 days
70 - 130%
Protein S
2.7mL Citrate
7 days
Male
75 – 114 U/dL
Female
55-120 U/dL
Prothrombin
2.7mL Citrate or 2 weeks
g.20210G>A’ (Factor V
4mL EDTA
Leiden tested at same
time)
Prothrombin Time (PT)
2.7mL Citrate
4 hours
8-13s
Pyruvate Kinase Screen
Contact Laboratory First
and assay
Reticulocyte Count
4mL EDTA
24 hours
10-100 x 109/L
Sickle Solubility Test
4mL EDTA
24 hours
If urgently required
contact laboratory
Thrombin Time (TT)
2.7mL Citrate
4 hours
13-19secs
Thrombophilia Screen
3 x 2.7mL Citrate 10 days
+ Clotted sample
Urinary Haemosiderin
20 mL urine in
24 hours
plain universal
(first early
morning sample)
Zinc Protoporphyrin
4mL EDTA
48 hours
30-80 µmol/mol
(ZPP)
Page 45 of 62
BLOOD TRANSFUSION
All staff involved in the requesting, prescribing, processing and testing, collection
and administration of blood components must be familiar with the Trusts
transfusion policy and competency assessed in accordance with the
requirements of NPSA SPN14. This can be accessed on the intranet:
http://qwss01/sites/NUH/Guidelines/1267.doc
It should be noted that transfusion practice is now governed by UK legislation
and all transfusion practices must be compliant with this.
The principles of Blood Transfusion practice are laid down in the Department of
Health
‘Handbook
of
Transfusion
Medicine’,
available
at
www.transfusionguidelines.org.uk
The transfusion laboratory provides the following services:
Full Blood Group
Antibody Screen
Antibody Identification
Cross Matching
Issuing of blood products and components
Kleihauer testing
Anti D issue
Investigation of suspected transfusion reaction
There is close links with the regional NHS blood and transplant service based in
Sheffield. Specialist work is referred to this centre.
Blood Grouping and Antibody Screen
Safe determination of a patient’s blood group and exclusion of clinically
significant antibodies takes a minimum of two hours. If an antibody is present
identification may significantly increase the time required by the laboratory for
safe blood provision. It is best to determine a patients blood group well in
advance of the time when blood may be required, as ‘emergency groups’ carry a
greater risk of error.
Surgical Waiting List Cases
An outpatient whose name is put onto the waiting list for operation should have
the blood group determined before admission to hospital. This reduces the risk
that blood may not be available at the time of operation if antibodies are
subsequently detected in the plasma. Please note it may take up to 48 hours to
provide compatible blood for patients with clinically significant antibodies.
PLEASE CONTACT BLOOD BANK AS SOON AS BLOOD REQUIREMENTS
ARE KNOWN.
Page 46 of 62
Blood Cross-Matching
To arrange for blood to be prepared for a transfusion, a Nottingham University
Hospitals Blood Transfusion request form must be completed and sent with a
6mL EDTA sample (pink top).
Samples
Samples for blood grouping and/or cross matching may be taken by
phlebotomists, medical staff or authorised nursing staff. The bottle label must be
handwritten and must indicate:
1.
2.
3.
4.
5.
Full name of patient.
Hospital number
Date of birth.
Time and date sample taken.
Sample must be signed by person taking the sample
Identity must be confirmed by direct questioning and by checking the identity
band when worn. Pre-printed adhesive identity labels must not be attached to
samples for blood transfusion because this negates proper identity checks on the
ward.
Request Form
It is essential that the request form is carefully completed, adhesive identity
labels may be used as long as this does not obscure any relevant information. It
is vital to supply details of the number of units of blood/products to be prepared
and the date and time that they are required.
Before making any request it is essential that the patient’s notes are checked for
possible previous transfusion problems and/or special requirements eg: CMV
negative, Irradiated and/or antigen and all relevant information included on the
request.
For
Haematology
patients
refer
to
the
guideline:
http://qwss01/sites/NUH/Guidelines/1074.doc
Collection
Only staff who have been trained in the collection of blood products in the last 2
years may collect blood components.
Blood transfusion should commence within 30 minutes of blood being removed
from the blood bank issue fridge and each unit of red cells must be transfused
within 4 hours of collection. If the transfusion is not started within this time but
transfusion is planned for the patient, and the unit can be transfused within 4
hours it is fine to use. If the transfusion cannot be completed within 4 hours and
the unit of blood has been out of the fridge for longer than 30 minutes, return the
unit to the blood bank laboratory and hand it to a member of the laboratory staff.
Never put blood back in the Issue Fridge if it has been out of temperature
control for more than 30 minutes. Blood returned from a satellite fridge can be
returned to the main issue blood fridge.
Page 47 of 62
Blood MUST NEVER be placed in a domestic refrigerator on the ward. Boxes
and cool packs are available from blood bank for transportation of blood. They
are not designed for the storage of blood and MUST NOT be used for this
purpose on the wards.
Prescription
All prescriptions for blood products must be made by a doctor. Blood
components must be prescribed on a blood transfusion prescription and record
sheet. After transfusion this document must be filed in the patients case notes
and the top copy returned to blood bank.
Emergency Transfusion
Personal contact between the doctor concerned and the Transfusion Laboratory
is essential in cases of emergency. 0 negative or group specific red cells can be
issued in dire emergency, but should be avoided if time allows for a full
crossmatch. Please see the guideline for massive haemorrhage in the
transfusion policy.
Reservation of Unused Blood
Cross-matched blood will be withdrawn 24 hours after the stated time of
operation and/or transfusion. After this time it will be available to be prepared for
other patients, and the onus is on the clinician to notify the Transfusion
Laboratory if it is considered that the blood will be required after the initial 24
hour reservation period has elapsed. This is particularly relevant where a
proposed operation is cancelled or postponed. Do not assume that the blood will
still be available. A further cross match sample and request may be necessary if
blood is again required after it has been withdrawn.
If you wish to check whether a patient has been cross-matched, then this
information is available on NOTIS.
Blood Components
The following products are available from blood bank
Red Cells
Fresh Frozen Plasma (FFP)
Cryoprecipitate
Platelets
Albumin (4.5% and 20%)
Coagulation Factor Concentrates (including Factor VIIa)
The storage, availability and administration of blood components differ between
products. Advice on the availability of products and pre-transfusion testing can
be given by laboratory staff. All requests for advice on the appropriateness of
transfusion and indications for blood component therapy should be directed to
the Haematology medical staff. This should be the registrar on duty for
Haematology in the first instance. The laboratory staff will challenge any requests
Page 48 of 62
they feel may be inappropriate and will request authority to issue blood products
from a member of the Haematology medical staff if they feel this is required.
Recombinant Factor VIIa (novoseven)
A trust guideline for the use of recombinant factor VIIa is available. The duty
Haematology registrar should be contacted for advice prior to requesting this
product.
http://intranet/Divisions/Medicine/Anticoagulation/Protocols/rVIIa%20protocol.pdf
Prothombin Complex Concentrates (Octaplex)
Indicated for emergency reversal of Warfarin. Requests should be discussed
with the Haematology registrar on call. Protocol for use is available at:
http://intranet/Divisions/Medicine/Anticoagulation/Protocols/Octaplex%20guidline
s.pdf
PREVENTION OF RHESUS HAEMOLYTIC DISEASE OF THE NEW-BORN
Anti-D immunoglobin is administered to non-sensitised Rh negative women
following a potential sensitizing event or as part of the routine antenatal anti
D prophylaxis (RAADP) programme. A trust guideline is available at:
http://qwss01/sites/NUH/Guidelines/1015.doc
Anti-D should be given within 72 hours of the sensitizing event at the very latest.
If this time has elapsed, contact the transfusion laboratory for advice regarding
administration.
OBSTETRIC PATIENTS
The samples listed below should be taken 30 minutes post delivery and should
be sent to the Blood Transfusion Laboratory as soon as possible for a decision
on the need for Anti-D administration to be made.
GYNAECOLOGICAL PATIENTS
The samples required are listed below and should reach the Blood Transfusion
Laboratory as soon as possible. Where the procedure is a planned termination
of pregnancy before 20 weeks gestation, the sample should be taken at the
Outpatient Clinic in advance of the admission.
Delivery or Abortion After 20 Weeks
Manoeuvres After 20 Weeks
(e.g. external cephalic version amniocentesis)
Manoeuvres Before 20 Weeks
(e.g. amniocentesis, abortion before 20 weeks)
Samples
Required
for
Obstetrics
and
Gynaecology
6ml + 3.0ml maternal EDTA samples, and 6mL EDTA
sample of cord or 2mL EDTA neonatal blood.
A completed Kleihauer card.
6ml + 3.0ml maternal EDTA sample.
A completed Kleihauer request form.
6mL EDTA maternal blood.
A completed Kleihauer request form.
ROUTINE ANTENATAL ANTI-D PROPHYLAXIS PROGRAMME (RAADP)
Page 49 of 62
The current recommendation is 1500IU Anti-D to be administered at 28 weks
gestation for non sensitized Rh D negative women. The injections given as
RAADP are in addition to any other anti-D given due to potential sensitizing
events. This service is provided by Blood Bank at both the QMC and City
Campus through the Community Midwives.
Samples
BLOOD TRANSFUSION
Group and Screen
Group, Screen
Cross Match
Coombs Test
and
Infant Group
(< 4 months of age)
Kleihauer
Rh anti-D Prophylaxis
Cold Agglutinin Screen
Cold Antibody Titre
(cardiac patients only)
HLA/platelet
antibody
testing
6ml EDTA
6ml EDTA
6ml EDTA
1ml EDTA 6ml maternal sample on first occasion if blood is required
6 ml + 3ml maternal EDTA + Cord Sample or Neonatal Blood for deliveries
6 ml +3ml maternal EDTA for non deliveries >20weeks
6 ml maternal EDTA for non deliveries <20weeks
Completed Kleihauer Form Required
6 mL EDTA
6mL EDTA
2 x 6mL EDTA
1 x 6mL Clotted
Page 50 of 62
CLINICAL PATHOLOGY DEPARTMENT
DEPARTMENTAL MANAGEMENT
Clinical Lead
Professor Noor Kalsheker MB, ChB, MSc, MD
Ext 78330720 noor.kalsheker@nuh.nhs.uk
Clinical Pathology Service Manager
Mrs. Karen Jones MSc, CSci, FIBMS, MinstLM
Ext 64929
Pathology Quality Manager
Ms Liz Bakowski
FIBMS
karen.jones@nuh.nhs.uk
Ext 57187 City
or 62538 QMC
liz.bakowski@nuh.nhs.uk
Ext
63087
Direct Line
0115 9709168
0115 9709167
IMMUNOLOGY SECTION
ENQUIRIES
Results
Fax
All specific enquiries regarding diagnosis and management of immune disorders
should be made to the Immunology medical staff
Most results are available (Monday-Friday) within 24-72 hours of the receipt of
the specimen. Some tests are batched and may take longer because of the
interval between batches. An Immunology medic can be contacted by
switchboard on Saturday mornings for advice 9.00am - 12.30pm. Urgent antiMPO / PR3 requests are available on Saturdays 9.00 – 11.00am following
discussion with the medic.
SENIOR STAFF
Ext
Consultant Immunologists
Dr Liz McDermott MB BS FRCP DM FRCPath
Dr Liz Drewe MBBS, PhD, FRCPath, MRCP
Prof H Sewell PhD, FRCP, FRCPath, FMedSci
67064
66032
78330003
Associate Specialist
Dr Anwar MBBS, PhD
64164
Specialist Registrars
65083
Operational Services Manager
Mr Simon Martin BA (Hons), FIBMS, CSci
61654
Page 51 of 62
GENERAL INFORMATION
The Immunology Section of Clinical Pathology is located on the Queen’s Medical
Campus and provides a number of specialised services.
This section is staffed from 9.00am to 5.30pm Monday to Friday.
Routine immunochemistry (immunoglobulins, myeloma screening and typing,
complement levels and other specific protein assays) are performed by Clinical
Pathology on the City Campus.
Immunological investigations are particularly relevant in the diagnosis and follow
up of patients with the following:1.
2.
3.
4.
Connective Tissue and other Autoimmune Diseases.
Immunodeficiency.
Allergy and Anaphylactic reactions.
Lymphoproliferative Disorders.
Discussion of clinical cases with the Immunology medical staff is encouraged in
order to select the most appropriate tests.
Test interpretations are provided where appropriate, and medical staff are
pleased to answer enquiries about interpretation or further tests.
URGENT REQUESTS
Samples for Anti-GBM will always be processed as URGENT; for any other tests
that are required urgently please notify the laboratory by telephone (Ext 64956)
before sending the sample. Whenever possible urgent requests will be
processed the same day.
If the patient is known to be, or suspected of being, HIV, Hepatitis B or C
positive, or falls into a high risk category please use a BIOHAZARD bag for the
transportation of the sample to the laboratory. DO NOT USE THE PNEUMATIC
TUBE FOR HIGH RISK SAMPLES.
ADVERSE DRUG REACTIONS/ANAPHLYAXIS
Anaphylaxis is a severe, life-threatening, reaction caused by hypersensitivity to
certain allergens. These are commonly food, drugs or venom.
Full details regarding diagnosis and management of anaphylaxis can be found
at: http://www.resus.org.uk/pages/reaction.pdf
In anaphylaxis, mast cells release tryptase and levels in the blood can be used in
the follow-up of suspected anaphylaxis. Levels increase after about 30 minutes
and peak at 1-2 hours before returning to baseline levels after around 8 hours.
During a reaction, ideally, 3 serum samples (clotted sample) or plasma (EDTA
sample) should be taken to measure blood tryptase:
Page 52 of 62
1) Immediately after the onset of the reaction (but do not delay treatment)
2) 1-2 hours after the onset of the reaction
3) 24 hours after the onset of the reaction
To assist interpretation, please label each sample with the time after the start of
the reaction.
All patients having suffered an anaphylactic reaction should be referred after the
event for outpatient assessment to Dr Liz Drewe or Dr. Kumar in the Clinical
Immunology and Allergy Unit.
Investigation
Turnaround Time
Result, Reference Range and
Extra Information
Our aim is to report 85% of tests within the following time frames.
Unless otherwise stated all analyses require 5mL of clotted blood.
Autoimmune liver screen
7 days
Reported as negative or positive
Screen includes:
Anti smooth muscle antibodies
Anti-gastric parietal cell
antibodies
Anti-mitochondrial antibodies
Anti-LKM antibodies
But NOT Rheumatoid factors or
anti-nuclear antibodies
Individual Autoantibodies
(Report as negative or positive unless otherwise stated)
Anti-Acetylcholine Receptor Abs
Anti-Adrenal Abs
Anti voltage gated calcium
channel antibodies
Anti-Cardiac Muscle Abs
Anti-Cardiolipin Abs
Anti-Beta-2-Glycoprotein Abs
Anti-Centromere Abs
Anti-DNA Abs
Anti-ENA Abs
Anti-Ganglioside Abs
Anti-glomerular basement
membrane antibodies
Anti-Intrinsic Factor Abs
Anti-Islet Cell Abs (Anti-ICA)
Anti-neuronal (cerebellar) Abs
21 days
7 days
21 days
Anti-nuclear Abs (ANA)
3 days
Anti-neutrophil cytoplasmic Abs
(ANCA)
3 days
Anti-Skeletal Muscle Abs
Anti-TPO
C3 Nephritic Factor
7 days
Rheumatoid Factor
Skin-Reactive Abs
7 days
7 days
7 days
3 days
7 days
7 days
21 days
24 hours
Numerical results
Numerical results
Numerical results
Numerical results for positive
samples
7 days
7 days
7 days
Anti Hu, Yo , Ri , Ampiphysin
reported
Titre and pattern also reported.
Anti-DNA and ENA performed
depending on results.
Anti-MPO and PR3 Abs
performed on new positive
samples, and for monitoring
See page 20
Recommend request C3 and C4
as well. Test only done if C3 is
low
See page 27
Pemphigus/Pemphigoid pattern
reported
21 days
7 days
Page 53 of 62
Immunochemistry
Complement Studies
C3, C4
C1 inhibitor
21 days
C3d
21 days
C1q
CH50/AP50
21 days
7 days
See page 22
10 mL Clotted. Recommend
request C3 & C4 as well
Discuss with Immunology staff
before requesting. EDTA plasma
must be received in the
laboratory on the same day.
Sample should reach laboratory
within 2 hours, otherwise sera
should be separated and frozen
Immunoglobulin Measurements (including Myeloma Screen)
Immunoglobulins (IgG, IgA &
IgM)
Serum Protein Electrophoresis
Immunofixation
Paraprotein Quantitation
(Densitometry)
Urine Bence Jones Protein
IgE – Total
IgE - Allergen Specific (RAST)
7 days
7 days
Oligoclonal bands
Isotransferrin (beta-transferrin)
Cryoglobulin Studies
7 days
24 hours
10 days
See page 24
See page 27
See page 24
See page 26
See page 20
Total 10mL Clotted.
10mL Clotted. Clinical details
essential for selection of
appropriate RAST tests.
Paired serum and CSF required
20 mL, clotted at 37oC – contact
Clinical Pathology Reception to
arrange collection prior to
venepuncture
FUNCTIONAL (SPECIFIC MICROBIAL) ANTIBODIES
Anti-tetanus, H. influenzae type b and Strep. Pneumoniae. Pneumococcal
antibodies are routinely tested for those antigens found in Pneumovax. Please
specify if Prevenar has been used. Dates of recent vaccinations should be
documented on the request card to enable appropriate interpretation
IMMUNOFLUORESCENCE INVESTIGATION OF BIOPSY TISSUE
Biopsy tissue must be fresh, unfixed and transported in liquid nitrogen.
CELLULAR INVESTIGATIONS
Lymphocyte markers (eg. CD4 monitoring) are available routinely. Requests for
any other panels, or requests for NBT, ADA or lymphocyte stimulation studies
should only be undertaken after discussion with the laboratory.
Immunophenotyping for malignant disease see page 38.
Page 54 of 62
MOLECULAR DIAGNOSTICS SECTION (QMC Campus)
GENERAL INFORMATION
The Molecular Diagnostics section is based at QMC Campus. It provides genetic
testing for thrombophilia risk factors (Factor V Leiden and prothrombin
g.20210G>A’ variants), alpha-1-antitrypsin deficiency and haemochromatosis.
The section is closely associated with the Haemophilia Comprehensive Care
Centre and provides genetic testing for inherited bleeding disorders, including
haemophilia A and B, fibrinogen disorders and a range of coagulation factor
deficiencies.
Operational Service Manager
Ext
66593
Dr Marian Hill BSc (Hons), Ph.D
ENQUIRIES
Please contact the laboratory for further information and test costs.
Ext
Direct Line
66593
0115 8754593
SAMPLE REQUIREMENTS
2x 5mL EDTA blood is required for most investigations. Buccal swabs may also
be used with prior arrangement.
For genetic analysis of bleeding disorders; requests must be made through a
Consultant Haematologist. The laboratory must be informed of any limitations to
consent. Genetic request forms are available – please contact the laboratory’
TURNAROUND TIME
For detection of a known mutation (eg. alpha-1-antitrypsin and
haemochromatosis genotyping, thrombophilia genetic risk factors or analysis of a
previously determined familial mutation) there is a 2 week turnaround time. We
aim to meet this target in 85% of cases.
For investigative testing (where target mutation has not been previously
determined) turnaround time for initial report is 6-8 weeks. We aim to meet this
target in 85% of cases.
Page 55 of 62
POINT-OF-CARE TESTING (POCT) DEVICES
Equipment to measure various analytes including blood glucose, blood-gases,
co-oximetry, bilirubin and haemoglobin are available in selected clinical areas.
All members of staff using POCT devices must be familiar with the Trust Policy
for the Management of Point of Care Testing Devices and the Trust Procedure
for the Implementation and Management of Point of Care Testing Devices. The
Trust Policy For Training In The Safe Use of Medical Devices also governs the
use of POCT equipment.
POCT equipment must only be used by trained staff with documented
competency and once appropriate results have been gained from quality
control (QC) testing. Results must be documented in the patient’s notes.
For any general queries regarding POCT devices (other than breakdown or
training requests) contact Ann Marie Carrol (ann marie.carroll@nuh.nhs.uk).
BLOOD GAS ANALYSIS
At City campus blood-gas analysers are sited within:
Neonatal Unit, Labour Suite, ICU, HDU, Cardiac Theatres, CICU, Southwell ward
(South corridor) and the Lung Function Laboratory (North Corridor).
At QMC campus blood-gas analysers are sited within:
Neonatal Unit, Labour Suite, AICU, PICU, ED, SHDU, AMU and CCU.
If a blood-gas analyser is not present on your ward at City campus you can
use the instrument located in the Lung Function Laboratory (North Corridor
areas) or on Southwell ward (South corridor areas). At QMC campus use
the analyser located nearest to you.
Lung Function Laboratory Service (City Campus)
During routine working hours (Monday-Friday 9.00-16.30) the Lung Function
Laboratory (Ext. 56191) will analyse samples brought from any location (by prior
arrangement, a Blood-gas card must be fully completed).
Where staffing levels allow the Lung Function Department offers a limited
capillary-gas service to wards at City campus. Telephone Ext 56191 for further
details.
Outside routine hours the Lung Function Laboratory can be accessed by using
the digital lock code (obtained in person from Switchboard). Follow the
instructions given above the analyser very carefully.
Specimen
Capillary or arterial blood collected into a labelled heparinised blood-gas syringe.
Immediately following collection expel all air bubbles from the syringe, cap tightly
and mix by rolling and gentle inversion. Samples must be analysed within 10
minutes of collection.
Breakdowns
If you have any problems with the blood gas analysers on the City Campus
(other than those present in the Lung function laboratory or Southwell ward)
Page 56 of 62
please contact the Clinical Pathology Department on Ext 54436. At QMC
Campus contact MESU on Ext 63559.
Training
Only trained staff may use a blood-gas analyser. Training can be obtained at City
campus by contacting Katie Evans (Ext 54436). At QMC campus contact MESU
on Ext 63559.
BLOOD GLUCOSE ANALYSIS
Most clinical areas have Medisense Optium Xceed glucose meters. Training is
available through the link nurse on the ward, or the diabetic nursing staff. Any
results that are grossly abnormal or unexpectedly high should be checked
immediately by the Clinical Pathology Department. ALL glucose results less than
2.5 or greater than 25.0 mmol/L MUST be checked by sending a venous sample
to the laboratory immediately.
Blood glucose meters MUST NOT be used during peripheral shutdown, such as
in DKA or hypovolaemia. In these cases a venous sample must be sent to the
Clinical Pathology laboratory.
Sample
Finger prick capillary blood sample that must be analysed immediately.
Breakdowns
If you have a problem, or suspect a problem, with a blood glucose meter stop
using it immediately and take it to MESU (QMC campus) or the Equipment
Library (City campus) to be replaced.
Training
Only trained staff may use a blood glucose meter. Training can be obtained at
City campus by contacting Janice Brown in Dundee House (Ext 56811). At QMC
campus contact Janet Evans on Ext 65813.
PAEDIATRIC BILIRUBIN ANALYSIS
A Bilirubinometer is sited in the Neonatal Unit at City campus. Training is
available through the Clinical Pathology Department. This machine is suitable
for paediatric samples only. Any results that are grossly abnormal, unexpectedly
high or above 350 µmol/L should be checked by sending a sample to Clinical
Pathology Department immediately.
Sample
Capillary blood collected into a Red Capped Chance-Propper capillary.
The sample must be protected from light until analysis.
Breakdowns
If you have a problem, or suspect a problem, with a Bilirubinometer stop using it
immediately and call MESU.
Page 57 of 62
HAEMOGLOBIN
HemoCue devices for haemoglobin analysis are present in several locations
across the Trust. Ensure that the instrument displays the result with the correct
units (g/dL). Results should always be interpreted in the light of the patient’s
condition. Any unexpected, very high or low results MUST be confirmed by
sending an EDTA specimen to Clinical Pathology for confirmation before action
is taken.
A HemoCue result should never be used as a basis for a transfusion request.
Sample
Finger prick capillary blood sample that must be analysed immediately. Do NOT
use samples from other areas (such as the earlobe) as this often gives incorrect
results.
Breakdowns
If you have a problem, or suspect a problem, with a HemoCue stop using it
immediately and call HemoCue (01246 292955)
Training
Only trained staff may use a HemoCue. Training can be obtained by contacting
the designated trainer for that area or by contacting Katie Evans (Ext 54436).
Page 58 of 62
VACUTAINER TUBE GUIDE
Please see our website for the most up to date Tube Guide.
Nottingham University Hospitals NHS Trust
COLOUR AND TYPE OF TUBE USED
LithHep
SST
Gel
EDTA
4mL
EDTA
7mL
Fluorideoxalate
17-alpha OHP
3-Hydroxybutyrate
ACE
ACTH
Adult Blood Group
AFP
Albumin
Alcohol
Aldosterone
Alk Phos (ALP)
SECTION
Clotted
Clinical Chemistry
Clinical Chemistry
Clinical Chemistry
Clinical Chemistry
Transfusion
Clinical Chemistry
Clinical Chemistry
Clinical Chemistry
Clinical Chemistry
Clinical Chemistry
Clinical Chemistry
Clinical Chemistry
Clinical Chemistry
Alk Phos Isoenzymes
ALT
Ammonia
Citrate
<30
Min
Amylase
ANCA
Androstenedione
Antenatal Group and
Antibody Screen
Antibody Screen
AST
Antithrombin III level
Anti Xa Assay
Clinical Chemistry
Immunology
Clinical Chemistry
Blood Transfusion
Blood Transfusion
Clinical Chemistry
Haematology
Haematology
Haematology
Haematology
Immunology
APC Resistance Ratio
APTT
Autoantibody Screen
- ANA
- AI Liver Screen
Autoantibodies
Eg;Adrenal, Islet
Cell,Salivary gland
Immunology
B12/Folate
Beta-2 microglobulin
Bicarbonate
Bile Acids
Bilirubin (D&I)
Bilirubin (Total)
Biotinidase
Clinical Chemistry
Clinical Chemistry
Clinical Chemistry
Clinical Chemistry
Clinical Chemistry
Clinical Chemistry
Clinical Chemistry
<30
Min
Blood Film Exam
Bone Profile
C3/C4
CA125
CA153
Caffeine
Calcium
Carbamazepine
CEA
Chloride
Cholesterol
Cholesterol HDL
Haematology
Clinical Chemistry
Clinical Chemistry
Clinical Chemistry
Clinical Chemistry
Clinical Chemistry
Clinical Chemistry
Clinical Chemistry
Clinical Chemistry
Clinical Chemistry
Clinical Chemistry
Clinical Chemistry
Page 59 of 62
Cholinesterase
CK
Clinical Chemistry
Clinical Chemistry
Haematology
Clotting Screen
(Prothombin Time,
APTT)
Coeliac screen
Cold agglutinin screen
Complement
Copper
Cortisol
Cross Match
C-Peptide
Creatinine
Crosslaps (CTx)
CRP
Cryoglobulins
Cyclosporin
Blood Transfusion
Clinical Chemistry
Clinical Chemistry
Clinical Chemistry
Blood Transfusion
Clinical Chemistry
Clinical Chemistry
Clinical Chemistry
Clinical Chemistry
Contact laboratory
Clinical Chemistry
Haematology
Clinical Chemistry
Clinical Chemistry
Blood Transfusion
Clinical Chemistry
Immunology
Clinical Chemistry
Immunology
Haematology
Clinical Chemistry
Haematology
Clinical Chemistry
Clinical Chemistry
Clinical Chemistry
Clinical Chemistry
Clinical Chemistry
Haematology
Haematology
Clinical Chemistry
Clinical Chemistry
Clinical Chemistry
Haematology
Immunology
D-Dimer Level
DHEAS
Digoxin
Direct Coombs (DCT)
Down Screen
DsDNA antibodies
Electrolytes
ENA
ESR
Ferritin
Fibrinogen Level
FK506 (tacrolimus)
Free Fatty Acids
Free T3
Free T4
FSH
FV Leiden
G6PD Screen
GALPut Screens
Gamma GT
Gastrin
Glandular Fever Screen
Glomerular Basement
Membrane Antibody
(GBM)
Glucose
Group & Save
Haemoglobinopathy
Screen
Haemoglobin S
Quantitation
Haemolysin (ABO
HDNB)Screen
Haptoglobin
HbA1c
HCG
Clinical Chemistry
Blood Transfusion
Haematology
Haematology
Blood Transfusion
Haematology
Clinical Chemistry
Clinical Chemistry
Blood Transfusion
Clinical Chemistry
HLA Antibody screen
Homocysteine
<30
Min
IBC
IgA
IGF-1
IgG
Clinical Chemistry
Clinical Chemistry
Clinical Chemistry
Clinical Chemistry
Page 60 of 62
IgM
Immunofixation
Immunoglobulins
Insulin
Iron
Lactate
LDH
LDH Isoenzymes
LH
Clinical Chemistry
Clinical Chemistry
Clinical Chemistry
Clinical Chemistry
Clinical Chemistry
Clinical Chemistry
Clinical Chemistry
Clinical Chemistry
Clinical Chemistry
Clinical Chemistry
Lipoprotein
Electrophoresis
Lithium
Liver Function Tests
Clinical Chemistry
Clinical Chemistry
Haematology
Clinical Chemistry
Haematology
Lupus Inhibitor Screen
Magnesium
Malarial Parasite
Screen
Methanol
Methotrexate
Neonatal
Thrombocytopenia
Clinical Chemistry
Clinical Chemistry
Blood Transfusion
Blood Transfusion
Blood Transfusion
Clinical Chemistry
Clinical Chemistry
Clinical Chemistry
Clinical Chemistry
Clinical Chemistry
Clinical Chemistry
Clinical Chemistry
Clinical Chemistry
Clinical Chemistry
Haematology
Blood Transfusion
Clinical Chemistry
Clinical Chemistry
Clinical Chemistry
Clinical Chemistry
Clinical Chemistry
Haematology
Haematology
Haematology
Pregnancy Test (Blood)
Oestradiol
Osmolality
P1NP
Paracetamol
Phenyalanine
Phenytoin
Phosphate
Plasma Amino Acids
Plasma Viscosity
Plasma Antibody
Potassium
Progesterone
Prolactin
Protein Electrophoresis
Protein (Total)
Protein C Level
Protein S Level
Prothombin Gene
20210A
Prothombin Time
PSA
PTH
Renal Profile
Renin
Reticulocyte Count
RF
Salicylate
SHBG
Sickle Screen
Skin Autoantibodies
Sodium
Haematology
Clinical Chemistry
Clinical Chemistry
Clinical Chemistry
Clinical Chemistry
Haematology
Immunology
Clinical Chemistry
Clinical Chemistry
Haematology
Immunology
Clinical Chemistry
Clinical Chemistry
Suxamethonium
Sensitivity
Tacrolimus
Testosterone
Theophylline
Clinical Chemistry
Clinical Chemistry
Clinical Chemistry
Page 61 of 62
Thyroid Function Tests
Thyroid Antibodies
Tissue Typing
Transferrin
Transfusion reaction
Triglyceride
Troponin I
TSH
Tyrosine
U&E’s
Urate
Urea
Clinical Chemistry
Immunology
Blood Transfusion
Clinical Chemistry
CONTACT BLOOD TRANSFUSION IMMEDIATELY
Clinical Chemistry
Clinical Chemistry
Clinical Chemistry
Clinical Chemistry
Clinical Chemistry
Clinical Chemistry
Clinical Chemistry
Clinical Chemistry
Clinical Chemistry
Clinical Chemistry
Clinical Chemistry
Clinical Chemistry
Clinical Chemistry
Valproate
Vitamin A
Vitamin E
White Cell Cystine
White Cell Enzyme
Whole Blood
Potassium
Zinc
Clinical Chemistry
Page 62 of 62