Using Qualitative Research Methods in Nursing
advertisement

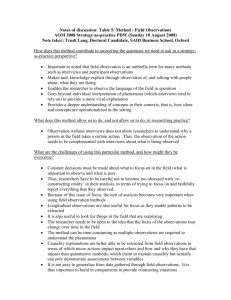
Marrow C (1996) Using qualititative research methods in nursing. Nursing Standard. 11, 7, 43-45. Using qualitative research methods in nursing This paper explores the problems and dilemmas encountered while conducting a longitudinal qualitative research study in the clinical nursing environment and highlights strategies that helped to overcome the difficulties of using observations and interview techniques. The author concludes that research within practice is essential to ensure successful implementation. Date of acceptance: May 17 1996. Carol Marrow BA(Hons), MPhil, Cert Ed, RGN, RMN, is Senior Lecturer, University College of St Martins Education Centre, Furness General Hospital, Barrow-in-Furness. KEY WORDS: NURSING RESEARCH QUALITATIVE RESEARCH METHODS NURSING PRACTICE Novice researchers are often unsure of the most appropriate methods to use in their research. However, critical evaluation of data collection methods used in other studies can help to develop some understanding of the methodological issues. It is important not to diminish the problems encountered when conducting a study. However, the benefits of qualitative methods in the clinical field should not be ignored as it is valuable to develop theories that recognise clinical constraints. This is essential to the profession of nursing with its emphasis on humanism and caring for the whole person. Indeed, Duffy (1985) suggested: 'Researchers of the phenomenological schools, for example grounded theorists, reject the assumptions of positivism, and attempt to humanise the research process.' Research methodologies which enable the participants to interpret their behaviour in a meaningful way are essential to the qualitative approach. This study explored supervision issues and involved observing and interviewing a cohort of Project 2000 students and their clinical supervisors (n=30). Data was collected using direct observations and semi-structured interviews and analysed by the use of a continuous, comparative method (Glaser and Strauss 1967). OBSERVATION One of the main reasons for choosing observation as a method of data collection in this study was to allow what actually occurred to be seen and recorded, rather than solely relying on the participants' perceptions of what had taken place. Observation techniques as a method of choice, however, are not without their problems and researchers should be aware of the issues to try to avoid any complications. In the clinical field, the best positions for observation should be identified as well as a suitable area for writing field notes, otherwise valuable time can be wasted when the investigation commences. In this study, it proved difficult to find a suitable place to write the field notes as many of the wards where observation took place did not have a quiet room, apart from in the mental health settings. The staff canteen had to be used on occasion, which was not ideal as it was usually noisy. Leininger (1985) highlighted other potential difficulties and stated that the observer must overcome at least two major hurdles concerning his or her relationship with the participants studied. The first of these is to gain entry. In this study, the students had been approached and the research explained before entering the ward. However, it was also important to make myself known immediately on entering the ward and to explain again to both the students and qualified staff (supervisors) why I was there. I was never once refused entry and was always made welcome, therefore it seemed the participants did not feel threatened by my presence. This was not always apparent in practice as some of the supervisors repeatedly asked: 'What are you looking for?' The second hurdle Leininger (1985) postulated was to establish rapport and develop trust within the social group. The wards were generally very busy on the occasions when the observations took place and it was clear that the participants often became so immersed in their work that they forgot my presence. This was supported by evidence from the subsequent interviews. When asked how it felt being observed practising, one student stated: 'It felt very uncomfortable at first; I felt I was being scrutinised but I was surprised how soon I forgot you were there and when you later came to seek me out for interview, I thought you had already gone...knowing you were a nurse helped, it made me think that you would understand.' Even when I tried to keep the participants informed, there were occasions, particularly in the early stages of the study, when I felt that they (mainly the qualified nurses) appeared suspicious of my real motives. This warranted careful handling of the staff through active communication on all aspects of the research. This continuous form of interaction, although important for information giving, might have caused many problems, not least developing too deep an involvement in the ward culture on my part. This was one of the reasons for being a non-participant observer. NON-PARTICIPANT OBSERVATION Participant observation was rejected in this study principally because the researcher often does not reveal his or her identity to the group being studied. This may place conflicting demands on the part of the researcher. Gold (1958) saw these conflicts as feelings of guilt concerning the way information has been obtained and the consequent need to reveal one's true identity. This in turn may prevent the researcher from performing convincingly in the role. Another difficulty is the ability to observe objectively, as the researcher may become so immersed in the participants' world that there is the danger of 'going native'. In this particular study, it may also have been difficult to obtain permission from hospital managers if my identity had had to be concealed. Non-participant observation also allows the researcher to take time out to write field notes and reflect on what has been observed and the issues raised. These included the actual behaviour of the participants, the theoretical application and the methodological problems. Bannister (1981) suggested that thinking time within a research project is vitally important; for example, problems with the observation framework can be addressed by acknowledging apparent weaknesses and, furthermore, theories can be thought through and applied to the observational notes. It is also important to take regular time out to combat lapses in concentration caused by fatigue or boredom; occasionally I considered leaving the research area earlier than scheduled and had to remind myself that this might mean missing relevant data. It proved difficult not to become involved with nursing care interventions; doing so may have interrupted the flow or the focus of thinking with respect to the research issues. Moreover, observing practice that appeared questionable by my own personal standards caused significant role conflict; I was forced at times to consider which role was more important, nurse or researcher? Many researchers believe that remaining outside the research scene is essential, so that the natural situation will not be changed by the researcher's presence. The researcher must analyse the complete situation objectively otherwise there is a danger of credibility being lost and further access being refused (Sapsford and Abbott 1992). Bogdan and Taylor (1975), however, suggested that some researchers believe that passive observation condones such behaviour. One helpful way of overcoming the problem of not participating was to interview the participants immediately after observations had occurred. After observing on the wards the field notes were carefully evaluated and, as stated earlier, issues that needed clarification were identified and noted. Sometimes these issues did have ethical implications and it was useful to be able to explore them further in a safe and trusting environment. Becker and Geer (1970) suggested that observers can interview their subjects at the end of the field work. They should then have the trust of the study participants and sufficient relevant information to make their questions 'poignant and relevant to the interests of subjects' (Bogdan and Taylor 1975). SEMI-STRUCTURED INTERVIEWS As suggested, another data collection method used in this study was semi-structured interviews based on an open questioning technique called 'the funnel' (Cohen and Manion 1989). This technique generally commences with a broad statement or question after which the focus progresses to more specific issues. The interviews, comprising five open-ended questions, were audio-taped to allow the feelings of the participants (students and supervisors) to come across and to ensure that no important issues were omitted. The interviews were taped with the participants' consent. Tape recordings are felt to be useful for capturing each participant's mood or strength of feeling on issues raised. However, when relying completely on tape recordings, non-verbal behaviour is often ignored. Breakwell (1990) maintained that it is useful to note points where non-verbal communication was strong; this can help to clarify whether what respondents are saying actually correlates with what they are feeling. For example, breaking eye contact when discussing an issue may indicate that the individual feels uncomfortable with that particular issue and does not wish to discuss it further. In this study, the interviews were taped with one exception (a student who was uncomfortable with the tape recorder) and key issues were noted. As already stressed, this was to prove useful when it came to transcribing the data, as the notes emphasised the substantial points and reinforced the feelings of the participants. Each tape recording was transcribed in full. The supervisors were also interviewed in the same conversational style. I had thought that the interviews with the qualified nurses would be easier and in greater depth because I presumed they would be more comfortable and knowledgeable when discussing their supervisory role and the students' learning. It was, therefore, surprising when the students proved generally more vocal than the qualified staff. It could be that the students welcomed the opportunity to vent their feelings on their clinical learning experience, whereas the pressure of work could have induced guilt feelings in the qualified staff for leaving the patients. However, to have interviewed them at a separate time and location would have been difficult organisationally, and the issues that arose from the observations would not have been as compelling if referred to out of context. Many issues observed were clarified at interview. This was crucial as many constraints on practice were identified; for example, lack of time, poor staffing levels and inadequate skill-mix resulting in poor student supervision. In addition, on many occasions a task-centred approach to care interventions was used. The interviews were conducted in a relaxed conversational style. The rapport that developed was important in helping to elicit more in-depth information by encouraging the students to feel both safe and confident. Massarik (1981) suggested various types of interview; these ranged from the hostile interview to the humanist phenomenal interview where there is mutual respect and sharing. The latter is characteristic of the interviews used in this study. The students were encouraged to feel relaxed and this was enhanced by asking them to discuss their clinical learning experiences generally before focusing on specific areas. A technique devised by Leininger (1985) was used. She described how the statements 'tell me' and 'I would like to hear about' tend to open the 'idea gate', and further explained that: 'These stems permit the informant to tell the story in his or her own way and style...the informant supplies the information more easily and makes it unnecessary for the researcher to ask literally hundreds of questions and often get less information.' In this relaxed style topics that arise can be explored, provided that the interview focus is adhered to and that any misunderstandings are resolved to avoid pursuing irrelevant information. The skills of the interviewer are also important in encouraging the participants to talk freely and comfortably. Although relatively inexperienced at research interviewing, some experience in mental health nursing and counselling helped me to adopt a facilitative rather than a controlling stance. This counselling approach can also be problematic, however, as the students often saw this as a chance to complain about the Project 2000 course. This was difficult to handle at first as I felt that these issues needed to be discussed otherwise the interview would not progress. The problem was eventually resolved by suggesting that the issues be discussed at the end of the interview if time was available or, alternatively, I could see the students again. This latter offer was never taken up and I feel that the students raised many grievances which remained unresolved. Interruptions were also a problem. Many of the interviews were conducted in the ward clinic as there was no other private area available. This sometimes interrupted the conversational flow and it often took some time to re-establish the discussion focus. Many of the interruptions were made by busy nursing staff requiring equipment. It seemed that the research participants had difficulty returning to the interview and one of the interviewees suggested one reason for this: 'It is sometimes difficult to concentrate when you know the ward is busy.' The interviews could have been more successful if a specific time had been identified for them and adhered to, as well as conducting them in a room where disturbances were kept to a minimum. COMBINING METHODS As previously asserted, one of the benefits of using interviews as well as observations was that they allowed the issues to be explored further. This also helped in coming to terms with the researcher's lack of participation during the observations. A combination of different research methods can also increase the validity of the findings. Becker and Geer (1970) stated that: 'An observation of some social event, the events which precede and follow it, and explanations of its meanings by participants and spectators, before, during and after its occurrence. Such a datum gives us more information about the event under study than data gathered by any other sociological method.' Utilizing a combination of data collection methods in this study overcame two potential problems: To have used interviews alone would only have represented the participants' viewpoint To have used observations exclusively would not have allowed the participants to present their own perspective on what had occurred. CONCLUSION The utilization of direct observations and semi-structured interviews in this study was beneficial to data collection. On occasions, problems were experienced and many of the problems encountered had not been anticipated initially. It is clear that the process can be enhanced by careful preparation. The environment should be vetted thoroughly before starting the study and the role of the researcher should also be clarified at an early stage. The aims of both the observations and interviews should be clear and opportunities to discuss sensitive issues should be offered. The participants should be fully informed about the research aims and time for reflection and note taking should be a priority. The opportunity to explore issues in the 'real nursing world' where the context is part of the research itself is a significant advantage of this type of research. The many variables within nursing practice, although problematic, can be taken into consideration to produce a richer picture. When empirical research is conducted away from the clinical setting, the findings can be idealistic and estranged from the reality of clinical constraints. This highlights the importance of conducting research in the subjects' natural environment where the researcher becomes aware of the problems surrounding practice, and the risk of implementing research that is far removed from that reality is reduced. REFERENCES Bannister D (1981) Personal construct theory and research method. In Reason P, Rowan J (Eds) Human Inquiry: A Sourcebook of New Paradigm Research. Chichester, John Wiley & Sons. Becker HS, Geer B (1970) Participant observation and interviewing: a comparison. In Filstead WJ (Ed) Qualitative Methodology: Firsthand Involvement with the Social World. Chicago IL, Markham. Bogdan R, Taylor SJ (1975) Introduction to Qualitative Research Methods: A Phenomenological Approach to the Social Sciences. New York NY, John Wiley. Breakwell GM (1990) Interviewing, Problems in Practice. London, British Psychological Society, Routledge. Cohen L, Manion L (1989) Research Methods in Education. Third edition. London, Routledge. Duffy ME (1985) Designing nursing research: the qualitativequantitative debate. Journal of Advanced Nursing. 10, 225-232. Glaser BG, Strauss AL (1967) The Discovery of Grounded Theory. New York NY, Aldine De Gruyter. Gold RL (1958) Roles in sociological field observation. Social Forces. 36, 217-223. Leininger M (1985) Qualitative Research Methods in Nursing. New York NY, Grune & Stratton. Massarik F (1981) The interviewing process re-examined. In Reason P, Rowan J (Eds) Human Inquiry: A Source book of New Paradigm Research. Chichester, John Wiley & Sons. Sapsford R, Abbott P (1992) Research Methods For Nurses and The Caring Professions. Buckingham, Open University Press. © RCN PUBLISHING COMPANY 2000