GENE/DOWN SYNDROME, A CLINICAL BIOLOGICAL AND
advertisement

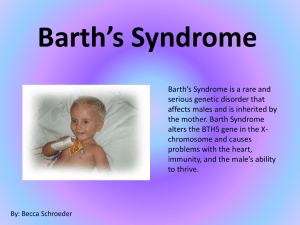
GENE/01(O).DOWN SYNDROME, A CLINICAL BIOLOGICAL AND GENETIC PROFILE K R Lahiri; Satish Department of pediatrics, Seth G S Medical College and KEM Hospital Mumbai 400012 Down syndrome (DS) is diagnosed clinically by its characteristic features and associated systemic malformation and there is a wide variation amongst individuals in the clinical manifestations. Aims and Objectives: This study was done to analyse the demographic and physical features, the distribution of cases in children with Dwon syndrome; with respect to maternal age, associated systemic malformations, occurrence of hematological and thyroid disorders and the pattern of cytogenetic abnormalities. Methodology: It was a retrospective study performed in a tertiary care centre involving random 114 cases of down syndrome confirmed by karyotype. Results: Of the total (n=114) cases, 68 were males and 46 females, average age of presentation was 18.8 months, and commonest age distribution of mothers was between 20-30 years (55.2%) followed by 30-40 yrs (41.2%). Most common cause for referral was dysmorphic features; followed by congenital heartdisease and delayed milestones. Hypotonia, mongoloid slant, flat face and epicanthal fold were the most common minor malformations. Non-disjunction was the most common (93%) cytogenetic abnormality. Most common major malformation was congenital heart disease (59%), followed by thyroid dysfunction (14.9%) and Gastro intestinal anomalies (3.5%). Endocardial cushion defect was seen as most common congenital heart disease followed by VSD and PDA. All physical features may not be present in all cases although hypotonia, mongoloid slant, epicanthal fold, flat face are seen in >50% cases. As many cases may be asymptomatic; all infants with Down syndrome should undergo 2 D-echo/color doppler study. Regular thyroid function tests should be done in cases of all age groups, It is prudent to advice non-invasive tests for antenatal screening for Down syndrome for all women irrespective of age. GENE/02(P).ALLAN-HERNDON-DUDLEY SYNDROME- A CASE REPORT Sanjay Verma, M.M.A.Faridi Department of Pediatrics, University College of Medical Sciences & Guru Tag Bahadur Hospital, Dilshad Garden, Delhi. Allan-Herndon-Dudley Syndrome (AHDS) is a rare X-linked disorder caused by mutation in the gene encoding the monocarboxylate transporter-8. We report a child with suggestive clinical and lab parameters. CASE REPORT: A 10-year-old child presented with global developmental delay, feet contractures, nystagmus and impaired hearing. There was a history of generalized weakness, hypotonia, reduced muscle mass and delay in developmental milestones since childhood. Birth history was normal & there was no similar family history in last three generations. On examination, vitals were normal; while anthropometry was: Wt 20 kg, Ht 128 cm, HC 49 cm and CC 57 cm. Child had an elongated face, large simple ears; high arched palate, bilateral ptosis, nystagmus, dysarthria & impaired hearing. Generalized muscular wasting, bilateral equines deformity of feet, cubitus valgus, scoliosis, pectus-excavatum & testicular atrophy were other associated findings. Routine lab investigations including karyotyping ware normal. Thyroid profile revealed: Free T3=730 pg/dL(N=230-660pg/dL), Free T4=1.0 ng/dL(N=0.8-2.2 ng/dL) & TSH=4.4 mIU/L(N=0.76.4 mIU/L). This was consistent with findings suggestive of AHDS. Child was advised corrective surgery for feet deformity & he is still on our follow- up. DISCUSSION: AHD Syndrome is characterized by mutations in the monocarboxylase transporter-8 gene. Protein encoded by this gene is needed for the transport of T3 into neurons. Abnormal transporter function is reflected by elevated free T3 & lowered free T4 levels in the blood. Infancy and childhood are marked by hypotonia, weakness, reduced muscle mass and delay of developmental milestones. Facial manifestations are not distinctive, but the face tends to be enlarged, ears are often simply formed or cupped. There is generalized weakness & speech is often dysarthric. Hypotonia gives way to spasticity in adult life & contractures usually develop at joints. Cognitive development is severely impaired & behavior tends to be passive. Clinical signs of thyroid dysfunction are usually absent in affected males, GENE/03(P).MITOCHONDRIAL ACETOACYL-COA THIOLASE (Β-KETOTHIOLASE) DEFICIENCY Radha G. Ghildiyal, Milind S. Tullu, Niranjan Singh, Shrinivas Tambe Department of Pediatrics, T.N. Medical College & BYL Nair Hospital, Mumbai 400008 Introduction: Mitochondrial acetoacyl-CoA thiolase deficiency is a rare autosomal recessive disorder leading to organic academia (gene location- long arm of chromosome 11). Case report: 15months-old girl born of third degree consanguineous marriage was admitted with acute gastroenteritis (grade II dehydration), acidotic breathing, and altered sensorium. In-spite of adequate rehydration, the patient had persistent metabolic acidosis with alteration of sensorium. The septicemia work up was negative. Further investigations revealed high anion-gap acidosis with ketonuria with mild hyperammonemia, hence provisionally diagnosed as an organic acidemia. His serum & urine gas chromatography - mass spectroscopy was suggestive of mitochondrial acetoacyl CoA thiolase deficiency. Patient responded dramatically to bicarbonate infusion and is presently being treated with oral carnitine and low protein diet. Similar disorder exists in the elder sibling (diagnosed as organic acidemia). Discussion: Mitochondrial acetoacyl-CoA thiolase deficiency is a rare genetic disorder with variable clinical manifestations (ranging from asymptomatic course to repeated attacks of severe metabolic acidosis wit intercurrent infections). Mental development is usually normal with treatment (with a favorable prognosis). Acute episodes are treated with adequate hydration and bicarbonate infusion (for acidosis). Long term management includes restriction of protein intake and oral carnitine. GENE/04(P).OSTEOGENESIS IMPERFECTA TYPE III: A CASE REPORT Karuna Thapar, Naresh Jindal Department Of Paediatrics, Government Medical College & Hospital Amritsar Osteogenesis Imperfecta is disorder with congenital bone fragility caused by the mutations in the genes that codify for Type I procollagen (COLA1A1 and COLA1A2) According to Sillence et al, 4 types have been described, out of which Type-II is lethal in infancy , however, Type-III can have a full life span. No information available regarding exact prevalence, however, in U.S., estimated to be 1 / 20000 live births. We are reporting such a case admitted in Department of Paediatrics, Government Medical College, Amritsar due to its rarity. Case report: A 7 year old female child admitted with progressive bowing of legs , multiple bone fractures and respiratory distress since last 2 years. Perinatal history uneventful and development normal till 5 years of age. Father and mother were short statured but didn’t have any fractures. On examination, a wide open anterior fontanelle , flat mid-face , frontal bossing, multiple fractures involving both clavicles, Humerus, femurs, tibias, pectus carinatum of chest wall, exaggerated metaphyseal flaring at wrist with slender diaphysis, scoliosis and slight bluish sclera was seen. Child was short statured (length 82 cms, < 3rd percentile) and macrocephalic (HC 60 cms ) . There was no hearing loss and neurological examination was normal. Child was having severe bronchopneumonia and CCF probably due to immobility from a long time. Radiological examination has shown multiple bone fracture with loss of bone mass, also popcorn appearance at knee joint was seen. She was classified as Type-III OI according to Sillence classification. GENE/05(R).EDWARDS SYNDROME, A CASE REPORT B.K.Meher, P.Mishra, K.J.Prusty,A.K.Mohanty S.V.P.Post Graduate Institute Of Paediatrics Trisomy 18 is the second most common multiple malformation syndrome with an incidence of 1 in 8000 live births. Indivisuals with such conditions have distinct phenotypic features like malformed ears, microcephaly, cleft lip/palate, micrognathia, epicanthal folds and cardiac defects like VSD and PDA. Clenched fisting with index finger overlapping the 3rd and 4th fingers as almost distinctive of this disorder. The survival rate is low with a very poor prognosis. Recurrence risk is very low(<1%). With h/o a sibling death (1 1/2 year female child ), due to unknown cause , a full term, 1500gm, four day female baby of Yasoda Sahu, born vaginally in hospital, a product of nonconsanguious marriage, without any h/o birth asphyxia, PROM, Prolonged labor, maternal illness or drug intake, presented with chief complaints of refusal to feed for 2 day. Clinical examination revealed weight :1500gm; length:39cm; head circumference:29cm; chest circumference:29cm; conscious baby with pulse rate =130/min; resp rate=64/min, regular AT; prominent occiput; micrognathia; low posterior hairline; prominent chest wall with decreased breath sounds on right side, short sternum; scaphoid abdomen; acrocyanosis(recovered after O2 inhalation); CTEV(left); bilateral closed fisting with 5th digit overlapping 4th and index finger overlapping middle finger, short nails on all digits and dactylography showing simple arch pattern in all digits. Investigation revealed Hb=10gm%, TLC=6000mm3, DC=N32E2L60M6B0, chest X-ray showed Diaphragmatic Hernia on right side and short sternum. Cytogenetic analysis of PHA stimulated peripheral blood lymphocytes revealed a Female karyotype with the presence of an extra copy of chromosome 18 (trisomy 18) in all the cells analysed. The condition is confirmed to be Edwards Syndrome. GENE/06(P).AUTOSOMAL DOMINANT CATARACT - A FAMILIAL DISORDER Ashish Lothe, Abhishek Paralikar, Pallavi Saple, Vidya Pawar, Kalpesh Date, Vijaya Bohra, Piyush Shah Department of Pediatrics, Grant medical College/Cama & Albless hospital, Mumbai Congenital cataract is a common major abnormality that frequently causes blindness in infants. One third of all cases can have family history mainly affecting siblings. The etiologies include congenital infections like Rubella, Chicken Pox, Toxoplasmosis or metabolic disorders or Down Syndrome. But cases with familial inheritance are very rare. Autosomal dominant congenital cataract seems to be the most common form of congenital cataract. Mutations at multiple sites have been incriminated. We report a family where congenital blindness was inherited through 5 successive generations. 2 year old male child born of non consanguinous marriage was admitted with complaints of impaired vision and white opacity in both eyes noticed by parents since birth. Child was not looking at parents or other objects but used to turn head to sounds. Linguistic development was normal. There was affection of individuals in 5 successive generations who had congenital cataract depicting autosomal dominant inheritance. On examination child had growth retardation without microcephaly or any dysmorphic features. Systemic examination was normal. Ophthalmic evaluation revealed bilateral mature cataract. Father’s ophthalmic evaluation revealed the same findings. Karyotyping showed no abnormality. Linkage analysis for mutations couldn’t be done. The familial cataracts, if operated early in life give better outcome. Counselling regarding the pattern of inheritance and early detection and surgery is beneficial. GENE/07(P).NEURAL TUBE DEFECTS-A CLINICAL PROFILE V.Priyavarthini,Saradha suresh,K.Seeniraj,Mangayarkarasi senguttuvan Institute of child health and hospital for children,Egmore,Chennai-600008 Neural tube defects are a spectrum of illnesses that pose several challenges in management and follow up. The psychological impact to the mother and the family is huge. Ironically, they are preventable. Aim: To study the clinical profile of neural tube defects in children in a tertiary care centre. Study design: Descriptive study. Methodology: 67 children presented with meningocele and myelomeningocele to the Department of Paediatric Surgery, Institute of Child Health, Chennai in the year 2005 were studied. Age at presentation, sex, antenatal history, clinical features, associated factors, management and outcome were recorded. Statistical analysis: Outcomes expressed in tables and percentages. Results: Open neural tube defects were commoner (60%) with preponderance for the lumbo-sacral region. Neurological deficits were present in 75%, CSF leak in 45% and meningitis 5%. Associated congenital malformations were detected in 50%. USG cranium revealed hydrocephalus in 25% and agenesis of corpus callosum in 30%. The sex distribution was equal. Term newborns predominated (78%). A sizeable proportion (40%) presented beyond the neonatal period. Consanguinity was present in 20%. Surgery was done in about 50% of cases with uneventful post-operative period. Antenatal USG was done in 15% of cases. There was no documented or reliable history of periconceptional folic acid intake. Conclusions: Periconceptional supplementation of folic acid to all women of child bearing age as part of RCH program is reemphasized and should be promoted vigorously to prevent the occurrence of neural tube defects. Early referral may help improving the outcome in significant proportion of cases. GENE/08(P).MECKEL GRUBER SYNDROME - A RARE ENTITY Prashant Patil, Ashish Lothe, Pallavi Saple, Ashok Rathod Department of Pediatrics, Grant amedical College/Cama & Albless hospital, Mumbai Meckel Gruber syndrome is rare lethal autosomal recessive disorder characterized by triad of encephalocele, postaxial polydactyly and large polycystic kidneys caused by failure of mesodermal induction. Associated congenital anomalies are soft palate, wide anterior fontanelle, pulmonary and hepatic hypoplasia. Infants with Meckel Gruber syndrome can be diagnosed based on their appearance at birth, or by ultrasound before birth, usually in the second trimester of pregnancy. Finding at least two of the three features of the classical triad, in the presence of normal karyotype makes the diagnosis. Here we present a case admitted with all features of this syndrome. Full term male newborn weighing 2.6 kg, born of non consanguinous marriage, was admitted in NICU with severe respiratory distress, & multiple congenital malformations. There is no family history of similar complaints or any significant antenatal complaints. Baby had malformations including occipital encephalocele, right hand polydactyly, soft cleft palate, receding forehead, short neck & small narrow chest. External genitalia were normal. X ray chest showed pneumonia. Ultrasound revealed had bilateral polycystic kidneys with pelvic urethral obstruction, with hepatomegaly with altered texture with normal biliary system. Liver & renal function tests were normal. Ultrasound of skull showed occipital meningoencephalocele with herniation of 3/4th of brain matter into sac with obstructive hydrocephalus. Karyotyping was normal. Patient was ventilated within few hours of birth but succumbed to death. The diagnosis is clinical & requires presence of classic abnormalities of this extremely rare disorder. GENE/09(O).SPECTRUM OF LEUKODYSTROPHIES AT A GENETIC CLINIC IN MUMBAI Parag M Tamhankar, Mamta N Muranjan, Shilpa Ranade, Pratima Kondurkar Genetic Clinic, Department of Pediatrics, KEM Hospital, Parel, Mumbai Leukodystrophies are determined group of progressive disorders affecting myelin in the brain, spinal cord and peripheral nerves. Aims and objectives: To study the clinical, biochemical and neuroradiological features in different types of leukodystrophy. Material and Methods: Cases diagnosed as leukodystrophy on the basis of clinical features and /or specific enzyme assay over a period of 8 years from January 1996 through December 2003 were analyzed retrospectively. Results: 34 cases (M: F ratio= 1.26) were diagnosed. Krabbe disease (41.2%) and metachromatic leukodystrophy (29.4 %) were the commonest. Rare disorders: Canavan disease 5.9%, cerebrotendinous xanthomatosis 5.9%, X-linked adrenoleukodystrophy 2.9%, Pelizaeus Merzbacher disease 2.9%, megalencephalic leukoencephalopathy with subcortical cysts 2.9%, neuronal ceroid lipofuscinosis 2.9%, and undiagnosed cases 5.8 %. Common ages at presentation were late infantile (50%) & early infantile presentation (26.5%). Cognitive impairment (70.6%) and neuroregression (64.7%) were the most frequent followed by developmental delay (35.3%), speech abnormality (35.3%), seizures (35.3%), gait disturbances (11.8%) and visual impairment (8.8%). Abnormality of higher functions was found in 67.6%, 35.3 % had hypotonia, 50% had hypertonia, 38.2% had hyperreflexia, and 32.3% had hyporeflexia. Cataracts were detected in cerebrotendinous xanthomatosis. Abnormal investigations: elevated CSF protein level in Krabbe disease (6 cases), Xlinked adrenoleukodystrophy (1 case), severe sensory motor neuropathy in metachromatic leukodystrophy (3 cases), Krabbe disease (5 cases). Enzyme assays or confirmatory studies were done in 91.2% patients. Neuroimaging was done in 94.1%. The changes noted were: deep white matter changes (70.6%), peripheral white matter involvement (26.5 %), gray matter involvement (17.6%), lack of myelination or delayed myelination (20.6%), non specific white matter pattern (11.8%), cerebellar involvement (38.2%), cerebral atrophy (14.7%), abnormalities of basal ganglia (14.7%), thalamic abnormalities (8.8%), brain stem involvement (20.6%) and involvement of corpus callosum (14.7%). Conclusion: Metachromatic leukodystrophy and Krabbe disease were the commonest. Early and late infantile disease was the most frequent presentation. Cognitive impairment and neuroregression with gait and/ or speech abnormalities should arouse suspicion. Characteristic abnormalities of white matter on neuroimaging can aid diagnosis. GENE/10(R).HOLT ORAM SYNDROME: A CASE REPORT Bhatia Ravi, Gupta M, 1-ra-6,gaytri Nagar, Hiran magri sector 5,Udaipur 313002 Introduction: Holt Oram Syndrome is a heart upper limb malformation with an autosomal dominant Inheritance and near complete penetrance with variable expression. First described in 1960. The responsible gene has been mapped to band 12q 24:1 Case History: One and half year old male born out of non consanguineous marriage was admitted to our ward with complaints of fever and cough of five days duration .On examination the patient was febrile,HR 180/min,RR 68/min,Resp sys :bilateral crepitations, SCR, ICR. CVS: low pitched mid diastolic murmur at the lower sternal edge and apex. I st heart sound was normal and there was fixed splitting of second heart sound. Thumbs in both hands were absent since birth and there was webbing of little and ring fingers at base in both hands. Investigation revealed Hb of 10gm/dl,TLC 10,600/cu.mm.X Ray chest showed Bilateral Infiltration and there was no cardiomegaly.X Rays of both hands revealed absent thumbs other bones being normal.2-d color Doppler echo revealed a 18 mm wide ASD Secndum defect with left to right shunt. Based on the above findings a diagnosis of Holt Oram Syndrome was made. Parents were counseled about the disease. The patient was treated for bronchopneumonia and advised surgery for cardiac ailment at a later stage since the cardiac problem was not interfering with daily activities GENE/11(P).PEUTZ-JEGHERS SYNDROME A.R. Dhongade, R.R. Palliana,N. Birla M. Deogaonkar, R.K. Dhongade Department of pediatrics,Sant Dyaneshwar Medical Education Trust, Pune 4110030 Peutz-Jeghers syndrome is a very rare autosomal dominant inherited disorder associated with intestinal polyposis (hamartomas typically) and mucocutaneous pigmentation ( perioral, perianal and on the digits ). The etiology is a genetic mutation of the gene STK11/LKB1 located on band 19p13.3. Our patient was a 13 year old boy who presented with complaints of colicky abdominal pain in the epigastric region since 6 months which occurred intermittently and was aggravated after consumption of food. The pain would be relieved by antispasmodics. The child also had multiple melanotic macules 1-5mm in size, in the perioral and perianal areas which were present since 1 yr. the patients father also had similar complaints. A barium meal follow through revealed a radioluscent filling defect in the body of the stomach, which appeared to be a polyp. Histopathology of polyp revealed extensive smooth mucle arborisation which was characteristic of Peutz-Jeghers syndrome. Peutz Jegher's syndrome has a very rare occurrence rate(1 in 60,000) with equal sex distribution.Cancer soon develops into the gastrointestinal tract with overall incidence more than general population.Pigmented lesions make early diagnosis possible in pediatric patients which usually fade away by puberty. GENE/12(P).CAMPOMELIC DYSPLASIA - A UNIQUE SKELETAL DISORDER Prashant Patil, Ashish Lothe, Pallavi Saple Department of Pediatrics, Grant amedical College/Cama & Albless hospital, Mumbai Campomelic dysplasia is a severe rare form of congenital short limbed dwarfism characterized by Campomelia (congenital bowing of long bones) associated with skeletal & extraskeletal features including cleft palate, hypoplastic scapulae, distinctive facial features, narrow bell shaped thorax, , pretibial pits, hypoplastic lungs, club feet, malformations of cervical spine, heart, & kidneys. Another characteristic feature is male to female sex reversal seen in two-thirds of XY cases. It is an autosomal dominant disorder caused by mutations in the SRY related gene called SOX9. We describe a case of this unique fatal type of skeletal dysplasia. Full term female child born to primi gravida by emergency Caesarean section with 1st & 5 th minute apgar scores of 5 & 7 respectively was admitted with congenital malformations and severe respiratory distress. There was no significant family history. Antenatal ultrasound had recorded single intrauterine fetus showing multiple limb deformities with polyhydroamnios. Anthropometry revealed weight of 2.6 kg, & length of 37 cms with upper to lower segment ratio of 2:1 depicting short limbed disproportionate short stature. Head circumference was 33 cms. On examination baby had multiple skeletal malformations like bowing of long bones, narrow bell shaped chest, cloverleaf shaped skull, soft cleft palate, distinctive flattened facies, bilateral talipus equinovarus, pretibial pits & multiple café au lait spots. Patient had severe respiratory distress with inspiratory crepts, & hepatosplenomegaly with apparently normal other systemic examination. X ray showed bowing & angulations of all long bones with telephone handle appearance, flat vertebral bodies, normal ribs, hypoplastic pelvis & scapulae. Abdominal ultrasound was showing hepatosplenomegaly with normal genitalia. Karyotyping was normal. Patient was ventilated within an hour of life, but general condition didn’t improve & she died on day 6 of respiratory insuffiency. This disorder is almost fatal with purely clinical diagnosis substantiated by classical radiological features. GENE/13(P).EPIDERMOLYSIS BULLOSA IN IDENTICAL TWIN :- A RARE ENTITY Sushma Save, Hitesh Bhambani, Sangeeta Amladi, Balu Rathod, Archana Kher, Alka Jadhav From :- Department of Pediatrics, TNMC & BYL Nair Hospital Mumbai -8. Introduction:- Epidermolysis Bullosa (EB) is the group of genetically determined disorders characterized by excessive susceptibility of the skin & mucosa to separate from the underlying tissues following mechanical trauma. Here we report the rare case of EB. Case History:- A pair of twin female, born of II degree consanguineous marriage presented with vesico-bullous leasion at birth. 18-20hr of life they had bilateral bullae & blistering of arms & legs. Examination revealed multiple fluid filled leasions on body. Few tense, few flaccid with sero- sanguinous fluid, few dried up leasions with scarring. On aspiration clear serous fluid obtained. Skin Biopsy (H&E stain) showed findings suggestive of dystrophic / junctional EB. Histologically babies have features of DEB / JEB, correct type will be obtained after electron microscopy & immunohistochemestry, which has been arranged. Babies were treated with non-adhesive dressing, systemic & local antibiotic. Discussion:- EB is diverse group of disease that is characterized by skin blistering. Classification is based on clinical characteristic, inheritance pattern & the level of cleavage within the skin. This prominent histologic feature defines three main groups:- simplex (cleavage within the basal cells of the epidermis), junctional (within the lamina lucida of the basement membrane zone) & dystrophic(beneath the lamina densa of the basement membrane). At each level, there are several protein components that contribute to skin integrity. These molecules all are expressed in utero during the first trimester, allowing prenatal diagnosis. The simplified classification system that recognizes three major EB types, Epidermolysis Bullosa Simplex (EBS), Junctional Epidermolysis Bullosa (JEB), Dystrophic Epidermolysis Bullosa (DEB) & 11 minor subtype. The most precise diagnostic tool is carefully performed skin biopsy to obtain specimen for immunofluroscence mapping & ultrastructural study. To date the main stay of therapy for this group of disorder is supportive. GENE/14(P).GALACTOSEMIA- A CASE REPORT Sushma Save, Shrinivas Tambe, Sunil Jumnake, Archana Kher From :- Department of Pediatrics, TNMC & BYL Nair hospital, Mumbai-8. Introduction:- Galactosemia is an autosomal recessive disorder caused by inability to metabolise galactose & it has prevalence of 1 in 60,000. Here we report this rare case of galactosemia. Case History :- Day 5 old full term female child with birth weight of 2.3kg,cried immediately after birth born of non-consanguineous marriage presented with lethargy, refusal of feed, seizure &yellowish discoloration of skin since day 2 of life. Baby was breastfed on day one of life. Examination revealed deep icterus, neck retraction, umbilical discharge. On systemic examination baby had poor cry, tone, activity & suck with significant hepatosplenomegaly. In view of presenting features, examination findings & evidence of hypoglycemia ,a possibility of metabolic disorder like galactosemia was made. Investigation showed positive screening test for galactosemia & enzyme assay revealed GALT (Galactose-1 Phosphate Uridyl Transferase) deficiency. Hence baby was started on galactose free diet. Discussion :- “Classic Galactosemia” is a serious disease with early onset of symptoms. It is due to structural gene mutation producing altered enzyme (GALT), which does not function normally. Some individuals homozygous for another gene, called Duarte variant, normally have half-normal GALT levels & are asymptomatic. The accumulation of galactose can cause complications such as feeding problems, vomiting, sepsis, diarrhea, dehydration hypoglycemia, jaundice, liver failure, kidney failure & brain damage. Galactosuria at birth but develop gradually over weeks to months. Mental retardation evident after 6-12 months & is usually irreversible. Sepsis to E.coli is frequent among galactosemic neonates & can cause death. The mainstay of therapy is lactose free diet, soy milk is beneficial for infants. Carrier testing & prenatal diagnosis can be performed by direct enzyme analysis of amniocytes or chorionic villi. Early diagnosis & treatment have improved the prognosis of galactosemia. GENE/15(P).CAREY- FINEMAN- ZITER SYNDROME : A RARE CASE Jyoti Suvarna, C T Deshmukh, Parag Tamhankar Department of Pediatrics, Seth G. S. Medical College & K.E.M. Hospital, Acharya Dhonde Marg, Mumbai- 400012. Introduction: Carey- Fineman- Ziter Syndrome is a very rare inherited disorder characterized by features of Moebius syndrome (unilateral or bilateral facial palsy with or without other craniopathies like XII, VI, IX or X palsy, with or without other malformations), Pierre Robin sequence (micrognathia with high arched palate or cleft palate) and muscle disorder (hypotonia or myopathy). Aim: To study the clinical profile of Carey- Fineman- Ziter syndrome. Case Report: A five month old child (born of a non-consanguineous marriage) came with fever, cough, and breathlessness for 5 days. He was a full term normal delivery (birth weight- 2.7 kg) but had feeding difficulties (requiring gavage feedings), recurrent respiratory tract infections and failure to thrive since birth. On examination child had a weak cry, poor gag, pooling of secretions, expressionless myopathic face due to bilateral facial diplegia, micrognathia, high arched palate hypotonia (floppy infant), and developmental delay (motor more than mental). X ray chest and CT chest showed a right upper and middle lobe atelectasis secondary to aspiration. CPK levels, laryngoscopy, USG brain and fundoscopy were normal. EMG showed primary muscle disorder. Carey- Fineman- Ziter syndrome was diagnosed on the basis of features of Moebius syndrome (bilateral VII nerve palsy with IX, X nerve palsy), Pierre Robin sequence (micrognathia with high arched palate) and muscle involvement (hypotonia with myopathy). Discussion: Although Moebius syndrome is well known clinical entity, Carey Fineman Ziter syndrome is rare and may be missed if not looked for. It is proposed to be due to a gene defect causing a failure in the formation of the motor nucleus of the VIIth cranial nerve and a type of muscular dysgenesis characterized by hypotonia and sometimes myopathy and congenital contracture. Feeding difficulties may lead to life threatening respiratory infections. The recurrence risk is higher than common Moebius syndrome. GENE/16(R).MACRODYSTROPHIA LIPOMATOSA- A CASE REPORT Harsh Gupta, Vikas Tripathi Acharyashree Bikshu Government Hospital, Moti Nagar, New Delhi Macrodystrophia lipomatosa is a rare form of localized gigantism characterized by overgrowth of all mesechymal elements of a digit. The abnormality is always unilateral and in the distribution of the median nerve (upper extremity) or/and the plantar nerve (lower extremity). The cause of this condition is obscure. A 9 months old female baby presented to the hospital with complaints of enlarged 2nd and 3rd toes of left leg. The enlargement of toes was gradual since birth. There was no local change in color, pain or constitutional symptoms. There was no family history of similar problem. There was no adverse antenatal history. On local examination, 2nd and 3rd left toes were enlarged in both vertical and transverse directions, to the size more than double on the right side. There was syndactyly of the soft tissue component of the second and third toes at the level of the proximal phalanges. There was no tenderness, dilated vessels or pitting edema over the toes. Movement of toes was painless. Rest of general and systemic examination was normal. On imaging, X- ray showed both bony and soft tissue overgrowth. Phalanges were enlarged both in length and transverse dimension with normal trabecular pattern. Translucencies in soft tissue were seen due to an increase in adipose tissue. A diagnosis of macrodystrophia lipomatosa was made on above findings. This case is being reported because of its rarity. Figure 1a & 1b: Clinical image & X-ray of 2nd & 3rd left toes showing macrodystrophia lipomatosa.