Furcation involved teeth :
advertisement

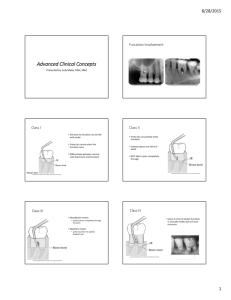
Furcation involved teeth :-(furcation involvement) The term furcation involvement :refers to the involvement of bifurcation or trifurcation of the multirooted teeth by the periodontal diseases. The bacterial plaque is the causative agent of the gingivitis and destructive periodontal disease causes destruction of the periodontal tissues. . Objectives of these procedures:1-to obtain visibility and access such areas of the roots to proper professional debridement. 2-To eliminate the pathologically depend on p.d pockets. 3-To establish the morphology of dentogingival region which facilitate the proper self performed tooth cleaning. Anatomical characteristics:General information regarding the anatomy of the function areas may be gained an autopsymaterial the buccal or labial plate of the alveolar bone may be thin or sometimes exposing the root surface so we may have dehiscene which is a dipping in the crestal bone margin in or fenestration which is circumscribed window like in the cortical plate over the root surface . 2 Diagnosis of furcation involved teeth:The examination of the teeth should include both probing and radiographic analysis . clinical examination done by using graduated perio-dontal probe,curred explorer or small curettes, because the involved teeth may have only a pin point area to be detected. Factors play a role in the etiology of the furcation involvement:1-plaque from progressive periodontal diseases. 2-Trauma from occlusion (injury from trauma). 3-Enamel .projections. Morphological variation:1-incisors and canines has tow roots for each and so we have tow furcas. 2-mand premolars----3 roots. 3-max premolars----3 roots. 4- mandibular molar ----4 roots . 5-fusion of divergent roots. 6- cervical E projection or E pearls in the furcation area. 3 7- Accessory pulp canals which communicates with the furcation areas. Classification of furcation involvement:Degree1(grade 1):- is the incipient or early lesion ,in which there is suprabony pocket involving the periodontal tissues surrounding the area Or:-horizontal loss of the periodontal tissue support not exceeding 1/3 of the width of the tooth . Degree2(grade 2):- bone destruction on one or more aspects of the furaction ,but a portion of the alveolar bone and periodontal ligament remains intact. or :-horizontal loss of the periodontal tissue support not exceeding 1/3 of the width of the tooth . Grade3(degree 3):- the interradicular bone is completely absent, but the facial and /or lingual orifices of the furcation are occluded by the gingival tissue ,these fore the furcation opening cannot be seen clinically ,it a through and through tunnel . 4 Or :-horizontal through and through destruction of periodontal tissues of furcation areas. Some times we have also:Degree4(grade4):- as in the grade 3, we have destruction of the interradicular bone ,but also we have recede of gingival tissue apically ,so that the furcation opening is clinically visible with out coverage by the gingival. Rational therapy of furcation involvement:Therapeutic alternatives for different degrees of the involvement Degree1 :- scaling and root planning , furcation plasty. Degree2:-furcation plasty Tunnel preparation Root resection Tooth extraction Degree3:-tunnel preparation Root resection Tooth extraction 5 Furcation plasty:Include the following procedures:1-Reflection of mucoperiosteal flap to get better access to the interradicular area. 2-Removal of soft and hard bacterial deposits and inflammatory soft tissue from furcation area. 3-Odontoplasty i.e removal of tooth substance in the furcation area in order to widen an arrow entrance of the furcas. 4-Osteoplasty :i.e recontouring of bony defect in the furcation area. 5-Repositioning and suturing of the flap . there for furcation plasty is done in advanced degree1 and initial degree2 involvement and to over come the difficulties of large contact area of max molar and premolars. Objectives of furcation plasty :6 1-removel of plaque and calculus. 2-establish a condition in the dento gingival region which facilitate the self performed plaque control. Tunnel preparation:It means surgical exposure of the furcation area , it is remained either open or close by flap . the flap is alterated ei buccally and lingually , then the roots surfaces are scaled and planned and irregular alveolar bone crests are recontoued. Surgical packs may be applied to prevent granulation tissue formation in the tunnel space during healing .mandibular malars are more suited for this mode of therapy . risks for caries lesion developed in the denuded root surfaces within and adjacent to such tunnels. The tunnels area should cleaned by interdental tooth brush which should immersed in fluoride sol . as a desensetizing agent . such method should be used with restriction and only in situation where there is enough space between the roots. 7 Root resection:This is the procedure of choice in the cases of deep grade 2 and grade 3 involvement . it means the removal of one or more roots from the multirooted teeth ,the risks of having an overhang of the tooth substance during tooth hemi section or root resection is important to carry out these procedures after flap alteration. Failures of furcation therapy:1-in adequate plaque control and maintenance. 2-Poor root resection technique. 3-Root caries. 4-Cracked roots. 5-Improper restoration. Molar furcation are complicated due to the presence of :1-fused roots. 2-Cervical enamel projections. 3-Enamel pearls. 4-Furcation ridges. 8 9 NEW ATTACHMENT AND GUIDED TISSUES REGENERATION-GTR. Aspects of periodontal healing:1-Regeneration 2-Repair 3-Attachment 1-Regeneration:-is the growth and differentiation of new cells and intercellular substance to form new tissue. It occurs by growth from the same type of the tissue that has been destroyed or from its precursor. 2-Repair:-Restoration of continuity of diseased marginal gingiva and reestablishment of by scar. Bone loss is arrested with mobilization of epithelial and connective tissue cells into the damaged area with increase mitotic division to provide the sufficient no. of cells. 3-New attachment:-Is the embedding of new periodontal ligament. Fibers into new cementum and attachment of epithelium to the tooth surface previously denuded by diseaas.The term re-attachment were used in the past to refer to the restoration of the marginal periodontium. Re-attachment:-refer to repair in the areas of root not previously opposed to the pockets but after surgical detachment of the tissues or 10 after traumatic tears in the cementum, tooth fractures, treatment of periapical lesion. Regeneration of periodontal ligament is the basis for new attachment because:1-periodontal ligament provides continuity between alveolar bone and cementum. 2-periodental ligament contain cells that can synthesize and remodel the 3 connective tissue of the alveolar part of periodontium. Evaluation of new attachment and bone regeneration:1-clinical methods:A- Pocket probing. B- Attachment level. C- Gingival indices. D- Bone level. 2- Radiographic methods. 3- Surgical re-entry. 4- Histologic methods. 11