family practice residency program evaluation
advertisement

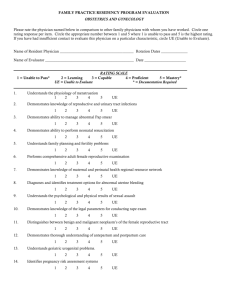
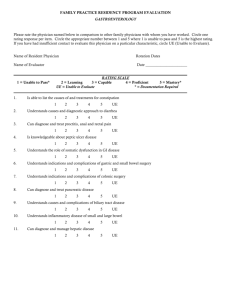
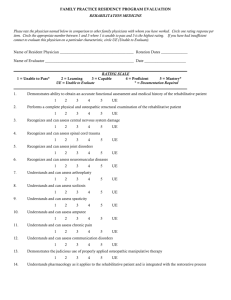
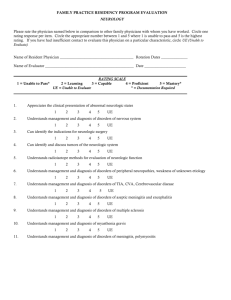
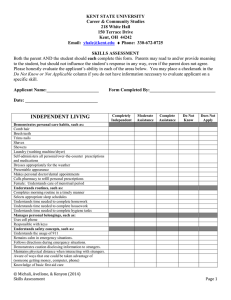
FAMILY PRACTICE RESIDENCY PROGRAM EVALUATION RADIOLOGY Please rate the physician named below in comparison to other family physicians with whom you have worked. Circle one rating response per item. Circle the appropriate number between 1 and 5 where 1 is unable to pass and 5 is the highest rating. If you have had insufficient contact to evaluate this physician on a particular characteristic, circle UE (Unable to Evaluate). Name of Resident Physician _______________________________________ Rotation Dates ______________ Name of Evaluator _______________________________________________ Date ______________________ ____________________________________________________________________________________________ RATING SCALE 1 = Unable to Pass* 2 = Learning 3 = Capable 4 = Proficient 5 = Mastery* UE = Unable to Evaluate * = Documentation Required ____________________________________________________________________________________________ 1. Understands the indications for and limitations of X-rays and scans 1 2. 5 UE 2 3 4 5 UE 2 3 4 5 UE 2 3 4 5 UE 2 3 4 5 UE 2 3 4 5 UE 2 3 4 5 UE Demonstrates knowledge of indications, techniques and limitations of venography 1 10. 4 Demonstrates knowledge of indications, techniques and limitations of arteriography 1 9. 3 Demonstrates knowledge of PET/CT, CTA, mammography and allied techniques 1 8. 2 Can interpret select plain films (skull, chest, C spine, LS spine and pelvis, survey abd and extremes) 1 7. UE Understands indications for fluoroscopy 1 6. 5 Understands side effects and complications of imaging studies 1 5. 4 Understands proper preparation for various imaging studies 1 4. 3 Understands frequency of ordering X-rays and proper sequence of ordering 1 3. 2 2 3 4 5 UE Demonstrates understanding of ultrasound scanner 1 2 3 4 5 UE 11. Demonstrates knowledge of indications, techniques and limitations of nuclear medicine, CT scan and MRI 1 2 3 4 5 UE Justification for 1 or 5_________________________________________________________________________ ____________________________________________________________________________________________ Comments___________________________________________________________________________________ ____________________________________________________________________________________________ _________________________________________________________ Evaluators Signature _______________________________________________________________ Program Directors Signature _______________________________________________________________ Resident Signature