The systemic inflammatory response to cardiopulmonary bypass
advertisement

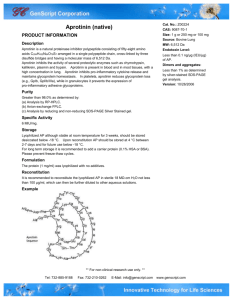
The systemic inflammatory response to cardiopulmonary bypass Collaborators: Ken Taylor, Dorian Haskard, Anna Randi, Clive Landis Cardiopulmonary Bypass (CPB) has been associated with some degree of major organ dysfunction since the earliest days of cardiac surgery. In the absence of infection or ischaemia, the concept of the “post-pump syndrome” or “Systemic Inflammatory Response Syndrome (SIRS)” is used 1. The clinical consequences of the inflammatory response vary from increased duration of hospital stay, to neurocognitive disorders, stroke, acute lung injury, multiple organ failure and death. The severity of SIRS attributable to CPB and the organs involved differ widely between patients, but the ischaemic lung appears to be particularly susceptible. The life threatening complication, Adult Respiratory Distress Syndrome (ARDS), occurs in 0.5 – 1.7% of CPB patients and can be associated with multiple organ failure, which carries a mortality of 50 – 92% 2. The mechanism of the inflammatory response in CPB is multifactorial. It combines operative trauma with contact activation of circulating blood components by the artificial surface of the bypass circuit, ischemia to major organs and endotoxin release from the gut. Systemic activation of complement, platelets, leukocytes and EC in turn leads to secretion of inflammatory mediators, such as IL-1, IL-6, IL-8 and TNF 3, 4 and generation of complement factors C3a, C5a and C5b-C9 (the membrane attack complex) 5. These are thought to lead to systemic vascular endothelial activation and leukocyte sequestration in organs 6, although direct evidence for these steps in humans is limited. Neutrophils and mononuclear phagocytes are thought to play an important role in lung injury by populating the affected organ and discharging their histotoxic contents. Activation of the circulating neutrophil pool has been demonstrated by elevated expression of Mac-1 (CD11b), and this occurs within 15 minutes of the commencement of bypass 7. Therapeutic effects of aprotinin Aprotinin (Trasylol) is a broad-spectrum serine protease inhibitor that has been in clinical use since the late 1980s to reduce blood loss during CPB surgery 8-10. It is an anti-fibrinolytic agent that inhibits the activity of plasmin 11. A significant additional benefit of aprotinin compared to other anti-fibrinolytic agents (eg. tranexamic acid) is that it appears to blunt the systemic inflammatory response to CPB 12, 13. A metaanalysis studying the cost and duration of hospital stay following CPB surgery has shown that aprotinin was the most effective treatment in high risk patients, compared to other state-of-the-art regimes, including leukocyte filtration, methylprednisolone administration or heparin-bonded circuitry 14. Clinically the effects of aprotinin are known to be mediated, at least in part, via reduced contact-activation of platelets and leukocytes 11, 15 and reduced inflammatory cytokine synthesis 16. Furthermore, during the 1995-1999 period, our in vitro and preclinical in vivo studies had suggested that aprotinin inhibits EC activation 17 and neutrophil transendothelial migration 18. Currently, Betsy Evans (BHF Clinical Research Fellow) is investigating the ability of aprotinin to prevent trapping of leukocytes in tissues during CPB, using cantharadininduced skin blisters 19. Changes in monocyte phenotype in response to CPB Cells of the monocyte/macrophage lineage are activated between 2-24h post-bypass, as demonstrated by elevated monocyte:platelet conjugate formation 20 and elevated expression of CD11b 21. In the context of our interest in monocyte-macrophage differentiation and anti-inflammatory function (see above), we have further explored the changes in monocyte surface phenotype induced by CPB. Our results suggest a change in monocyte function in response to surgery lasting for at least 2-3 days, such that monocytes post-operatively are more capable of interacting with immunecomplexes and scavenging Hb:Hp complexes 19, 22. We are currently exploring the putative anti-inflammatory phenotype of post-operative monocytes in more detail. References (1) Butler J, Rocker GM, Westaby S. Inflammatory response to cardiopulmonary bypass. Ann Thorac Surg 1993 February;55(2):552-9. (2) Asimakopoulos G, Smith PL, Ratnatunga CP, Taylor KM. Lung injury and acute respiratory distress syndrome after cardiopulmonary bypass. Ann Thorac Surg 1999 September;68(3):1107-15. (3) Lahat N, Zlotnick AY, Shtiller R, Bar I, Merin G. Serum levels of IL-1, IL-6 and tumour necrosis factors in patients undergoing coronary artery bypass grafts or cholecystectomy. Clin Exp Immunol 1992 August;89(2):255-60. (4) McBride WT, Armstrong MA, Crockard AD, McMurray TJ, Rea JM. Cytokine balance and immunosuppressive changes at cardiac surgery: contrasting response between patients and isolated CPB circuits. Br J Anaesth 1995 December;75(6):724-33. (5) Chennoweth DE, Cooper SW, Hugli TE, Stewart RW, Blackstone EH, Kirklin JW. Complement activation during cardiopulmonary bypass: evidence for the generation of C3a and C5a anaphylatoxins. N Engl J Med 1981;304:497-503. (6) Dreyer WJ, Michael LH, Millman EE, Berens KL, Geske RS. Neutrophil sequestration and pulmonary dysfunction in a canine model of open heart surgery with cardiopulmonary bypass. Evidence for a CD18-dependent mechanism. Circulation 1995 October 15;92(8):2276-83. (7) Asimakopoulos G, Kohn A, Stefanou DC, Haskard DO, Landis RC, Taylor KM. Leukocyte integrin expression in patients undergoing cardiopulmonary bypass. Ann Thorac Surg 2000 April;69(4):1192-7. (8) Royston D, Bidstrup BP, Taylor KM, Sapsford RN. Effect of aprotinin on need for blood transfusion after repeat open- heart surgery. L 1987 December 5;2(8571):1289-91. (9) Bidstrup BP, Royston D, Sapsford RN, Taylor KM. Reduction in blood loss after cardiopulmonary bypass using high dose aprotinin (Trasylol): studies in patients undergoing coronary bypass surgery, reoperations and valve replacement for endocarditis. Thorac and Cardiovasc Surg 1989;97:373-8. (10) Bidstrup BP, Harrison J, Royston D, Taylor KM, Treasure T. Aprotinin therapy in cardiac operations: a report on use in 41 cardiac centers in the United Kingdom. Ann Thorac Surg 1993 April;55(4):971-6. (11) van OW, Jansen NJ, Bidstrup BP, Royston D, Westaby S, Neuhof H, Wildevuur CR. Effects of aprotinin on hemostatic mechanisms during cardiopulmonary bypass. Ann Thorac Surg 1987 December;44(6):640-5. (12) Blauhut B, Harringer W, Bettelheim P, Doran JE, Spath P, LundsgaardHansen P. Comparison of the effects of aprotinin and tranexamic acid on blood loss and related variables after cardiopulmonary bypass. J Thorac Cardiovasc Surg 1994 December;108(6):1083-91. (13) Royston D. Aprotinin versus lysine analogues: the debate continues. Ann Thorac Surg 1998 April;65(4 Suppl):S9-19. (14) Gott JP, Cooper WA, Schmidt FE, Jr., Brown WM, III, Wright CE, Merlino JD, Fortenberry JD, Clark WS, Guyton RA. Modifying risk for extracorporeal circulation: trial of four antiinflammatory strategies. Ann Thorac Surg 1998 September;66(3):747-53. (15) Wachtfogel YT, Kucich U, Hack CE, Gluszko P, Niewiarowski S, Colman RW, Edmunds LH, Jr. Aprotinin inhibits the contact, neutrophil, and platelet activation systems during simulated extracorporeal perfusion. J Thorac Cardiovasc Surg 1993 July;106(1):1-9. (16) Tassani P, Augustin N, Barankay A, Braun SL, Zaccaria F, Richter JA. Highdose aprotinin modulates the balance between proinflammatory and antiinflammatory responses during coronary artery bypass graft surgery. J Cardiothorac Vasc Anesth 2000 December;14(6):682-6. (17) Asimakopoulos G, Lidington EA, Mason J, Haskard DO, Taylor KM, Landis RC. Effect of aprotinin on endothelial cell activation. J Thorac Cardiovasc Surg 2001 July;122(1):123-8. (18) Asimakopoulos G, Thompson R, Nourshargh S, Lidington EA, Mason JC, Ratnatunga CP, Haskard DO, Taylor KM, Landis RC. An anti-inflammatory property of aprotinin detected at the level of leukocyte extravasation. J Thorac Cardiovasc Surg 2000 August;120(2):361-9. (19) Philippidis P, Mason JC, Evans BJ, Nadra I, Taylor KM, Haskard DO, Landis RC. Hemoglobin Scavenger Receptor CD163 Mediates Interleukin-10 Release and Heme Oxygenase-1 Synthesis: AntiInflammatory Monocyte-Macrophage responses in vitro, in Resolving Skin Blisters in vivo and Postoperatively Following Cardio-Pulmonary Bypass. Circulation Research 2004;94:119-26. (20) Rinder CS, Bonan JL, Rinder HM, Mathew J, Hines R, Smith BR. Cardiopulmonary bypass induces leukocyte-platelet adhesion. Blood 1992;79:1201-5. (21) Mathew JP, Rinder CS, Tracey JB, Auszura LA, O'Connor T, Davis E, Smith BR. Acadesine inhibits neutrophil CD11b up-regulation in vitro and during in vivo cardiopulmonary bypass. J Thorac Cardiovasc Surg 1995 March;109(3):448-56. (22) Stefanou DC, Asimakopoulos G, Yagnik DR, Haskard DO, Anderson JR, Philippidis P, Landis RC, Taylor KM. Monocyte Fc gamma receptor expression in patients undergoing coronary artery bypass grafting. Ann Thorac Surg 2004 March;77(3):951-5.