Functional dyspepsia patients have lower mucosal
advertisement

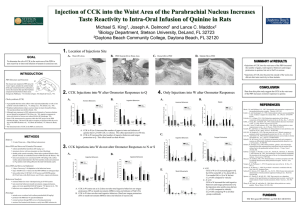
Functional dyspepsia patients have lower mucosal cholecystokinin concentrations in response to duodenal lipid O.S. van Boxel1; J.J.M. ter Linde1; J. Oors1, 5; B. Otto3; B.L.A.M. Weusten4; C. Feinle-Bisset2; A.J.P.M. Smout1, 5; P.D. Siersema, 1 1. Departement of Gastroenterology and Hepatology, University Medical Center Utrecht, the Netherlands. University of Adelaide Discipline of Medicine and Centre of Clinical Research Excellence in Nutritional Physiology, Interventions and Outcomes, Royal Adelaide Hospital, Adelaide, Australia. 3. Department of Gastroenterology , Medizinische Klinik - Campus Innenstadt, München, Germany. 4. Department of Gastroenterology , St. Antonius Hospital Nieuwegein, the Netherlands. 5. Department of Gastroenterology , Academic Medical Center Amsterdam, the Netherlands. 2. Introduction: Cholecystokinin (CCK)-1 receptor antagonism has been shown to relieve gastrointestinal symptoms induced by duodenal lipid load and gastric distension, demonstrating a role for CCK in postprandial symptom generation. Excessive release of CCK and/or hypersensitivity to CCK may explain the exaggerated response to duodenal lipid in functional dyspepsia (FD) patients. Thus far, only plasma CCK response has been determined in these patients; however, CCK acts in a paracrine manner, making mucosal levels in the duodenum relevant to measure. Presuming an excessive CCK release in FD, elevated levels of apolipoprotein A-IV (apoA-IV), a signaling protein released from enterocytes upon lipid absorption stimulating release of CCK, may also be found in FD. Aim: To investigate whether excessive fat-induced release of CCK at the level of the duodenum is involved in symptom generation in FD. Methods: Sixteen symptomatic FD patients and 10 healthy volunteers (HV) matched for age, gender and BMI (all normal weight) were included. All subjects underwent duodenal perfusions with Intralipid 20%, 2 kcal/min, for 60 min. Symptoms were scored and blood samples collected every 15 min. Fifteen minutes after discontinuation of the lipid infusion, duodenal biopsies were taken endoscopically. Plasma and mucosal protein levels of CCK were determined by a specific radioimmunoassay. Mucosal mRNA and protein expression of apoA-IV were quantified by real-time PCR and an established enzyme-linked immunosorbent assay, respectively. Results: Duodenal lipid infusion caused an increase in upper abdominal discomfort and nausea in FD patients but not in HV (P=0.001 and 0.033 relative to baseline, respectively). The mean (SD) mucosal CCK level in FD was 3.52 ± 1.11 pmol/mg protein and in HV 5.34 ± 0.79 pmol/mg protein, which was significantly different (P<0.0001). Fasting plasma CCK levels and the stimulation of plasma CCK by duodenal lipid infusion were comparable in FD patients and HV. No significant differences in mucosal apoA-IV mRNA and protein expression between the two groups were found. Conclusion: The lower duodenal CCK concentration suggests excessive release of CCK in FD patients in response to duodenal lipid. This finding increases insight into the mechanism by which fatty foods induce and exacerbate symptoms in FD patients. Our data do not demonstrate involvement of apoA-IV, therefore the underlying cause of elevated peripheral CCK release in FD patients warrants further investigation.