PATIENT BED STATUS In order to fully comply with CMS
advertisement

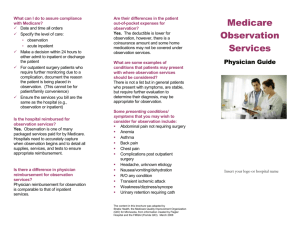
PATIENT BED STATUS In order to fully comply with CMS regulations regarding proper status for bedded patients, admitting physicians need to select the appropriate status from the following list: INPATIENT: Inpatient status should be for medical patients meeting severity and intensity criteria as established by InterQual. In most instances, all ICU admissions are appropriate for inpatient status as are patients after major surgeries with anticipated post-operative stays of greater than 48 hours as well as medical patients with anticipated length of stays based on severity and/or intensity of greater than 48 hours. Documentation of medical necessity for inpatient admission must be provided. OUTPATIENT with OBSERVATION SERVICES: Outpatient with observation services should be used for bedded patients with low acuity and/or low intensity whose length of stay is likely to be less than 48 hours. This category can be used for medical or surgical patients meeting InterQual criteria for outpatient with observation services. This category should not be used for patients who do not have a specific medical justification for this category. Documentation in the medical record should indicate the justification for this category. SAME DAY SURGERY in a BED: This category should be selected for patients who have undergone a surgical or other procedure who are being kept in a bed for routine recovery after an outpatient procedure wherein there is no clear medical indication for them to be bedded (meaning the patient does not meet criteria for outpatient with observation services). This category is for routine recovery after a procedure. OUTPATIENT in a BED: This category should be used for bedded patients who do not meet any of the categories. Patients bedded in this category have no clear medical indication for bedded status, but wherein the admitting physician feels it is in the patient’s best interest to be in a bedded status. This category should be used for patients of low acuity who need an intervention that could be performed in an outpatient setting such as infusion therapy, transfusion therapy, family/social reason, etc. MEDICARE/MEDICAID PATIENTS Outpatient with Observation Services should be written only after a planned surgery/procedure and the medical record must contain physician documentation to support the need for Outpatient with Observation Services. CASE MANAGEMENT PERSONNEL Case management personnel are available 24/7 to answer any questions and/or to assist the admitting physician with choosing the proper bedded status whenever there is a question. To contact case management services: Case Management Contact Numbers Monday – Friday, Evenings, Saturday, Sunday, Holidays: Monday – Friday: 271-4518/271-5260 Saturday: 271-9158 Presbyterian Tower ED Case Manager on site; 271-0354 for TCH ED case manger; and Sunday the Case Manager pager is 647-0051. Any need in the evening or on holidays should go through the page operator for the Case Manager on call. More Patient Status Information Inpatient vs. Outpatient with Observation Services? OU Medical Center uses InterQual criteria in conjunction with Medicare’s Inpatient only Addendum E list and guidelines in reviewing for appropriate patient status. Per HCA Observation Manual - Medicare’s Definition of Observation: Observation care is a well-defined set of specific, clinically appropriate services, which include ongoing short term treatment, assessment, and reassessment before a decision can be made regarding whether patients will require further treatment as hospital inpatients or if they are able to be discharged from the hospital. ___________________________________________________________________ Question: Many times physicians expect their patients to remain in house overnight with discharge the following morning as a part of routine recovery after an outpatient procedure. Can the extended recovery be billed as observation? Answer: If the usual recovery for a specific procedure were for a patient to remain in-house overnight, then that would be your “standard recovery period” for that procedure. It would not be appropriate to charge for observation or inpatient services in this scenario. Question: Can Observation Services be charged with surgical procedures, diagnostic testing, chemotherapy administration, blood transfusions, endoscopic procedures or cardiac catheterizations? Answer: Observation Services should not be charged for patients who are assigned to a routine care bed unit for standard recovery or monitoring following a surgical or diagnostic procedure _______________________________________________________________________________ In summary, if a patient needs to be in a bed overnight, then in order to charge Observation Services there must be documentation as to why the patient needs the extended recovery (i.e., spike in blood pressure not resolved in standard recovery, etc) Otherwise, “Same Day surgery in a Bed” is usually the best choice. Examples: Here is a Good Example of appropriate use of the category “Outpatient with Observation Services” after a planned surgery: Patient admitted as Same Day Surgery for a planned Laparotomy with Bilateral Salpingooopherectomy. Post operatively, the patient goes to PACU and then to Phase II recovery where she has a documented spike in blood pressure requiring IV medication. The patient’s blood pressure remains elevated above baseline. It is then appropriate for the physician to order, “Admit as Outpatient with Observation Services”. The admitting physician should then document something to the effect, “Patient’s blood pressure spiked in recovery requiring IV medication. Need to continue monitoring blood pressure for next 24 hours.” This would qualify for “Outpatient Observation” However, if this same patient had no problems with blood pressure and her recovery was uneventful, but the physician wanted to monitor overnight because of concerns about home care and/or late surgery and did not want to send home at night (or any similar action for patient convenience) This would qualify for “Same Day Surgery in a Bed”