UTMJ Imaging Case Presentation - University of Toronto Medical
advertisement

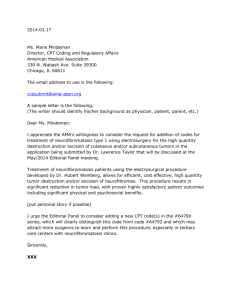
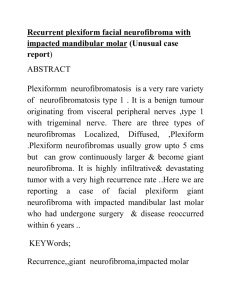
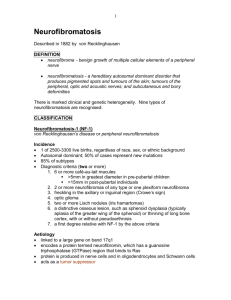
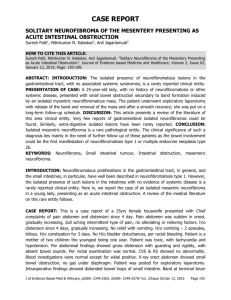
UTMJ Imaging Case Presentation Skeletal Manifestations of Neurofibromatosis Type 1 Vincent R Spano1, BMSc(H), Robert R Bleakney2, MD 1 2 University of Toronto, Faculty of Medicine, MD Candidate 2012* Department of Medical Imaging, Mount Sinai Hospital and University Health Network, University of Toronto, Toronto, Ontario, Canada Corresponding author: Vincent R. Spano, BMSc(H) University of Toronto MD Candidate 2012 vincent.spano@mail.utoronto.ca PART 1 – The Case A 41 year-old man presents with a diffuse soft tissue mass extending throughout his left arm, resulting in marked disfigurement and decreased functionality. This mass has been present since adolescence, however he is concerned about its progressive increase in size over the past several years. He also complains of intermittent, throbbing pain in his left arm and numbness in the median nerve distribution of his left hand. On physical exam, he appears short in stature with mild macrocephaly. A thorough dermatologic examination reveals axillary freckling and several pigmented macules on the back, trunk and limbs measuring 1-2 cm in diameter. Small soft-tissue lesions are found above and below the skin, the majority of which are concentrated on the trunk. A diffuse, tender mass extends throughout the anterior aspect of his left arm with a firm, “rubbery” consistency. His blood pressure is moderately elevated at 138/90 mm/Hg, although the remainder of his cardiovascular exam is normal. The rest of his neurological exam and recent blood work are unremarkable. The patient is sent for plain film radiographs of his left forearm, shown in Figure 1 below. Figure 1.A Figure 1.B Q. What is the diagnosis? a) Proteus Syndrome b) McCune-Albright syndrome c) Schwannomatosis d) von Recklinghausen disease e) Milroy’s disease Answer: d) von Recklinghausen disease (Neurofibromatosis Type 1) PART 2 Background and Clinical Features Neurofibromatosis type 1 and type 2 are genetic disorders involving autosomal dominant mutations. These conditions result in an increased frequency of developing both benign and malignant tumours.1 Neurofibromatosis 1 (NF1), also known as von Recklinghausen disease, is associated with a defect in the NF1 gene, a tumour suppressor gene on chromosome 17 responsible for the production of neurofibromin.1 Neurofibromin inhibits the activity of the p21 ras protein within cells, and is important in downregulating signal transduction and cell proliferation or differentiation.2 Neurofibromatosis 2 (NF2), on the other hand, is a distinct condition resulting from a mutation in the NF2 tumour suppressor gene on chromosome 22, which interferes with the production of a regulatory protein in nervous tissue known as merlin.1 The prevalence of Neurofibromatosis type 1 as a disease is approximately 1 in 3500 people, and is usually diagnosed clinically.3 Approximately 50% of all cases are familial, with the remainder due to sporadic mutations.4 Despite nearly 100% penetrance by the time the patient reaches adulthood, there is extreme variability in expression, resulting in a wide range of clinical presentations.4 The most common findings are Lisch nodules, café-au-lait spots, axillary or inguinal (skinfold) freckling, and neurofibromas (see Table 1 for NIH Diagnostic Criteria5). These are frequently accompanied by skeletal abnormalities, learning disabilities, vision loss, and renovascular hypertension.1,6 In contrast, NF2 is primarily associated with schwannomas, not neurofibromas. Peripheral tumours are much less common, and cutaneous manifestations are less prominent. Bilateral vestibular schwannomas, juvenile posterior subcapsular lenticular opacities, meningiomas and gliomas are some of the more common features in NF2. 1 Neurofibromas are tumours arising from the Schwann cells that surround peripheral nerves, and can occur in several forms.6 Cutaneous and subcutaneous neurofibromas are typically benign and are often present in large numbers. Nodular or diffuse plexiform neurofibromas, however, can grow to remarkable sizes and are at risk of undergoing transformation to malignant peripheral nerve sheath tumours (MPNST).6 Depending on their size and location, plexiform neurofibromas may result in severe disfigurement and morbidity through pain, nerve compression, loss of functionality, and even polyneuropathy. In addition to MPNSTs, other tumours commonly associated with NF1 include optic pathway gliomas and pheochromocytomas, leading to potential loss of visual acuity and uncontrolled hypertension, respectively. 3 Musculoskeletal abnormalities are important manifestations of NF1 and are the main focus of the images in this case presentation. Although the pathophysiology is not well understood, it has been shown that NF1 patients have decreased bone mineral density and Vitamin D deficiency, in addition to pronounced accumulation of osteiod and high bone turnover rates.7 10-30% of patients have a disorder of the spine, with scoliosis being the most common osseous manifestation in the NF1 patient population.3 This frequently presents between 6 and 10 years of age, and is sometimes accompanied by a debilitating kyphosis. Congenital dysplasia of the tibia with antero-lateral bowing and pseudoarthrosis is seen in approximately 5% of patients, and is usually evident within the first year of life.6,8 Short stature, thinning of the cortex, cystic bone lesions, sphenoid wing dysplasia, macrocephaly, and generalized osteoporosis are also characteristic findings.6 Other musculoskeletal changes in NF1 patients may result from unilateral segmental hypertrophy, most commonly involving the lower extremities or the head and neck.3 This causes marked abnormalities in bone growth, particularly in association with overlying soft tissue changes such as hemangiomas, plexiform neurofibromas or elephantiasis. These changes manifest as elongated, gracile bones with thickened, wavy irregularities of the cortex on imaging, and can easily be appreciated on plain film radiographs as shown in Figure 1.3 Imaging Studies Plain film radiographs of the spine, skull, chest, and extremities are often helpful in confirming the diagnosis of NF1 and in monitoring the progression of skeletal dysplasia. Figure 1A and 1B are AP and lateral x-rays of the patient’s left forearm, respectively. Large soft-tissue masses can be seen projecting anteriorly, representing extensive plexiform neurofibromas. The bones are generally osteopenic and dysplastic. They are thin and gracile with extrinsic cortical erosion from adjacent soft tissue neurofibromas. Supplemental images further demonstrate these findings in the left humerus and olecranon (Figures 2 and 3, respectively). Scoliosis, pseudoarthrosis, anterolateral bowing of the tibia, and the multitude of other skeletal manifestations can be reliably detected on plain film radiographs, making imaging a valuable tool in the diagnostic work-up and evaluation of disease severity. Magnetic resonance imaging (MRI) in neurofibromatosis type 1 may reveal optic nerve thickening and areas of increased T2-weighted signal in the brain, commonly referred to as “Unidentified bright obects (UBO’s)”. These UBO’s are of unknown clinical significance and often disappear with age. 9 Despite the presence of these abnormalities, routine examination with MRI is often controversial, as it has not been shown to have any effect on clinical management.6 MRI may also be useful in monitoring the growth of plexiform neurofibromas, investigating neuropathology, and for preoperative planning. Management A thorough physical examination and detailed family history are paramount in the early diagnosis of neurofibromatosis type 1.1 Yearly ophthalmologic exams and routine developmental assessments are important during childhood, as is close monitoring of blood-pressure in adults. Although there is no cure, the role of surgery in treating NF1 is extensive. Tumours are often resected, particularly in the case of disfiguring plexiform neurofibromas. However, these operations are often unsuccessful due to extensive involvement of nervous tissue and the tendency for these lesions to grow back. Congential tibial dysplasia is frequently managed with bracing, bone grafts, compression or distraction histiogenesis, or even amputation in severe cases.3 Adjuvant chemotherapy is sometimes warranted for progressive tumours, while medical management is required for hypertension and learning or behavioural disorders. Lastly, counseling patients and family members on psychosocial adjustment, genetics, complications and prognosis is essential, and should be offered to all patients, particularly during childhood.1,6 The patient in this case presentation had very little clinical or radiological follow-up since the diagnosis of NF1 was made during his childhood. He did, however, have previous surgery on his spine to correct his scoliosis as a young adult. Since presenting with rapidly increasing disfigurement of his left arm at the age of 41, multiple debulking operations of his plexiform neurofibromas have been performed in a stage-like fashion. This was accompanied by median nerve decompression in order to relieve the intermittent parasthesia in his left hand caused by the extensive mass. His hypertension is being successfully managed with amlodipine, and he has undergone MRI scans of the brain and abdomen to rule out optic gliomas and pheochromocytomas, respectively. He now has routine follow-up with a multidisciplinary team involving neurosurgery, plastic surgery, and neurology in order to ensure appropriate management. Discussion Although several individual features of NF1 are present in other genetic disorders, the overall characteristic presentation is fairly distinct. However, without a thorough history and known presence of NF1 in immediate family members, several syndromes must be considered in the differential diagnosis. For example, tissue overgrowth resembling neurofibromas is consistent with both Proteus syndrome and schwannomatosis, however the presence of café au lait spots, axillary freckling, and other cutaneous manifestations in this patient makes these diagnoses unlikely.6 In this particular case, Milroy’s disease may also be considered due to the extensive unilateral enlargement of his left arm. Similarly, the presence of the characteristic cutaneous and musculoskeletal manifestations suggests otherwise. Legius syndrome is often high on the differential for NF1, as it is associated with café-au-lait spots, macrocephaly, and axillary freckling.6 However, the striking soft tissue masses resulting from neurofibromas and features of skeletal dysplasia are not characteristically involved, ultimately leading one to consider an alternative diagnosis. Despite the café-au-lait spots seen in McCune-Albright syndrome, it can also be ruled out in a similar fashion. As exemplified in this case, imaging studies revealing characteristic skeletal manifestations can aid significantly in making the diagnosis of NF1 in a patient with soft tissue masses and typical cutaneous involvement. Confirmation of the diagnosis can ultimately be determined through genetic testing for mutations in the NF1 gene.6 This case highlights the important clinical signs and symptoms of neurofibromatosis type 1, and illustrates the common musculoskeletal changes associated with this disease. The patient described above fulfills the diagnostic criteria for NF1, and exemplifies the morbidity and disfigurement that can result. The propensity for developing malignant tumours warrants close patient follow-up and a multidisciplinary approach to management. A thorough understanding of the signs, symptoms and pathophysiology of this complex condition is required in order for a team of physicians from various medical and surgical disciplines to execute an effective treatment plan. Depending on the age of the patient and severity of disease, this may commonly include specialists from pediatrics, orthopedic surgery, plastic surgery, neurosurgery, oncology and neurology. References 1. Gutmann DH, Aylsworth A, Carey JC, Korf B, Marks J, Pyeritz RE, Rubenstein A, Viskochil D. The diagnostic evaluation and multidisciplinary management of neurofibromatosis 1 and neurofibromatosis 2. JAMA. 1997 Jul 2;278(1):51-7. 2. Oguzkan S, Terzi YK, Cinbis M, Anlar B, Aysun S, Ayter S. Molecular genetic analyses in neurofibromatosis type 1 patients with tumours. Cancer Genet Cytogenet. 2006 Mar;165(2):16771. 3. Crawford AH, Schorry EK. Neurofibromatosis update. J Pediatr Orthop. 2006 MayJun;26(3):413-23. 4. Rasmussen SA, Friedman JM. NF1 gene and neurofibromatosis 1. Am J Epidemiol. 2000 Jan 1;151(1):33-40. 5. National Institutes of Health Consensus Development Conference. Neurofibromatosis: Conference statement. Arch Neurol 1988;45:575-578. 6. Jett K, Friedman JM. Clinical and genetic aspects of neurofibromatosis 1. Genet Med. 2010 Jan;12(1):1-11. 7. Seitz S, Schnabel C, Busse B. Schmidt HU, Beil FT, Friedrich RE, Schinke T. Mautner VF, Amling M. High bone turnover and accumulation of osteoid in patients with neurofibromatosis 1. Osteoporos Int 2010;21:119-127. 8. Stevenson DA, Birch PH, Friedman JM, Descriptive analysis of tibial pseudoarthosis in patients with neurofibromatosis 1. M J Med Genet 1999;84:413. 9. Van Es S, North KN, McHugh K, De Silva M. MRI findings in children with neurofibromatosis type 1: a prospective study. Pediatr Radiol 1996; 26:478. Table 1. Diagnostic criteria for Neurofibromatosis Type 1* The diagnostic criteria for NF-1 are met if two or more of the following are found: 1. Six or more café au lait macules over 5 mm in greatest diameter in prepubertal individuals and over 15mm in greatest diameter in postpubertal individuals 2. Two or more neurofibromas of any type or one plexiform neurofibroma 3. Freckling in the axillary or inguinal regions 4. Optic glioma 5. Two or more Lisch nodules (iris hamartomas) 6. A distinctive osseous lesion such as sphenoid dysplasia or thinning of long bone cortex, with or without pseudoarthrosis 7. A first degree relative (parent, sibling, or offspring) with NF1 by the above criteria *from the National Institutes of Health Consensus Development Conference5 Supplemental images: Figure 2 Figure 3 Figure 1. AP (1A) and lateral (1B) plain film radiographs of the left forearm in a patient with neurofibromatosis type 1. Extensive soft-tissue masses are seen projecting anteriorly, representing extensive plexiform neurofibromas. The bones are generally osteopenic and dysplastic, and appear thin and gracile with extrinsic cortical erosion from the adjacent soft tissue neurofibromas. Figure 2. A plain film radiograph of the left shoulder and arm in a patient with neurofibromatosis type 1. The thin, gracile appearance of the humerus illustrates some of the features of skeletal dysplasia seen with this condition. Extrinsic cortical erosion from adjacent soft tissue neurofibromas can also be seen. Figure 3. A plain film radiograph of the left olecranon in a patient with neurofibromatosis type 1. Generalized osteopenia and multiple large extrinsic cortical erosions can be seen resulting from adjacent soft tissue neurofibromas.