Patient Education:
Laryngectomy
Laryngectomy Patient Education 1
Appointments
Doctor:_____________________
Doctor:_____________________
Date:_________ Time:________
Date:_________ Time:________
Location:___________________
Location:___________________
___________________________
___________________________
Phone:_____________________
Phone:_____________________
Doctor:_____________________
Doctor:_____________________
Date:_________ Time:________
Date:_________ Time:________
Location:___________________
Location:___________________
___________________________
___________________________
Phone:_____________________
Phone:_____________________
Doctor:_____________________
Doctor:_____________________
Date:_________ Time:________
Date:_________ Time:________
Location:___________________
Location:___________________
___________________________
___________________________
Phone:_____________________
Phone:_____________________
Doctor:_____________________
Doctor:_____________________
Date:_________ Time:________
Date:_________ Time:________
Location:___________________
Location:___________________
___________________________
___________________________
Phone:_____________________
Phone:_____________________
Laryngectomy Patient Education 2
Medication Record
Medication
Dose
Frequency
Start Date
Stop Date
____________________
_________
____________
____/____/____
____/____/____
____________________
_________
____________
____/____/____
____/____/____
____________________
_________
____________
____/____/____
____/____/____
____________________
_________
____________
____/____/____
____/____/____
____________________
_________
____________
____/____/____
____/____/____
____________________
_________
____________
____/____/____
____/____/____
____________________
_________
____________
____/____/____
____/____/____
____________________
_________
____________
____/____/____
____/____/____
____________________
_________
____________
____/____/____
____/____/____
____________________
_________
____________
____/____/____
____/____/____
____________________
_________
____________
____/____/____
____/____/____
____________________
_________
____________
____/____/____
____/____/____
____________________
_________
____________
____/____/____
____/____/____
____________________
_________
____________
____/____/____
____/____/____
____________________
_________
____________
____/____/____
____/____/____
____________________
_________
____________
____/____/____
____/____/____
____________________
_________
____________
____/____/____
____/____/____
____________________
_________
____________
____/____/____
____/____/____
____________________
_________
____________
____/____/____
____/____/____
Laryngectomy Patient Education 3
Health Professionals:
I am a laryngectomee (no vocal cords). I am a total neck breather. I speak via a voice
prosthesis. In the event that I stop breathing, expose my entire neck. Keep my neck opening clear and
protected from liquids. Resuscitate with air or oxygen to neck opening, or use mouth-to-neck
breathing.
Personal Information
Telephone Numbers
Name:___________________________________
Home:_________________________________
Address:_________________________________
Cell:___________________________________
________________________________________
Work:__________________________________
________________________________________
Other:__________________________________
Date of Birth: _____/______/______
Emergency Contact 1
Telephone Numbers
Name:___________________________________
Home:_________________________________
Address:_________________________________
Cell:___________________________________
________________________________________
Work:__________________________________
________________________________________
Other:__________________________________
Emergency Contact 2
Telephone Numbers
Name:____________________________________
Home:_________________________________
Address:__________________________________
Cell:___________________________________
_________________________________________
Work:__________________________________
_________________________________________
Other:__________________________________
Primary Physician
Head and Neck Surgeon
Name:___________________________________
Name:___________________________________
Address:_________________________________
Address:_________________________________
Phone Number:____________________________
Phone Number:____________________________
Preferred Local Hospital:_________________________________________________
Medical Insurance Carrier
Name:_______________________________________________ Phone Number:_______________________
Medic-Alert ID Number:___________________________________________________
Medications
___________________________________________ ___________________________________________
___________________________________________
___________________________________________
___________________________________________
___________________________________________
Laryngectomy Patient Education 4
Contents:
Pages
6-8
Laryngectomy Timeline
9-12
Glossary
13
Parts of the Mouth
14
Parts of the Throat and Neck
15-16
Laryngectomy
17-18
Radical Neck Dissection
19-20
General Information for the Laryngectomee
21
Incision Care
22
Stoma Care
23-24
Suctioning
25-26
Reinsertion of Laryngectomy Tube
27
Mouth and Skin Care
28
Checking Residual
29
Flushing Your Feeding Tube
30
Tube Feeding
31
Medication Administration
Support Groups and Resources
Laryngectomy Patient Education 5
Laryngectomy Timeline
Pre-Operation
1st Visit with:
An Ear, Nose, Throat (ENT) physician
Cancer Care Coordinator (this person will set-up diagnostic tests)
2nd Visit with:
ENT Physician’s Assistant (PA)
Anesthesia
Speech Therapy
Cancer Care Coordinator
Other physicians
Operation
Pre-Operation preparations:
The anesthesiologist will talk with you about anesthesia
Your vital signs (blood pressure, pulse, respirations, temperature,
oxygen saturation) will be taken
An intravenous (IV) catheter will be inserted in your vein (usually the
hand or arm) for fluid and medication administration before, during,
and after surgery
Blood may be drawn before surgery
Length of Operation:
Approximately 8 hours
Recovery Room:
You will be in the recovery room for approximately 4 hours.
During your recovery room stay, your vital signs and pain level will
be monitored.
When you are determined stable, you may be transferred to the
Intensive Care Unit (ICU).
Laryngectomy Patient Education 6
Post-Operation
Intensive Care Unit (ICU):
You will be carefully monitored in the ICU for at least one day (longer
for complicated cases) after surgery to make sure your body
tolerated surgery
When your are determined to be stable, you will be transferred to a
medical/surgical nursing floor
Medical/Surgical Nursing Floor:
Upon arrival to the medical surgical floor, your nurse will teach you
how to:
o Care for your laryngectomy and incisions
o Suction your laryngectomy stoma
o Feed and give medications through your feeding tube (if
applicable)
o Reinsert the laryngectomy tube if it becomes dislodged
You and your family will be expected to demonstrate the above skills
by discharge
Discharge:
Approximately 7-9 days after surgery
Nurse will have you sign discharge paperwork
You will be sent home with (including but not limited to):
o Suction equipment from an outside agency
o Obturator for your laryngectomy tube (if applicable)
o An extra laryngectomy tube (if applicable)
o Alkalol spray
o Humidity
Laryngectomy Patient Education 7
Follow-up
1st Visit:
Approximately 1 week after discharge
Meet with an ENT physician for suture, staple, and nasal gastric
(NG) tube removal. May have swallow test.
Esophagram to evaluate for possible leak
Make arrangements for meeting with radiation oncologist, if
indicated. Radiation treatment should begin within 6 weeks of
surgery.
2nd Visit:
Approximately one month after surgery
Meet with the ENT physician
Set-up appointment or meet with the Speech Therapist
Long-term Follow-up Care
Evaluation by your ENT staff surgeon on a regular schedule for
cancer surveillance
o Years 1-2: Every 6-8 weeks
o Year 3: Every 3 months
o Year 4: Every 4 months
o Year 5: Every year
If you would like more information or have questions, please contact The University
of Kansas Department of Otolaryngology Head and Neck Surgery at (913) 588-6701.
Laryngectomy Patient Education 8
Glossary
Anesthesia: Medication used to produce a loss of sensation or feeling.
Anesthesiologist: A medical doctor that administers anesthesia.
Cancer: Abnormal cells that multiply without control. They can spread through
the bloodstream and the lymphatic system to other parts of the body.
Carcinoma: Cancer that begins in the lining or covering of an organ.
Cartilage: Firm, rubbery tissue that cushions bones at joints.
Chemotherapy: Anticancer drugs used to treat cancer.
Clinical Trials: Studies of new cancer treatments. Results from clinical trials
determine future cancer treatments.
Electrolarynx: A battery operated instrument that makes a humming sound to
help laryngectomees talk.
Epiglottis: The flap that covers the trachea during swallowing so that food
does not enter the lungs.
Esophageal Speech: Speech produced with air trapped in the esophagus and
forced out again.
Esophagus: The tube through which food passes from the throat to the
stomach.
Glottis: The middle part of the larynx where the vocal cords are located.
Humidifier: A machine that puts moisture in the air.
Laryngectomy Patient Education 9
Laryngectomee: A person who has their voice box removed.
Laryngectomy: An operation to remove all or part of the larynx.
Larynx: An organ in the throat used in breathing, swallowing, and talking. It is
made of cartilage and muscle and is lined by a mucous membrane similar to
the lining of the mouth. It is also called the voicebox. The larynx has three
parts: the supraglottis, the glottis, and the subglottis.
Lymph Nodes: Small, bean-shaped organs located along the lymphatic
system. Nodes filter bacteria or cancer cells from the lymph fluid.
Malignant: Cancer that has the ability to spread to other parts of the body.
Metastasis: Cancer cells that spread to other parts of the body. These cells
have the same appearance or characteristics of original tumor or mass.
Neck Breather: A term used for a person who has had a laryngectomy. The
laryngectomee breathes from the neck because the trachea is diverted from
the mouth and nose to the neck.
Obturator: A device with a curved tip used in the insertion, or reinsertion, of a
laryngectomy or tracheostomy tube.
Oncologist: A doctor who specializes in the treatment of cancer.
Otolaryngologist: A doctor who specializes in the treatment of diseases of the
ear, nose and throat. Also known as an ENT or Head and Neck surgeon.
Pathologist: A doctor who identifies diseases by studying cells and tissues
under a microscope.
Pneumatic Larynx: A device that uses air to produce sound to help a
laryngectomee talk.
Laryngectomy Patient Education 10
Prognosis: The probable outcome or course of a disease; the chance of
recovery.
Radiation Therapy: Treatment of cancer cells with high energy beams from xrays or other sources to kill these cells.
Remission: Disappearance of the sign and symptoms of cancer; can be
temporary or permanent.
Risk Factors: Something that increases a person’s chance of getting a
particular type of cancer.
Speech Pathologist: A specialist who evaluates and treats people with
communication and swallowing problems.
Staging: Doing exams and tests to learn the extent of the cancer; whether it
has spread to any other areas of the body.
Stoma: The opening into the windpipe made by the surgeon. Laryngectomees
breathe through this opening.
Subglottis: The lowest part of the larynx, just below the vocal cords down to
the top of the trachea.
Supraglottis: The upper part of the larynx, above the vocal cords; including
the epiglottis.
Systemic Therapy: Therapy that reaches and affects cells all over the body.
Trachea: The airway that connects the larynx to the lungs; the windpipe.
Tracheoesophageal Puncture: A small opening made by the surgeon,
between the esophagus and the trachea. A valve keeps food out of the trachea
but lets air into the esophagus for esophageal speech.
Laryngectomy Patient Education 11
Tracheostomy: Surgery to create an opening in the windpipe.
Tracheostomy Button: A ½ to 1½ inch long plastic tube placed in the stoma
to keep it open.
Tracheostomy Tube: A 2-3 inch long metal or plastic tube that keeps the
stoma and trachea open.
Tumor: An abnormal mass of tissue.
Vocal Cords: Two small bands of muscle within the larynx that closes to
prevent food from getting into the lungs and they vibrate to produce voice.
If you would like more information or have questions, please contact The University
of Kansas Department of Otolaryngology Head and Neck Surgery at (913) 588-6701.
Laryngectomy Patient Education 12
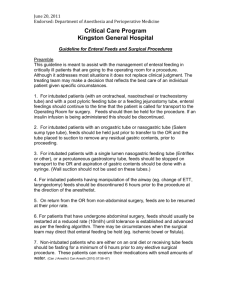
Parts of the Mouth
Your mouth allows you to speak, breathe, and chew. Listed below are specific
parts of the mouth and where they are located.
© 2005 The StayWell Company, 780 Township Line Road, Yardley, PA 19067. All rights
reserved. This information is not intended as a substitute for professional medical care.
Always follow your health care provider's instructions.
Laryngectomy Patient Education 13
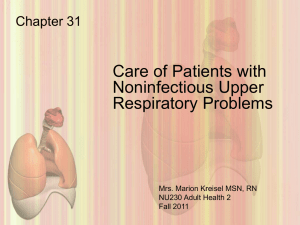
Parts of the Throat and Neck
Your throat allows you to swallow, breathe, and speak. Parts of the neck help
you fight infection. Listed below are specific parts of the throat and neck and
where they are located.
© 2005 The StayWell Company, 780 Township Line Road, Yardley, PA 19067. All rights
reserved. This information is not intended as a substitute for professional medical care.
Always follow your health care provider's instructions.
Laryngectomy Patient Education 14
Laryngectomy
A laryngectomy is an operation to remove the larynx. The larynx, or voice box,
is the organ that produces the sound that allows us to speak. It also prevents
food from entering the air passage.
Who is a candidate for the procedure?
A person with cancer of the larynx is a candidate for this procedure.
How is the procedure performed?
A laryngectomy is done through an incision in the neck. The larynx is removed.
Air can no longer pass from the lungs into the mouth, because the connection
between the mouth and the windpipe no longer exists. So a new opening for
air to enter the lungs must be made in the front of the neck.
The upper portion of the trachea, or windpipe, is brought out to the front of the
neck to create a permanent opening. This opening is called a “stoma.” A
laryngectomy tube may be placed in the stoma to keep it open until it heals.
Often, an operation called a neck dissection is done at the same time as a
laryngectomy. This is done to remove the lymph nodes in the neck, to which
cancer may have spread.
What happens right after the procedure?
After the laryngectomy surgery, the person will be taken to the surgery
recovery room to be watched closely for a short time. Vital signs, blood
pressure, pulse, and breathing will be checked frequently. A small mask with
humidified air will be placed over the stoma. This helps to keep the secretions
thin and prevent blockage of the airway. The head of the bed will be elevated
to promote drainage from the surgical site. Suction drains may have been
placed under the skin to catch any fluid that collects at the incision. The nose,
mouth, and the laryngectomy tube will be suctioned gently.
Laryngectomy Patient Education 15
What happens later?
The person usually spends a few nights in the intensive care unit after a
laryngectomy. Fluids are given through an intravenous line. A stomach tube
may be inserted in the nose into the stomach to supply nutrition until the throat
has healed. You will not be able to eat by mouth for 7-14 days. The total
hospital stay after a laryngectomy is usually about a week.
Before discharge, the person is taught how to care for the stoma. It is very
important that the person and the family understand stoma care. The stoma is
the person's only airway. It must be kept free of fluids, mucus, and anything
else that can block the flow of air. Any blockage of the stoma can be very
serious.
The person will need to learn a new way of speaking. Speech therapy can help
to provide alternative ways of speaking. These alternative ways to speak
include using artificial voice aids, esophageal speech, and voice prosthesis. It
may be helpful to talk with someone who has undergone this procedure. The
International Association of Laryngectomees can help provide support.
What are the potential complications after the procedure?
Surgery carries the risk of bleeding, infection, wound healing problems
including a salivary fistula (an opening into the throat), and allergic reactions to
anesthesia. As with any major surgery, there is a slight risk of heart attack,
stroke, or death. Keeping the new airway open is essential to prevent airway
complications.
If you would like more information or have questions, please contact The University
of Kansas Department of Otolaryngology Head and Neck Surgery at (913) 588-6701.
Adapted from: Hendrickson, Gail. Laryngectomy. Retrieved from:
http://health.discovery.com/encyclopedias/3208.html
Laryngectomy Patient Education 16
Radical or Modified Radical Neck Dissection
A radical neck dissection is a procedure used to remove cancerous tumors
from one side of the neck or upper airway. Almost all the lymph nodes and
some of the muscles, tissues, veins, and nerves in this area may be removed
as well.
Who is a candidate for the procedure?
A person who has a cancerous tumor in the lymph nodes in the neck and
upper airway is a candidate for this procedure.
How is the procedure performed?
The procedure is done under general anesthesia. This means that the person
will be put to sleep with medications. An incision, or cut, is made under the
chin towards the ear. Another incision is made down to the bottom of the neck.
A third incision is made down the middle of the neck. Other incisions may also
be made so the surgeon has a full view of the structures inside the neck. The
skin is then spread open and the tissues underneath the skin are pulled away
from the skin. The surgeon then removes the lymph glands from the neck and
oral cavity.
In addition to the lymph nodes, there are three main structures that may be
removed from the neck area if they are involved by cancer. These are: the
internal jugular vein, the accessory nerve, and the sternocleidomastoid muscle.
Any other veins, nerves, or muscles that are involved with the cancer are also
removed. If the cancer has spread, it may be necessary to remove sections of
the jaw, tongue, or voice box. At times, it is also necessary to perform a
tracheostomy. A tracheostomy is a surgically created opening through the neck
into the trachea, or windpipe. The incision is closed with sutures, staples, or
skin clips.
Laryngectomy Patient Education 17
What happens right after the procedure?
Usually after a radical neck dissection, a person will be in the surgery recovery
room for a few hours for close monitoring. Oxygen will be given through a
facemask or nasal prongs. Pain medication will be given as needed. A person
cannot eat or drink anything at first. Then later in the day, the person can start
taking small sips of fluid. There may be a few tubes that are left near the
incision to drain fluids and blood. These tubes will be removed once the
draining stops.
For the next few days the person will be encouraged to do deep breathing.
This helps to clear the lungs and prevent pneumonia. The day after surgery the
person will be encouraged to get out of bed and walk around. This helps to
lower the risk of blood clots.
If a tracheostomy was done, the person (and family members) will be given
special training in caring for the tracheostomy site.
What happens later at home?
The person will be in the hospital from 4 to 14 days depending if other
operations have also been performed with the neck dissection. Activity at
home will be based on how the person is recovering. Usually a small amount
of activity is recommended on the first day or two after getting home. The
person can increase the activity level if he or she feels ready. Sutures, staples,
or clips are usually taken out 7 to 10 days after surgery. A person is advised
not to drive or participate in strenuous activity for several weeks.
What are the potential complications after the procedure?
After a radical neck dissection a person may have bleeding at the surgery site,
infection, pain, and scarring. There is also a chance for injury to the veins and
nerves in the neck. This can cause bleeding or numbness. This procedure may
also cause a deformity of the neck and face.
If you would like more information or have questions, please contact The University
of Kansas Department of Otolaryngology Head and Neck Surgery at (913) 588-6701.
Adapted from: McLaughlin, Eileen. Radical Neck Dissection. Retrieved from:
http://health.discovery.com/encyclopedias/3212.html
Laryngectomy Patient Education 18
Patient Education:
General Information for the Laryngectomee
Activities of Daily Living:
Plan regular rest periods during the day.
Exercise lightly as tolerated, such as walking. Increase your level of
exercise on a daily basis but not to the point of exhaustion or pain.
Maintain your diet as ordered by your physician. Food will taste dull and
it will have no odor, however, you must eat and keep your weight up in
order to heal and get well.
Drink plenty of fluid; at least 8-10 glasses of water a day. Drinking the
recommend amount of fluids will decrease your chance of getting
constipated.
You may drink any other fluids in addition as long as they do not contain
alcohol. Alcohol will dehydrate your body.
You may shower 24 hours after your drains have been removed.
When showering, you will need to cover your stoma/incision with a shield
or cover with your hand. Avoid getting soap lather in your stoma
because it will make you cough. Pat area dry with towel.
Shave with an electric razor or safety razor.
Laryngectomy Patient Education 19
Communication:
Wear a medical alert bracelet that says “Neck Breather”.
Notify your physician of the following conditions:
o Severe pain and swelling, redness or drainage from the incision
area.
o Prolonged fever of 101.5 degrees Fahrenheit for over 24 hours.
o Persistent cough
o Respiratory distress, difficulty breathing, or a feeling of being short
of breath.
Contact 911 or your local EMS when you have trouble removing dried or
thick secretions from your stoma or difficulty breathing from your stoma.
Other:
Avoid smoking or being in the room where others are smoking. The
smoke fume may irritate your throat and will induce coughing.
Avoid persons with respiratory tract infections, especially colds. You will
be more susceptible to these infections for the first several months after
surgery.
Contact the doctor’s office if you have any questions at (913) 588-6700.
To contact one of our hospital ENT nurses, please call (913) 588-9350.
Laryngectomy Patient Education 20
Patient Education:
Incision Care
Wash your hands with soap and water.
Pour equal amounts of hydrogen peroxide and water in a cup.
Dip one swab into the hydrogen peroxide mixture. Clean around stoma
and incision. Do this one swab at a time and
remove any dried crust or mucus.
Rinse off any hydrogen peroxide mixture with a
swab or gauze that is dipped in plain water.
Gently dry your skin with a dry cloth.
Apply a thin layer of triple antibiotic ointment to
stoma and incision with a cotton swab for the
first 10 days after surgery (if ordered by your
physician).
Source: http://devweb3.vip.
ohio-state.edu/patedu.htm
ate.edu/patedu.htm
Clean stoma and incision 2 times a day and as
needed until healed.
Look at your incision. If it is red or hurts, repeat stoma care more than 2
times a day.
Wash your hands with soap and water.
If you would like more information or have questions, please contact The University
of Kansas Department of Otolaryngology Head and Neck Surgery at (913) 588-6701.
Adapted from: Ohio State University Medical Center. Laryngectomy Stoma Care. Retrieved from:
http://devweb3.vip.ohio-state.edu/patedu.htm
Laryngectomy Patient Education 21
Patient Education:
Stoma Care
Spray the stoma with alkalol spray (diluted one part alkalol to two parts of
water) every 1-2 hours while awake. This will help keep the secretions
moist and prevent crusts from forming. It will also make it easier for you to
cough the secretions out. The diluting water may be plain tap water.
Remove dried secretions from stoma with tweezers as needed. You may
need to use alkalol to loosen the crust.
Blood specks in the sputum occur in the
winter. Increased moisture helps prevent
crusting and subsequent blood specks.
It is important that you cover the stoma
when you cough. Your secretions are now
coming from your stoma instead of your
mouth.
Source: http://devweb3.vip.ohio-state.edu/patedu.htm
Keep you stoma covered at all times with either the stoma cover or other
collars of your choice. This will keep dirt and debris out of your stoma.
This will also help you keep from coughing in an embarrassing manner.
You may want to wear clothing with high necklines or scarves so that the
area is covered and looks attractive during cold weather when the air is
dry, you will need to place extra covering over your stoma so that the air
will condense on the cover and freeze.
If you would like more information or have questions, please contact The University
of Kansas Department of Otolaryngology Head and Neck Surgery at (913) 588-6701.
Adapted from: Ohio State University Medical Center. Laryngectomy Stoma Care. Retrieved from:
http://devweb3.vip.ohio-state.edu/patedu.htm
Laryngectomy Patient Education 22
Patient Education:
Suctioning
Suctioning keeps your stoma clear of excess mucus
Suction when unable to clear your secretions or you are having trouble
breathing.
Suctioning Procedure:
1. Collect your supplies
Suction machine
Catheter
Small bowl of distilled water
Disposable powder-free gloves
2. Wash your hands with soap and warm water. Then put on clean,
disposable, powder-free gloves.
3. Prepare to suction
Turn the suction machine
to 80-120 mmHg
Attach the suction
catheter to the suction
machine. Dip the catheter
tip into the distilled water
to assure the suction is
working.
Do the following if your
secretions are thick: Spray
small amount of alkalol, 23 times in your stoma as
you inhale. This will help
loosen mucus.
Source: http://devweb3.vip.ohio-state.edu/patedu.htm
Laryngectomy Patient Education 23
Patient Education:
Suctioning (continued)
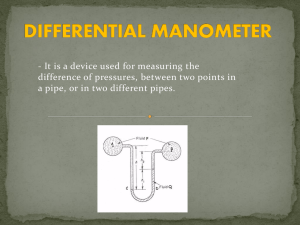
4. Insert the Catheter
Take a few deep breaths
to fill your lungs with
oxygen.
Gently insert the catheter
into your tracheotomy
tube. While you insert the
catheter, do not suction.
Stop inserting the catheter
when you start to cough
or meet resistance
(usually 3-4 inches).
5. Suction
Apply suction by intermittently
covering the suction hole with
your thumb. At this time,
slowly pull the catheter out of
your trach tube. Move the
catheter tip in a circle as you pull Source: http://www.cpem.org/gif/55.gif
the catheter out.
The catheter should be out of
your stoma within 5-10 seconds.
If you need to suction more, relax and breathe before you start
again. Repeat suctioning process until airway is clear.
Discard the catheter, water and gloves. Rinse the suction
connecting tube with water until it is clear of mucus.
Turn off the suction machine. Wash your hands.
If you would like more information or have questions, please contact The University
of Kansas Department of Otolaryngology Head and Neck Surgery at (913) 588-6701.
Adapted from: Ohio State University Medical Center. Laryngectomy Suctioning. Retrieved
from: http://devweb3.vip.ohio-state.edu/patedu.htm
Laryngectomy Patient Education 24
Patient Education:
Reinsertion of Tracheostomy Tube
1. Remain calm. Call 911.
2. Remove the inner cannula.
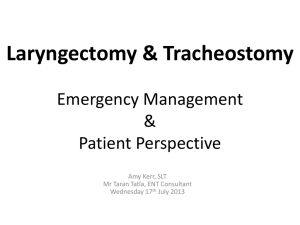
3. Insert the obturator into the
laryngectomy tube. You will know the
obturator is in place when you see the
round tip protrude out of the cannula.
Outer Cannula
Obturator
4. Hold the obturator in place with your thumb
and grasp the outer cannula under the
faceplate with the index and middle fingers,
and insert the new tube following the track
of the dislodged tube.
Stoma
5. Guide tube into trachea, gently with tip
toward your toes. If you have difficulty
inserting the cannula, lift your chin up to
better align the stoma with the hole in the
trachea.
Laryngectomy Patient Education 25
Patient Education:
Reinsertion of Laryngectomy Tube (Continued)
6. Immediately remove the obturator.
7. Reinsert the inner cannula to reestablish the
airway.
Inner
Cannula
8. Secure the tube with ties.
9. If you are unable to reinsert the laryngectomy tube, try inserting suction
catheter to maintain some airway and keep incision open until expert
help arrives.
If you would like more information or have questions, please contact The University
of Kansas Department of Otolaryngology Head and Neck Surgery at (913) 588-6701.
Source: Ohio State University. Reinsertion of a Tracheostomy Tube. Retrieved from: http://devweb3.vip.ohiostate.edu/Materials/PDFDocs/procedure/tube-care/trach/reinsert.pdf.
Laryngectomy Patient Education 26
Patient Education:
Mouth and Skin Care
You need to keep the skin around the feeding tube dry and clean. This helps
prevent soreness and infection. The mouth also needs to be cleansed, even
though food isn’t taken through it.
Caring for the Mouth
To keep the mouth clean, follow these steps:
1. Brush the teeth or dentures at least twice daily with
a soft toothbrush.
2. If you have dentures, remove your dentures and
wipe the inside of the mouth with a damp
washcloth.
3. Apply a lip balm to keep the lips moist.
Cleaning the Skin and Under the Bolster
Gently wash the skin around the feeding tube each day. Follow these steps:
1.
2.
3.
Wash your hands.
Wet a soft cloth or gauze with warm, soapy water.
Gently wipe the skin around the feeding tube. Also
wipe the bolster and the base of the feeding tube.
4. Gently lift the bolster just enough to get the cloth or
gauze under it. Be careful not to pull on the feeding
tube.
5. Check for redness, swelling, bleeding, or leakage around the opening.
6. Clean under the bolster with the soapy cloth or gauze.
7. Rinse well with clear, warm water. (This can be done in the shower.)
8. Pat dry with a soft cloth.
9. Apply a protective skin barrier or antibacterial ointment if your health care
provider tells you to.
10. Gently push the bolster back against the skin.
11. Give the feeding tube a gentle 1/4 turn. This helps keep the tube from
sticking to the inside of the stomach.
12. Wash your hands.
Bolster
If you would like more information or have questions, please contact The University
of Kansas Department of Otolaryngology Head and Neck Surgery at (913) 588-6701.
Source: The StayWell Company (2004). Tube Feeding: Skin and mouth care. Retrieved from
www.kramesondemand.com.
Laryngectomy Patient Education 27
Patient Education:
Checking Residual
Residual is the fluid in the stomach that is left over from the previous feeding.
Always check residual before using tube for feedings.
1.
2.
3.
4.
5.
6.
Gather supplies: feeding syringe,
empty cup.
Clamp feeding tube in-between fingers
to prevent contents in tube from leaking
out.
Open the cap of the feeding tube.
Put the tip of the feeding syringe in the
feeding tube.
Pull back gastric contents into syringe with plunger.
Measure amount of gastric contents in syringe. You may need to
empty the gastric contents in to a cup and continue to draw back
gastric contents with syringe.
If residual is less than 100ml:
1. Replace all gastric contents
back into the stomach.
2. Flush the tubing according to
instructions below.
If residual is greater than
100ml:
1. Replace all gastric contents
back into the stomach.
2. Flush the tubing according
to instructions below.
3. Recheck residual in one
hour
If you would like more information or have questions, please contact The University
of Kansas Department of Otolaryngology Head and Neck Surgery at (913) 588-6701.
Source: The StayWell Company (2004). Feeding Tube Care: Flushing. Retrieved from
www.kramesondemand.com.
Laryngectomy Patient Education 28
Patient Education:
Flushing Your Feeding Tube
With tube feeding, you need to keep the tube from getting clogged by flushing
it with warm water before and after each feeding and before and after giving
any medications.
1.
Fill a clean bowl with warm water.
2.
Put the tip of the syringe in the water.
3.
Draw up 50 cc of water.
4.
Clamp feeding tube in-between fingers to prevent
contents in tube from leaking out.
5.
Open the cap on the feeding port.
6.
Put the tip of the syringe in the feeding port.
7.
Push down on the plunger. Let the water run through the tube.
8.
Clamp feeding tube in-between fingers to prevent
contents in tube from leaking out.
9.
Close the cap.
10. Tape the tube to the skin with medical tape.
If you would like more information or have questions, please contact The University
of Kansas Department of Otolaryngology Head and Neck Surgery at (913) 588-6701.
Source: The StayWell Company (2004). Feeding Tube Care: Flushing. Retrieved from
www.kramesondemand.com.
Laryngectomy Patient Education 29
Patient Education:
Tube Feeding
People who can have a normal amount of food at one time can be fed by
bolus feeding. Feedings are most often given every 4 to 6 hours during
waking hours. They are only given in the stomach. When starting a feeding,
open and use only the prescribed amount of liquid food (formula).
Tube Feeding Solution:______________________
Tube feeding amount:_________________cans/day
Water:________________________ml/day
1.
2.
Pull the plunger out of the syringe.
Clamp feeding tube in-between fingers to
prevent contents in tube from leaking out.
3. Open the cap on the feeding port.
4. Put the tip of the syringe in the feeding port.
5. Pour the formula into the syringe.
6. Fill syringe only half-full.
7. Hold the syringe straight up and let the
formula run through the tube by gravity.
8. If the formula is not going in by gravity, put
the plunger back into the syringe. Then push
down slowly on the plunger.
9. Continue pouring tube feeding into the
syringe until you have given the prescribed
amount.
10. After feeding, flush tube as instructed above.
11. Remove the syringe and close the port cap.
If you would like more information or have questions, please contact The University
of Kansas Department of Otolaryngology Head and Neck Surgery at (913) 588-6701.
Source: The StayWell Company (2004). Bolus Tube Feeding. Retrieved from www.kramesondemand.com.
Laryngectomy Patient Education 30
Patient Education:
Medication Administration via Feeding Tube
1.
2.
3.
4.
5.
6.
7.
8.
9.
10.
11.
12.
13.
Prepare liquid medications and set aside.
If medications are in tablet form, crush medications and let them sit in
warm water for 5 minutes prior to putting in the tube.
Pull the plunger out of the syringe.
Clamp feeding tube in-between fingers to prevent contents in tube
from leaking out.
Open the cap on the feeding port.
Put the tip of the syringe in the feeding port.
Pour the medications into the
syringe.
Fill syringe only half-full.
Hold the syringe straight up and let
the medications run through the tube
by gravity.
If the medication is not going in by
gravity, put the plunger back into the
syringe. Then push down slowly on
the plunger.
Continue pouring the medications into the syringe until you have given
the prescribed amount.
After all medications have been given, flush tube as instructed above.
Remove the syringe and close the port cap.
**If tube feedings and medications are due at the same time, administer the
medications half-way through the tube feeding.
If you would like more information or have questions, please contact The University
of Kansas Department of Otolaryngology Head and Neck Surgery at (913) 588-6701.
Source: The StayWell Company (2004). Bolus Tube Feeding. Retrieved from www.kramesondemand.com
Laryngectomy Patient Education 31
Support Groups and Resources
Alcoholics Anonymous
Missouri
District 12 Office
24 Hr. Answering Service
P.O. Box 1673
Columbia, MO 65205
(573)442-4424
St. Louis County Intergroup Office
Trades Center
394 Brooks Dr.
Hazelwood, MO 63042
(314) 731-4854
http://www.ncoaa.org
Jefferson City Answering Service
Jefferson City, MO 65101
(573) 659-6670
Central Services of A.A.
2683 S Big Bend Blvd. Room #4
St. Louis, MO 63143
(314) 647-3677
TDD (314) 647-3683
http://www.aastl.org/
Central Office of SW Missouri
102 A Webb Street
Webb City, MO 64870
(417)673-8591
Kansas
Kansas Area Assembly Central Office
P.O. Box 1773
Salina, KS 67402
(913)823-3058
Kansas City Area Central Office
200 E. 18th Ave.
North Kansas City, MO 64116
24 Hour availability
(816) 471-7229
E-mail: kcacol@juno.com
http://www.kc-aa.org
Information & Service Center
Shawnee Mission, KS 66205
(913) 384-2770
Central Office
1031 E Battlefield St.
Suite 124C
Springfield, MO 65807
(417) 823-7125
United Service Intergroup
P.O. Box 702
Ulysses, KS 67880
(316) 356-3003
Information Exchange Intergroup
P.O. Box 1256
St. Charles, MO 63302
(314) 946-1560
Topeka Area Answering Service
Topeka, KS 66605
(785) 354-3888
Central Office
2812 E. English
Wichita, KS 67211
(316) 684-3661
E-mail: wichitaaaco@aol.com
Laryngectomy Patient Education 32
Support Groups and Resources (continued)
American Cancer Society
www.cancer.org
Cancer Action
Provides free service to cancer patients and their families in the Kansas City
area.
www.canceractionkc.org
Cancer Center Patient Resource Center
(913) 588-0130
InHealth Speakers Club
Free membership provides: quarterly newsletter, new product announcements,
product specials and promotions, and free one-year membership to MedicAlert
($35.00 value).
Email: speakersclub@inhealth.com
(800) 477-5969
The University of Kansas Health Resource Line
(913) 588-1227
National Institutes of Health
www.nih.gov
Nu-Voice Club
An organization of Laryngectomees, families, and friends. Sponsored by The
American Cancer Society.
(816) 842-7111
Smoking Cessation Clinic
Kansas University Medical Center
(913) 588-1227
WebWhispers
Free Laryngectomee support via the Internet at www.webwhispers.org.
Laryngectomy Patient Education 33
Laryngectomy Patient Education 34