A Patient`s Guide to Minimally

Minimally Invasive Total
Hip Replacement: Home Health Guide
What is different about a Minimally Invasive Hip Replacement?
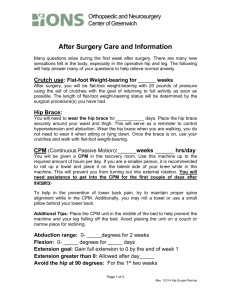
A traditional approach to total hip replacement requires an 8-10" incision on the outside of a patient's thigh. More recently surgeons have begun to decrease the size of the incision, but with traditional technique. In some cases surgeons have been able to reduce the size of the incision to 3-4". This is called the "mini" incision technique, but still requires cutting through muscles, tendons, and hip capsule to do the operation.
The minimally invasive total hip replacement requires two incisions, each about
1 1/2" long. One incision is made in the front of the hip, and one on the side. In this approach the muscles are spread apart rather than cut, leading to less pain and disability.
We are able to do this because we have newly designed instruments which allow us to see better in a small space, and because we use an x-ray machine, called a c-arm, to visualize what we are doing.
What are the advantages of a Minimally Invasive Total Hip
Replacement?
The main advantages are due to faster recovery. We do not cut any muscles, and therefore you can be up and around and walking on this hip the same day of surgery.
You will still experience discomfort, of course, but it should not be debilitating. Some patients feel well enough to go home the same day of surgery, but we are recommending that patients stay overnight in general.
We hope that a faster recovery, and sooner ambulation will lead to a decreased rate of complications as well, but we do not know that yet. Theoretically we should see a lower rate of blood clots, fewer dislocations of the hip, and fewer medical problems. We do not know for sure if this is true because this is a new procedure which hasn't been done before.
What can I expect in the post op recovery of these patients ?
Thigh edema from internal bleeding after surgery is quite common. This leads to a feeling of “tightness” in the hip. Patients do have some same side ankle and foot swelling, and occasionally some abductor weakness.
The patient’s activity level is usually much higher than that of a standard total hip patient.
They will often overdo by walking too much, and experience a high level of pain subsequently. Many of these patients need Percocet rather than Vicodin when they overdo. We are trying to send all of these patients home with Percocet prescriptions.
What are the postoperative physical therapy protocols, and why do these patients have to be seen within 24 hours of discharge ?
These patients most often are discharged after one night in the hospital. While they are able to functionally get up and down stairs and walk at least 100 feet, they still have had recent major surgery. This procedure is also being done under experimental protocol.
We are concerned that patients might have medical difficulty in going home so early, which is why we are having our patient checked so soon after discharge. We may learn over time that this is not necessary, however in this initial phase it is critical that our patients are checked on that first day home by a physical therapist who can let us know if there is a problem that we need to address.
As far as gait these patients should be treated weight bearing as tolerated unless otherwise noted in the MD orders. The approach is anterior to the hip, and therefore special precautions need to be followed.
PT & Nurse Guidelines:
These patients should be seen by a physical therapist the day after discharge, and also by a nurse to draw the protime for the coumadin therapy.
1.
No external rotation
2.
No extension of the hip
3.
Hip abduction is OK. Strengthening of abductors should be encouraged.
4.
No flexion >90 degrees
5.
Do Not cross legs
6.
Do Not sit on low surfaces
7.
Do not twist
8.
Do not ride in an airplane for 6-8 weeks after surgery
9.
Do not ride in a car for more than 45 minutes for 1 month
10.
WBAT unless otherwise instructed
11.
Gradually increase activity level
12.
May shower 24 hours after the wounds are dry
13.
Coumadin is to continue for 3 weeks post operatively. This is per protocol in the
Oakland Anticoagulation Clinic. PT INR should be between 1.5-2.0. Protimes are drawn twice per week starting on the day after discharge. These blodd draws continue 2x per week for 3 weeks.
14.
Long leg TED hose are to be continued for 4 weeks post operatively
ANY QUESTIONS? PLEASE CALL DR. BARBER at 510-752-6890 OR DR. TRAUNER at 510-752-
6222. Our nurses: Mary Ellen for Dr. Barber at 510-752-6903 or Phyllis for Dr. Trauner at 510-752-6929