Sedation and General AnesthesiaDOC
advertisement

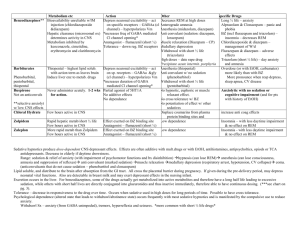
Pediatric Dentistry 538 WEB Lecture Child Management – Sedation and General Anesthesia Author – Dr. Norman Tinanoff SPECIFIC OBJECTIVES: The student should know: 1. The general concepts and requirements of sedation for children. 2. The anatomic and physiologic differences between children and adults that affect sedation techniques. 3. The general concepts of the techniques and agents that are used to sedate child patients for dental procedures. 4. The indications for general anesthesia to perform oral rehabilitation in children. METHODOLOGY: ASSIGNMENT: WEB Lecture McDonald and Avery, 2000; Chapters 14, pages 297-324; Chapter 15, pages 325-348 - 534 Synopsis Concepts of Sedation in Children The goals of conscious sedation for pediatric patients are to control behavior that interferes with the provision of dental care and to produce a patient that will have a positive attitude toward future care. Sedated children have all reflexes intact, have the ability to maintain a patent airway and can respond to physical stimuli and verbal commands. Deep sedation involves partial or complete loss of the ability to continuously maintain a patent airway and the patient does not respond purposefully to physical stimulation or verbal commands. Requirements for sedation: Thorough knowledge of agents to be used. Careful planning taking into consideration patient’s age, weight and behavior. Patient evaluation to consider conditions that might alter the expected response including previous experiences with sedation, lung and airway patency. Medical history that includes current medications, allergies, previous hospitalizations. Well-documented informed consent that includes risks, benefits and alternative procedures. Office facilities that allow for appropriate monitoring. Emergency medical services and office personal thoroughly trained in their use. Anatomic and Physiologic Differences in Children Compared to an Adult Basal metabolic activity is greater in children, which affects drug response and oxygen demand. Airway management is more difficult in children because of narrow nasal passages and frequent hypertrophic tonsils and adenoids. Children have less functional oxygen reserve due to smaller lungs with less expansion capability. The heart rate is faster and the blood pressure is lower than adults. The effect and duration of drugs is more variable in children. Sedation Techniques Sedative drugs may be administered by inhalation, oral, rectal, submucosal, intramuscularly or intravenous routes. Inhalation of nitrous oxide-oxygen mixture is often combined with any of the other routes. Nitrous oxide produces nonspecific central nervous system depression with limited analgesia. At levels of 30-50%, it will produce a somnolent patient who may appear dissociated and easily susceptible to suggestion. In combination with other drugs, nitrous oxide potentiates the effects; however, it is safer than increasing the sedative drug because it can be rapidly reversed. The oral route is the most variable because the effect depends on absorption through the gastrointestinal mucosa. It is also difficult to reverse oral medications. Recovery time may be prolonged. Papoose Board is often used to restrain children who are combative. Shoulder rolls keep the head slightly up and back. Nitrous oxide is generally used with oral sedation. Intramuscular sedation also has a similar problem as the oral route in that there is a prolonged time to peak effect and the lack of reversibility. Intravenous sedation is the easiest and most efficient, but extremely hard to manage in child patients because of behavior and very small veins. Common Agents Antihistamines such at hydroxyzine (Atarax, Vistaril), promethazine (Phenergan) and diphenhydramine (Benadryl) are rapidly absorbed from the GI tract and ideal for oral administration. They produce drowiness, prevent histamine release and have antiemetic properties.. Clinical effect is in 30 minutes. Excretion is by the liver and the half-life is 3 hours. Vistaril dosage is 0.6 mg/kg and comes in a dosage of 25 mg/5 ml. Antianxiety agents such as diazepam (Valium) medazolam (Versed) are rapidly absorbed in the GI tract. They tranquilize as well as produce amnesia. Diazepam halflife is 20-50 hours and can have a rebound effect with the consumption of a fatty meal. Oral dosage of 0.2 – 0.5 mg/kg. Medazolam has twice the potency as diazepam. Halflife is 2-5 hours. It can produce respiratory depression at high dosages. Dosage is 0.25 – 0.5 mg/kg, supplied as syrup in a concentration of 2 mg/ml. Flumazenil is a benzodiazepine receptor antagonist and reversal of sedation can be given with an initial dose of 0.2 mg, with repeats at 1-minute intervals. Sedative hypnotics such as barbiturates can produce all levels of CNS depression. Short-acting barbiturates include seconal, triazolam and pentobarbital. They are not used that often because of other more modern drugs. Chloral hydrate (Noctec), 25-60 mg/kg, taken orally has an onset of action within 30 minutes, peak effect in 1 hour, and half-life of 8-11 hours. It has an unpleasant taste and irritates the gastric mucosa. Young children should not receive more than 1-gram total dose. At higher dosages and in combination with other drugs there can be loss of a patent airway. Dissociative agent such as Ketamine (Ketalar) produce a cataleptic state with profound analgesia and amnesia. Dosage 3 – 7 mg/kg IM. Disadvantages increase salivation, increase heart rate, potential for delirium in older children, potential for laryngospasm. Advantage is rapid onset, no respiratory depression, lack of skeletal movement. Often used with medazolam (to potentiate effect and amnesia) and atropine (to reduce salivary secretions). Narcotics such as meperidine (Demerol) and fentanyl (Sublimaze) produce hypnotic states, relief from pain and respiratory depression. They are powerful potentiators of other CNS depressant drugs. Demerol can be administered orally but with rapid loss due to liver metabolism. Dosage in all three routes is 1- 2.2 mg/kg. Oral syrup is 50mg/5ml; parenteral solutions come in 25, 50, 75 and 100 mg/ml. Fentanyl is approximately 1,000 times more potent that meperidine. Dosage is 0.002 – 0.004 mg/kg. Nalozone (Narcan) is the preferred narcotic antagonist. It acts in 2-5 minutes after a subcutaneous dose. Duration of reversal is about 45 minutes. Dosage 0.1 mg/kg with subsequent dosages of 0.1 mg/kg every 2-3 minutes. Caution -- the duration of the opiate is longer that that of the antagonists. Monitoring If the patient is being sedated, heart, respiratory rate, blood pressure and oxygen saturation need to be continuously monitored. Hypoxia is the primary complication in children. Pulse oximeters are adequate for measuring blood oxygen saturation, but devices that measure the respiratory concentration of carbon dioxide (capnographs) is a better measure inspired and end-tital respirations. Dental Procedures Performed on a Sedated Child Patient Note monitoring devices on the child General Anesthesia There are many indications for treating a child in the hospital with general anesthesia for oral rehabilitation. Some of these include: very young children requiring extensive dental work. children that have to travel significant distances for dental care. children with mental or physical handicapping conditions that makes treatment in the outpatient setting very difficult. children with severe dental phobias that does not permit dental care in the out patient setting. Dentists who wish to work in the hospital OR generally must have advanced training that has included experience in the hospital setting. Additionally, dentists must apply for and receive hospital privileges from the hospital credentials committee. Dental procedures are performed as a “dirty case” which means that absolute sterile operating conditions are not followed. However, the patient is draped with sterile clothes, and the operators perform normal scrubbing and gowning procedures. Instruments for restorative procedures in the OR are the same as those for procedures in the dental operatory. The use of rubber dam isolation is preferred for all operative procedures. The treatment plan may be modified in that all restorations should provide greatest longevity. Conservative procedures are not performed on questionable teeth.