Radius Bone - By Dr Nand Lal Dhomeja ( Anatomy Department )
advertisement
")
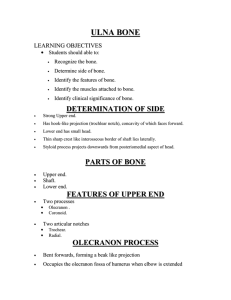
RADIUS BONE & BONES OF HAND LEARNING OBJECTIVES Students should able to • Recognize the bones of forearm &hand • Determine side of bones. • Identify the features of bones. • Identify the muscles attached to bones. • Identify clinical significance of bones. RADIUS BONE • Lateral bone of forearm • Three Parts • Upper end Head Neck Tuberosity • Shaft • Lower end DETERMINATION OF SIDE • Upper end rounded & bears the head. • Lower end more wider than the upper end • Lateral surface of shaft is convex & its anterior surface is concave in lower part • Styloid process projects from lateral surface of the lower end HEAD Disc-shaped, overhangs the neck on all sides • Medially it articulates with radial notch of ulna. • Upper surface articulates with capitulum-- form elbow joint • It is covered with hyaline cartilage. •Medial surface articulates with radial notch of ulna to form superior radio-ulnar joint Attachment Annular ligament to the articular cicumference of head NECK • Constricted part below head • Surrounded by lower part of annular ligament • Attachments: Supinator is inserted into the lateral anterior &posterior aspects of neck TUBEROSITY Lies below the medial part of the neck. • Attachments: • Biceps brachii is inserted into rough posterior part. • Smooth anterior part is related to bursa. SHAFT • Narrow above, broader below • Three borders. • Interosseous(medial) • Anterior • Posterior Three surfaces • • Anterior • Posterior • Lateral BORDERS INTEROSSEOUS (MEDIAL) BORDER • Sharp except at its upper part • Begins from posterio-inferior part of radial tuberosity • Lower end form posterior boundary of small triangular area above ulnar notch of radius Attachment on interosseous border • • Pronator quadratus is inserted Gives attachment to interosseous membrane in lower 3\4 ANTERIOR BORDER Begins just below antero-lateral part of radial tuberosity Upper & lower parts are sharp • • Attachments on anterior border • • Origin of Flexor digitorum superficialis from upper & lower parts Extensor retinaculum is attached to lower edge POSTERIOR BORDER Begins from posterio-inferior part of tuberosity End in dorsal tubercle at back of lower end Prominent in middle part • • • SURFACES ANTERIOR SURFACE Lies between anterior and interosseous border Presents nutrient foramen directed up ward • • Attachments on anterior surface • • Origin to flexor pollicis longus from upper 2\3 Insertion to pronator quadratus in lower 1\4 POSTERIOR SURFACE • • • Lies between interosseous & posterior borders Origin of Abductor pollicis longus from upper part Origin of Extensor pollicis brevis from lower part LATERAL SURFACE • • • • Lies between anterior&posterior borders Rough ridge in middle part gives insertion to pronator teres Insertion to supinator into V Shape area at upper part Brachioradialis is inserted just above styloid process LOWER END • Expanded &rectangular • Has five surfaces • Lateral surface • Medial surface • Anterior surface • Posterior surface • Inferior surfaces • LATERAL SURFACE • • • • Present styloid process Radial collateral ligament of wrist joint is attached at tip of styloid process Brachiodialis is inserted into lower part of lateral surface Two grooves lateral to styloid process for tendons of Abductor pollicis longus &Extensor pollicis brevis MEDIAL SURFACE Bears ulnar notch for articulation with head of ulna Articular disc of inferiorradio-ulnar joint is attached to ridge at lower part. ANTERIOR SURFACE • In form of thick prominent ridge • Radial artery is palpated as radial pulse • Pronator quadratus is inserted into the lower part of anterior surface POSTERIOR SURFACE • Irregular • Present dorsal tubercle(of lister) • Four grooves for extensor tendons • • INFERIOR SURFACE • • • Bears triangular area for Scaphoid bone Medially, quadrangular area for Lunate Takes part in forming wrist joint CLINICAL ANATOMY Fractures of radius Fracture of head • Can occur from fall on outstretched hand Fracture of neck of radius • Occur in young children FRACTURES OF SHAFT OF RADIUS • May or may not occur with ulna • Displacement of fractured fragment depends on pull of muscle • Supinator and biceps supinate the proximal fragment • Pronator quadratus pronates the distal fragment • Brachioradialis and extensor carpi radialis and brevis shortens the fore arm COMBINE FRACTURES OF RADIUS AND ULNA • • • Shaft of ulna fractured by a force from behind Bowing forward of ulnar shaft with anterior dislocation of radial head Rupture of annular ligament COMBINE FRACTURES OF RADIUS AND ULNA • Proximal third of radius is fractured • Distal end of ulna is dislocated at distal radio ulnar joint FRACTURES OF DISTAL END Colles’ fracture • Fall on outstretched hand • Distal fragment is displaced posteriorly and superiorly • The fore arm and wrist resembles the shape of dinner fork • Dinnerfork deformity • Reverse colles’s fracture • Distal fragment displaced anteriorly • Fall on back of hand • BONES OF HAND • Eight carpal bones Five metacarpal bones Fourteen phalanges • Eight carpal bones • Arranged in two rows • • CARPAL BONES Proximal row Medial to lateral • Scaphoid • Lunate • Triquetral • Pisiform Distal row • Trapezium • Trapezoid • Capitate • Hamate CHARACTERISTICS OF EACH BONE Each bone has six surfaces. Scaphoid is boat –shaped • tubercle on its lateral side Lunate is half moon shaped or crescentic Triquetral is pyramidal shape • has oval facet on distal part of palmar surface Pisiform is pea shaped • only one oval facet on proximal part of dorsal surface Trapezium is quadrangular in shape • crest & groove anteriorly Trapezoid resemble shoe of baby Capitate is largest with rounded head Hamate is wedge –shaped with hook near base ATTACHMENTS Most important structure related with carpal bones --------- FLEXOR RETINACULUM Attachment: Lateral • scaphoid • anterior border of lower end Medial • Pisiform • Hamitate CLINICAL ANATOMY Fracture of scaphoid • Most common fractured bone among carpal bone • Non union & avascularity common problem • Tenderness & swelling in anatomical snuff box Dislocation of lunate • • • • Most common dislocated bone of carpal bone May compress median nerve in front of wrist Carpal tunnel syndrome CARPAL TUNNEL SYNDROME Carpal tunnel: • osseofibrous space formed by anterior concave surface of carpus and flexor retinaculum • Passage of long flexor tendon and median nerve CARPAL TUNNEL SYNDROME • Syndrome is caused by compression of median nerve due to reduced size of canal • Pain and paraesthesia of lateral one and half finger • Weakness of thenar muscle METACARPAL BONES • Short long bones • Numbered from lateral to medial side • 1st metacarpal Shorter & thicker articulates with trapezium. Other metacarpal bones • • • • • Expanded bases articulate with distal row of carpal bones & with each other Middle metacarpal show styloid process Heads has boldly rounded articular facets Form concavity for palm Heads form knuckles of fist PHALANGES 14 in number Parts Base Shaft Head