Parturition/Stages of Labor
Methodius Tuuli, MD, MPH
Division of Maternal-Fetal Medicine
2
Objectives
1. Describe physiology of labor
2. Define stages of labor
3. Discuss concepts of normal labor progress
– Traditional (Friedman’s)
– Contemporary (Zhang’s)
– Custom labor curve (Cahill/Tuuli)
PARTURITION
4
Parturition
• Early Pregnancy
– Uterine quiescence
– Closed cervix
Fetus
• Parturition
– Coordinated uterine activity
– Cervical remodelling
– Progressive cervical dilation
Placenta
Membranes
Mother
5
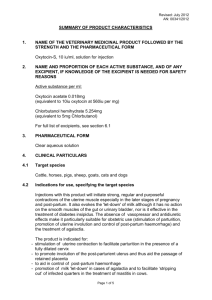
Mediators of Uterine Activity
Inhibitors
•Progesterone
•Prostacycline
•Relaxin
•Nitric Oxide
•Parathyroid
hormone-related
peptide
•CRH
•HPL
Quiescence
Uterotrophins
Estrogen
•Progesterone
•Prostaglandins
•CRH
Activation
Uterotonins
Prostaglandins
Oxytocin
Stimulation
Involution
Oxytocin
•Thrombin
Involution
6
Initiation of Labor
• Fetus
– Sheep
• Fetal ACTH and cortisol
– Placental 17 α hydroxylase
– Estradiol
– Progesterone
– Placental production of oxytocin, PGF2 α
– Humans
• Fetal increased DHEA
– Placental conversion to estradiol
– Increased decidual PGF2 and gap junctions
– Increased oxytocin and PG receptors
– Changes in progesterone receptors
7
Initiation of Labor
• Oxytocin
– Peptide hormone
– Hypothalamus-posterior pituitary
– Oxytocin receptors
• Fundal location
• 100-200 x during pregnancy
– Actions
• Stimulate uterine contractions
• Stimulate PG production from amnion/decidua
8
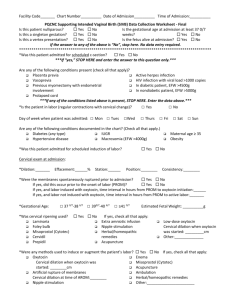
Oxytocin receptor
Calcium channel
Extracellular
Intracellular
Phospholipase C
cAMP
Ca+
+ Oxytocin
+ Prostaglandin
MLCK
Ca store
Uterine contractions
9
LABOR
10
Labor
Regular uterine contractions
and
Progressive cervical dilatation
11
Labor
• Cervical effacement
• Cervical dilatation
12
Labor: the three “P’s”
• Passage
• Passenger
• Powers
13
Passage
14
Passenger
• Size
– Estimated fetal weight
• Lie
– Longitudinal
– Transverse/oblique
• Presentation
– Vertex 95%
– Non-vertex 5%
• Station
• Position
15
Passenger: cardinal movements of labor
•
•
•
•
•
•
Descent
Flexion
Internal rotation
Extension
External rotation
Expulsion
16
Powers
• Uterine contractions
– Duration 30-60 seconds
– 3-5 contractions / 10 minutes
– Montevedeo units (intrauterine catheter)
• Baseline to peak
• Sum over 10 minutes
• Adequate: >200-250 MVU
17
LABOR PROGRESS
18
Stages of Labor
• First stage – onset of labor to complete dilatation
– Latent phase
– Active phase
• Second stage – complete cervical dilation to expulsion
of fetus
• Third stage – expulsion of fetus to expulsion of placenta
• (Fourth Stage – First hour after expulsion of placenta)
19
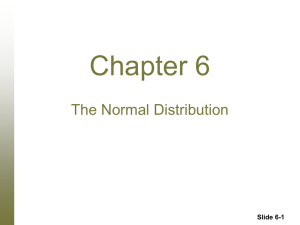
Labor Curve
20
First Stage
• Latent phase – onset to rapid cervical change
• Active phase – rapid cervical change to complete
dilatation
• Traditional standards
Nulliparous
95th
Mean
% tile
Latent
phase
Active
phase
Multiparous
95th
Mean
%tile
7.3-8.6hr 17-20 hr 4.1-5.3hr 12-14 hr
1.5cm/hr
1.2cm/hr
21
Second Stage
• Traditional standards
No epidural
Epidural
Nulliparous
95th
Mean
% tile
53-57
122-147
min
min
79 min
185 min
Multiparous
95th
Mean
%tile
17-19
57-61
min
min
45min
131min
• Immediate versus delayed pushing
• Spontaneous versus coached pushing
22
Third Stage
• Standards
– Mean – 6 minute
– 97th% tile – 30 minutes
• Active versus passive
23
CHANGING LABOR STANDARDS
24
Why concern?
l
Too many cesarean
Why concern?
1955: Friedman’s Labor Curve
• Convenience sample
– 622 consecutive nullips
– 500 with adequate data
• Cervical dilation (Y) plotted against time (X)
• Major advance in his day
“…..introduces a new dimension to us. Evaluation of progress,
previously synonymous with nebulous degree of change,
becomes available to us in terms of specific change.”
Traditional labor curve: Friedman’s
28
Limitations of Friedman’s Curve
• Non-representative sample
• More ‘graphical’ than ‘statistical’
– Did not take into account special characteristics of labor
data
• Adopted without complete context
– Subject characteristics
– Interventions
2002: Zhang’s Labor Curve
• Took into account the unique features of labor data
–
–
–
–
Left censored
Interval censored
Repeated measures
Log-normal distribution
• ‘Appropriate’ analytical tools
– Repeat ed measures regression curves
– Interval censored regression models medians (95th tile)
• Contemporary sample
2002: Zhang’s Labor Curve
2002: Zhang’s Labor Standard
Zhang’s curve: key concepts
• Transition to active labor after 6cm dilation; not 4cm.
• No deceleration phase
• Traverse times
– much longer in latent phase
– much shorter in active phase
TOWARDS CUSTOM LABOR STANDARDS
34
4
6
8
10
Does one size fit all?: Fetal Size
0
2
4
6
Duration of labor (hours)
<2500g
3000-3500g
>4000g
2500-3000g
3500-4000g
8
Does one size fit all?: Fetal Sex
Cahill AG, Roehl KA, Odibo AO, Zhao Q, Macones GA. Am J Obstet Gynecol. 2012 Apr;206(4):335.e1-5.
Does one size fit all? Maternal Race
Does one size fit all? Induced labor
Harper LM, Caughey AB, Odibo AO, Roehl KA, Zhao Q, Cahill AG. Obstet Gynecol. 2012 Jun;119(6):1113-8.
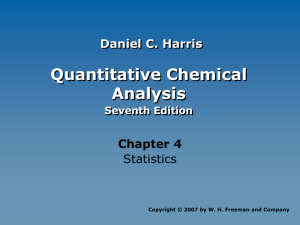
Does one size fit all? Induction method
2
4
6
8
10
Average Labor Curves: Misoprostol versus Foley Catheter
0
5
10
Duration of Labor (hours)
Misoprostol
15
20
Foley Catheter
Tuuli MG, Keegan MB, Odibo AO, Roehl K, Macones GA, Cahill AG. Am J Obstet Gynecol. 2013 Sep;209(3):237.e1-7.
Does one size fit all?: Maternal Obesity
Norman SM, Tuuli MG, Odibo AO, Caughey AB, Roehl KA, Cahill AG. Obstet Gynecol. 2012 Jul;120(1):130-5.
Custom Labor Curve: the Holy Grail
Seeks to incorporate the multiplicity of individual patient factors
in estimating expected labor progress
• Has been methodologically challenging
• Recent progress
– N=5000
– Detailed labor data
– Collaboration with statisticians
– Mathematical model incorporating
•
•
•
•
Parity
Epidural
BMI
Labor type
Custom Labor Curve: the Holy Grail
Custom Labor Curve: the Holy Grail
• Next steps
–
–
–
–
Validate in independent data set (N=4000)
Refine model to include time variable factors
Software development
RCT to assess impact on cesarean rate
Summary
• Labor involves transition of the uterus from a
quiescent state to regular contractions and cervical
dilation resulting in delivery of the fetus and placenta
• Initiation of labor in humans is incompletely
understood, but involves maternal-fetal-placental
interactions
44
Summary
• Clinical management of labor requires
understanding of the normal progress
• Our understanding of normal progress of
labor is evolving towards more ‘customized’
individualized standards
45
Questions