September 23, 2014
advertisement

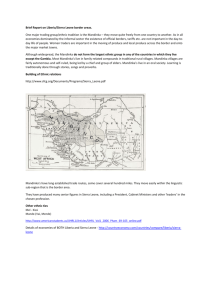
Modeling the Ebola Outbreak in West Africa, 2014 Sept 23rd Update Bryan Lewis PhD, MPH (blewis@vbi.vt.edu) Caitlin Rivers MPH, Eric Lofgren PhD, James Schlitt, Katie Dunphy, Henning Mortveit PhD, Dawen Xie MS, Samarth Swarup PhD, Hannah Chungbaek, Keith Bisset PhD, Maleq Khan PhD, Chris Kuhlman PhD, Stephen Eubank PhD, Madhav Marathe PhD, and Chris Barrett PhD Currently Used Data Guinea Liberia Nigeria Sierra Leone Total ● ● ● ● Cases 861 2712 22 1603 5198 Deaths 557 1137 8 524 2226 Data from WHO, MoH Liberia, and MoH Sierra Leone, available at https://github.com/cmrivers/ebola MoH and WHO have reasonable agreement Sierra Leone case counts censored up to 4/30/14. Time series was filled in with missing dates, and case counts were interpolated. 2 Epi Notes • WHO reports results on case history analysis providing clarity on some disease parameters NEJM • CDC releases their model with some dire forecasts MMWR • Sierra Leone not doing as well as they report – More graves from Ebola patients than reported cases – NY Times 3 Comparison of Parameters 4 Liberia- Case Locations 5 Liberia – Contact Tracing 6 Contact Tracing Metrics 7 Sierra Leone – Contact Tracing Efficiency 8 Sierra Leone – Case Finding Assuming all cases are followed to the same degree, this what the “observed” Re would be based on cases found from contacts (using time lagged 7,10,12 day reported cases as denominator) 9 Twitter Tracking Most common images: Solidarity with Ebola affected countries, Jokes about bushmeat, Ebola risk, and names, Positive health message 10 Liberia Forecasts Forecast performance 8/13 – 8/19 8/20 – 8/26 8/27 – 9/02 9/3 – 9/9 9/10 – 9/16 9/179/23 9/24 – 9/30 175 353 321 468 544 -- -- Forecast 176 229 304 404 533 801 1105 Actual 52% of Infected are hospitalized Reproductive Number Community 1.5 Hospital 0.1 Funeral 0.4 Overall 2.0 11 Liberia Forecasts – Role of Prior Immunity 12 Sierra Leone Forecasts Forecast performance 41% of cases are hospitalized 13 Prevalence of Cases 14 All Countries Forecasts Model Parameters 'alpha':1/10 'beta_I':0.200121 'beta_H':0.029890 'beta_F':0.1 'gamma_h':0.330062 'gamma_d':0.043827 gamma_I':0.05 'gamma_f':0.25 'delta_1':.55 'delta_2':.55 'dx':0.6 rI:0.85 rH:0.74 rF:0.31 Overal:1.90 15 Combined Forecasts Reproductive Number Community 1.3 Hospital 0.1 Funeral 0.3 Overall 1.7 8/10 – 8/16 8/17 – 8/23 8/24 – 8/30 8/31– 9/6 9/8 – 9/13 9/149/20 9/21 – 9/27 9/28 – 10/4 Actual 231 442 559 783 681 -- -- -- Forecast 329 393 469 560 693 830 1007 1213 16 Learning from Lofa • Lofa has experienced decreasing cases for several weeks – Exploring with contacts in MoH about whether these are reporting artifact or reality and to understand what factors are driving it • The decrease starts at 0.13% of population infected – Montserrado is currently at 0.101%, model predicts this will occur on 9/19 • If we fit the decreased rate in Lofa what might Monteserrado look like? – Assuming equal decrease across all betas until more info available 17 Learning from Lofa 18 Learning from Lofa 19 Hospital Beds – Prelim analysis • Proposed scenario of 70% in hospital beds will tip epidemic • Explore using Compartmental Model – Based on Liberia wide model – Trigger change at a certain point in time (ie instantaneously move up to 70%) – Transmission in hospitals also assumed to be 90% better than current fit 20 Hospital Beds – Prelim analysis Impact in Liberia Cases on Feb 1 Oct 1 155k Nov 1 226k Dec 1 352k Jan 1 521k No beds 669k 21 Hospital Beds – Discrete Rollout • Using Stochastic model – Monteserrado model fit (very high transmission fit) – 170 beds start arriving every week from midOctober on – These beds are assumed to be 100% effective – If beds are full, the current “hospitals” are assumed to absorb – No lower tier but better than current ECUs in place 22 Hospital Beds – Discrete Rollout 23 Synthetic Liberia Now integrated into the CNIMS interface 24 Agent-based Simulations • Running simulations on two simulation platforms – EpiFast – Fast, integrated with CNIMS interface, some interventions and behaviors can’t be represented – EpiSimdemics – Very flexible, can represent nearly any conceivable behavior or intervention, slower, and more cumbersome to execution 25 ABM of Monrovia 26 EpiSimdemics ABM running 27 Next steps • Focus on agent-based model – Incorporating regional travel – Re-calibrate with WHO based parameters – Set up to incorporate behaviors • Address bed rollout in Stochastic Compartmental model – Sensitivity analysis to identify what capacities and assumed reductions are necessary for turning the epidemic down. 28 Supporting material describing model structure, and additional results APPENDIX 29 Further evidence of endemic Ebola • 1985 manuscript finds ~13% sero-prevalence of Ebola in remote Liberia – Paired control study: Half from epilepsy patients and half from healthy volunteers – Geographic and social group sub-analysis shows all affected ~equally 30 Legrand et al. Model Description Susceptible Exposed not infectious Infectious Symptomatic Hospitalized Infectious Funeral Legrand, J, R F Grais, P Y Boelle, A J Valleron, and A Flahault. “Understanding the Dynamics of Ebola Epidemics” Epidemiology and Infection 135 (4). 2007. Cambridge University Press: 610–21. doi:10.1017/S0950268806007217. Infectious Removed Recovered and immune or dead and buried 31 Compartmental Model • Extension of model proposed by Legrand et al. Legrand, J, R F Grais, P Y Boelle, A J Valleron, and A Flahault. “Understanding the Dynamics of Ebola Epidemics” Epidemiology and Infection 135 (4). 2007. Cambridge University Press: 610–21. doi:10.1017/S0950268806007217. 32 Legrand et al. Approach • Behavioral changes to reduce transmissibilities at specified days • Stochastic implementation fit to two historical outbreaks – Kikwit, DRC, 1995 – Gulu, Uganda, 2000 • Finds two different “types” of outbreaks – Community vs. Funeral driven outbreaks 33 Parameters of two historical outbreaks 34 NDSSL Extensions to Legrand Model • Multiple stages of behavioral change possible during this prolonged outbreak • Optimization of fit through automated method • Experiment: – Explore “degree” of fit using the two different outbreak types for each country in current outbreak 35 Optimized Fit Process • Parameters to explored selected – Diag_rate, beta_I, beta_H, beta_F, gamma_I, gamma_D, gamma_F, gamma_H – Initial values based on two historical outbreak • Optimization routine – Runs model with various permutations of parameters – Output compared to observed case count – Algorithm chooses combinations that minimize the difference between observed case counts and model outputs, selects “best” one 36 Fitted Model Caveats • Assumptions: – Behavioral changes effect each transmission route similarly – Mixing occurs differently for each of the three compartments but uniformly within • These models are likely “overfitted” – Many combos of parameters will fit the same curve – Guided by knowledge of the outbreak and additional data sources to keep parameters plausible – Structure of the model is supported 37 Liberia model params 38 Sierra Leone model params 39 All Countries model params 40 Long-term Operational Estimates Turn from 8-26 End Total Case from 8-26 Estimate 1 month 3 months 13,400 1 month 6 months 15,800 1 month 18 months 31,300 3 months 6 months 64,300 3 months 12 months 91,000 3 months 18 months 120,000 6 months 12 months 682,100 6 months 18 months 857,000 • Based on forced bend through extreme reduction in transmission coefficients, no evidence to support bends at these points – Long term projections are unstable 41