Gas Transport in The Blood
advertisement

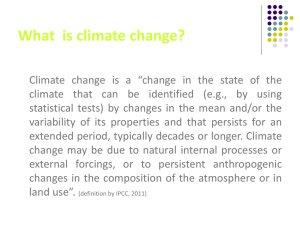
Gas Transport in the Blood Dr Shihab Khogali Ninewells Hospital & Medical School, University of Dundee Understand the effect of partial pressure on O2 and CO2 carriage in the blood Understand the means of O2 carriage in the blood Understand the oxygenhaemoglobin dissociation curve and the significance of its sigmoid shape Know the Bohr effect and its significance in O2 liberation at tissue level What is This Lecture About? Understand the means of CO2 carriage in the blood Know the Haldane effect and its significance in the uptake of CO2 and CO2 generated H+ at tissue level; and CO2 liberation at the lungs See blackboard for detailed learning objectives Atmospheric air Alveoli O2 Picked up by blood at the lungs must be transported to the tissues for cellular use Pulmonary circulation Systemic circulation CO2 produced at tissues must be transported to the lungs for removal from the body Oxygen Partial Pressures around the System Air PO2 kPa 20 Gas Pulmonary Capillary Arterial Diffusion 10 Atmosphere Tissues This means that if the partial pressure in the gas phase is increased the concentration of the gas in the liquid phase would increase proportionally The partial pressure of a gas in solution is its partial pressure in the gas mixture with which it is in equilibrium What is the Effect of Partial Pressure on Gas Solubility? Henry’s Law •Gaseous Phase •Liquid Phase (gas in solution) The amount of a given gas dissolve in a given type and volume of liquid (e.g. blood) at a constant temperature is: proportional to the partial pressure of the gas in equilibrium with the liquid Dissolved Oxygen The O2 amount dissolved in blood is proportional to the partial pressure (Henry’s Law) 3ml O2 per litre of blood at a PO2 of 13.3 kPa Under Resting conditions (cardiac output 5L/min): 15 ml/min of O2 is taken to tissues as dissolved O2 Even at strenuous exercise (cardiac output of 30 L/min): 90 ml/min would be taken to tissues as dissolved O2 Resting O2 consumption of our body cells is about 250ml/min O2 consumption may increase up to 25 folds during strenuous exercise – Clearly, another mechanism is involved in O2 transport in the blood. Oxygen Transport in the Blood Most O2 in the blood is transported bound to haemoglobin in the red blood cells Normal O2 concentration in the arterial blood is about 20 ml/100 ml (200 ml per litre) at a normal arterial PO2 of 13.3 kPa and a normal haemoglobin concentration of 15 grams/100 ml Percentage of O2 carried bound to haemoglobin = 98.5% Percentage of O2 carried in the dissolved form = 1.5% (3 ml per litre at a PO2 of 13.3 kPa ) O2 is present in the blood in two forms: (1) bound to haemoglobin (2) physically dissolved (very little O2) Oxygen binding to haemoglobin Haemoglobin can form a reversible combination with O2 Each Hb molecule contains 4 haem groups Each haem group reversibly binds to one O2 molecule Haemoglobin is considered fully saturated when all the Hb present is carrying its maximum O2 load The PO2 is the primary factor which determine the percent saturation of haemoglobin with O2 5.3 8.0 Blood PO2 (kPa) 13.3 O2 concentration ml/100 ml % Haemoglobin Saturation Oxygen Haemoglobin Dissociation Curve 100 % Hb saturation Total O2 20 O2 combined with Hb Dissolved O2 0 0 0 PO2 (kPa) 13 O2 concentration (ml/100 ml) Oxygen Haemoglobin Dissociation Curve 100 Hb =20 100 Hb =15 20 100 Hb =10 0 0 13 PO2 (kP) 0 0 0 % Hb saturation O2 concentration (ml/100 ml) Saturation Oxygen binding of haemoglobin Binding of one O2 to Hb increases the affinity of Hb for O2 – co-operativity – Sigmoid Flattens where all sites are becoming occupied Flat upper portions means that moderate fall in alveolar PO2 will not much affect oxygen loading Steep lower part means that the peripheral tissues get a lot of oxygen for a small drop in capillary PO2 % Haemoglobin Saturation Significance of Sigmoid 5.3 8.0 Blood PO2 (kPa) 13.3 Bohr Effect A shift of the curve to the right:- The Bohr Effect % Hb saturation 100 Increased release of O2 by conditions at the tissues PCO2 [H+] Temperature 2,3-Biphosphoglycerate 0 PO2 Off-loading of O2 at Tissues Curve in arterial conditions O2 content (ml/10mls) 20 Curve in tissue conditions Additional O2 given up 10 Tissue O2 Tension 0 0 20 2.6 40 5.3 60 8.0 80 10.6 PO2 (mm Hg, kP) Arterial O2 Tension 100 13.3 Means of CO2 Transport in the Blood Solution (10%) As Bicarbonate (60%) As Carbamino compounds (30%) (1) CO2 in Solution Henry’s Law Carbon dioxide about 20 times more soluble than oxygen About 10% of carried CO2 is in solution (2) Bicarbonate: Most CO2 is transported in the blood as bicarbonate Bicarbonate is formed in the blood by:- CO2 + H2O CA H2CO3 H+ + HCO-3 Carbonic Anhydrase Occurs in red-blood cells Bicarbonate Formation Chloride shift Capillary wall - Cl + CO2 - H + HCO3 H2CO3 H+ + Hb CA H2O + HbH Red blood cell (3) Carbamino Compounds Carbamino compounds formed by combination of CO2 with terminal amine groups in blood proteins. Especially globin of haemoglobin to give carbamino-haemoglobin Rapid even without enzyme Reduced Hb can bind more CO2 than HbO2 CO2 concentration (ml/100ml) CO2 Dissociation Curve 5.3 55 v- PO2 13.3 PO2 a = CO2 content in arterial blood v- = CO2 content in mixed venous blood a 45 5.3 6.6 CO2 partial pressure (kP) The Haldane Effect Removing O2 from Hb increases the ability of Hb to pick-up CO2 and CO2 generated H+ The Boher effect and the haldane effect work in synchrony to facilitate: O2 liberation and uptake of CO2 & CO2 generated H+ at tissues Summary of CO2 Transport in the Blood