The Urinary (Excretory) System
advertisement
 System")
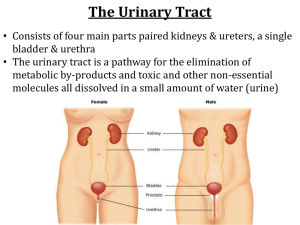
The Urinary (Excretory) System Functions of the Urinary System (aka Functions of Kidneys) (see p. 305) 1. Removal of metabolic wastes; 2. Maintenance of water-salt balance in body (blood). 3. Maintenance of acid-base balance in body (blood). 4. Hormonal function (EPO) – described in Circulatory System; as well as Renin (an enzyme), described later. Excretion • The removal of metabolic wastes (nitrogen-based (nitrogenous)) from the body. • The metabolism of amino acids, nucleotides, and creatine phosphate (all of which are nitrogenous) results in nitrogenous wastes that need to be ‘disposed’ of by the body. • Typical nitrogenous wastes that humans excrete include, in order of amount: urea, creatinine, uric acid, ammonia (which tends to buffer H+ present in urine – forming NH4+ (ammonium)). Ammonia is present in trace amounts. • Feces is not considered to be metabolic waste…it consists of materials that never actually ‘entered’ the body; the ridding of feces is known as elimination. Amino Acid Metabolism - the deamination of amino acids (ie. the removal of the amino (-NH2) group) occurs in the liver in order to convert three amino acids into a glucose. - Deamination results in the formation of ammonia (NH3), which is a basic, toxic chemical requiring a large amount of water for safe dilution and subsequent removal from any animal. - Thus, to conserve water for the body, the human liver converts the majority of the ammonia into urea, which is far less toxic, and requiring much less water for disposal, than ammonia. - Urea is filtered out of the blood into the urine by the kidneys. Ammonia reacts with CO2 in the liver to produce UREA: 2 NH3 + CO2 + H2O Nucleotide Metabolism - if too many DNA/RNA/ADP nucleotides exist within the body or if they become degraded to a non-functional state, they might be metabolized in order to conserve space within cells. - The metabolism of nucleotides results in the formation of uric acid, which is a rather insoluble nitrogenous waste (bird ‘pee’ – the white stuff). - Uric acid is filtered out of the blood by the kidneys for excretion. - If too much uric acid is in the blood, it may precipitate out, most commonly in joints (known as gout), less commonly in the urinary tract as a kidney stone. Creatine Phosphate Metabolism - creatine phosphate is a ‘donator’ molecule that ‘donates’ a phosphate group to ADP (adensine diphosphate), within skeletal muscle cells only, in order to re-create ATP; this serves to speed up the production of ATP in muscles (where ATP is needed quickly and in larger quantities during exercise/stressful times). - Once creatine phosphate has given up its phosphate, it is known as creatinine – a nitrogenous waste that is filtered out of the blood by the kidneys. • Urea (and some ammonia), uric acid, and creatinine are all nitrogenous wastes that exist in urine. • Urine is produced within the kidneys (the kidneys essentially filter the blood) for expulsion from the body. • The composition of urine is as follows: – 95% water; 5% solids/dissolved substances • Solids/Dissolved substances include (per 500 mL urine): - 10 g urea - 0.33-0.67 g creatinine - 0.33 g uric acid - 8-9 g of the following: Na+, K+, Ca2+, Mg2+, NH4+ (a combination of H+ and NH3), SO42-, PO43-, HCO3- varying levels of toxins, drugs, antibiotics, histamines. Anatomy of the Urinary System (fig. 16.1 p. 304) • All organs and blood vessels of the urinary system work to maintain a constant internal environment (ie. they work to maintain homeostasis) with respect to water-salt balance, pH balance, and nitrogenous waste management. • The kidneys are paired, kidney bean-shaped organs that exist on either side of the spinal cord, just below the diaphragm; each kidney ~ the size of a fist. • They are protected from the front and back in the following manners: – BACK: they lie against the back muscles in depressions (‘caves’) within the muscles; – FRONT: they are protected by the lower ribcage. • Kidneys are suspended within their back muscle depressions by connective tissue known as renal fascia, which can easily be broken by a blow to the back resulting in a ‘floating’ kidney. • Kidneys serve to produce urine, whereas other urinary structures serve to transport, store, and eliminate (excrete) urine. • Blood carrying dissolved wastes enters each kidney on its concave side (called the hilium) via the renal artery; even though the kidneys comprise only 1% of the mass of a human body, they receive about 20% of the blood pumped with each heartbeat. • The blood is essentially filtered by the kidneys as it flows through a series of arterioles, capillaries, and venules. • Blood eventually exits the kidneys via the renal vein. • Urine, the product of the filtering by the kidneys (ie. the waste fluid), exits the organs through paired ducts known as ureters. • Ureters are narrow, muscular tubes that carry urine to its storage area, the urinary bladder, by peristalsis. • The urinary bladder is a muscular organ that expands as urine enters it; it can store up to 600 mL of urine due to its distensible (‘stretchy’) walls. • At ~250 mL, one gets the urge to urinate; at ~500 mL, it becomes uncomfortable; eventually, the urge can be lost if the bladder is stretched too much. • The urinary bladder also houses special stretch receptors that send sensory impulses to the spinal cord (reflex), which sends motor impulses back to the bladder signaling it to contract. • So why don’t we ‘pee our pants’ when this occurs? • The brain plays a role as well – there is a voluntary ‘holding’ of your urine that may occur (not in babies as they have not developed the ability to do so). • Urine that leaves the bladder enters the urethra, which is the final tube it passes through before leaving the body; the passage of urine from the bladder to the urethra is mitigated by two musclecontrolled sphincters. • The first sphincter is under parasympathetic, involuntary control (spinal cord/reflex control) and is relaxed when the bladder contracts (ie. we have no choice in the matter). • The second sphincter is under the conscious, voluntary, somatic control of the brain; this is how one can ‘hold their pee’. • See fig. 16.2 p. 305 • The urethra extends from the bladder to the exterior opening known as the external urethral orifice. • The urethra is ~4 cm long in females, and ~20 cm long in males (this is why females are more susceptible to urinary tract infections (bacterial)). Read ‘Health Focus’ on p. 306. • The prostate gland encircles the urethra in men and can cause a restriction of urination if it becomes enlarged. FEMALE URETHRA MALE URETHRA Effects of Aging upon Urinary System • Reduced blood supply to kidneys – less filtering of blood. • On top of that, the kidney become less efficient with respect to the filtering process. • Poorer salt-water/pH balance – dehydration more evident in the elderly. • Bladder control adversely affected. • In men, the prostate may enlarge and apply pressure to the urethra making urination difficult (surgery required). Kidneys • When a kidney is sliced lengthwise, it is evident that the renal artery, the renal vein, and the ureter all enter/exit the kidney at the hilium (fig. 16.3a p.307). • The longitudinal section also provides one with a glimpse into the three major regions (layers) of a kidney: the renal cortex, renal medulla, and renal pelvis (fig. 16.3b p. 307). • The renal cortex is the outer, overlying, protective layer that houses an ECF with a relatively low osmotic pressure. • The renal medulla is the inner, ‘fan-shaped’ layer that houses an ECF with a relatively high osmotic pressure; this region consists of multiple cone-shaped tissue masses called renal pyramids, which serve to collect and drain urine into the third region, the renal pelvis – the innermost cavity that collects urine and allows it to drain into a ureter • On a ‘micro’ scale, a kidney is composed of ~ one million nephrons, which are urine-producing ‘factories’ in and of themselves. • Each nephron serves to produce a tiny bit of urine, which eventually drains into the renal pelvis. • Each nephron possesses structures that exist in the renal cortex or the renal medulla. In fact, the collecting ducts of nephrons (the ‘final’ tubules of nephrons) are responsible for the ‘fan-shaped’ appearance of the renal pyramids in the medullar region of the kidneys. Nephron Structure (fig. 16.4 p. 308) TWO MAJOR PARTS: Blood Vessels and Urinary Tract; keep in mind, as well, the existence of ECF between these two major parts). Blood Vessels - The renal arteries are the vessels carrying blood to the kidneys (to be filtered and to provide O2 and nutrients to the kidney cells). - A renal artery splits into ~ one million afferent arterioles, each of which carry blood to a nephron. - An afferent arteriole carries blood to the first nephronal capillary bed known as the glomerulus, a ‘knot-like’ ball of capillary vessels located in the Bowman’s (Glomerular) Capsule of the nephron. • Some filtering occurs here, then blood leaves the glomerulus and enters an efferent arteriole, which carries blood to the second nephronal capillary bed called the peritubular capillary network (the efferent arteriole is another example of a portal system as it connects two capillary beds). • This network surrounds the majority of the nephron like a spider’s web – more filtering occurs here. • Blood then flows into a renal venule, and eventually the renal vein, where its composition is quite different from what it was in the renal artery. In fact, blood in the renal vein is hypotonic compared to blood in the renal artery (due to the filtering that occurs between the glomerulus/peritubular network and the ECF/Urinary tract). The Urinary Tract - The nephron is really a tube (with a lumen) that acts to receive and process material from the blood. - It consists of several parts: Bowman’s (Glomerular) Capsule, Proximal Convoluted Tubule, Loop of Henle (Loop of the Nephron), Distal Convoluted Tubule, and Collecting Duct. - Bowman’s Capsule: - a ‘goblet-like’ structure found at the blind end of the nephron. - Outer layer comprised of protective epithelial cells; inner layer comprised of special cells called podocytes, which integrate with the glomerulus to form pores (‘slits’) that allow for simple size-based filtration to occur between the glomerulus and Bowman’s Capsule. Proximal Convoluted Tubule (PCT): - Comprised of special epithelial cells that possess microvilli, which form a ‘brush border’ that serves to increase the SA for the tubular reabsorption that occurs here (microvilli collect materials from lumen of tubule and allow entrance to epithelial cells, which perform tubular reabsorption). Fig. 16.5 p. 309 - This reabsorption process (described later) is an active one requiring ATP and carrier proteins. Thus, a plethora of mitochondria exist within each epithelial cell of the proximal convoluted tubule. *both the Bowman’s Capsule and the PCT exist in the renal cortex of the kidney. Loop of Henle: - Begins in the renal cortex, dips deep into the renal medulla, and returns (due to a hairpin turn at its base) to the cortex. - Thus, the loop is discussed in two parts, its descending arm and its ascending arm as they both have distinctly different structures/functions. - Both ‘arms’ possess a thin-walled and a thick-walled portion whose effects will be discussed during urine formation (fig. 16.7 p. 312). Distal Convoluted Tubule (DCT): - Lined by epithelial cells (this time, no microvilli) that possess many mitochondria for active transport during a process known as tubular secretion. - Here, substances tend to actively move from the blood into the DCT for excretion. - More tubular reabsorption occurs here as well. - Exists solely within the renal cortex. - Unlike most diagrams of the nephron, the DCT actually neighbours the afferent arteriole (ie. they touch) at a region known as the juxtaglomerular apparatus (fig. 16.8 p. 313). Such a ‘twisting back’ of the nephron allows each nephron to be skinnier so that a million can exist within a kidney. Collecting Duct: - The nephron’s last urinary structure is the collecting duct, which dives back into the renal medulla region of the kidney. - Comprised of epithelial cells that are permeable to water but not to salts. - Several DCTs drain into one collecting duct (~ 200-300 collecting ducts per kidney – why you see ‘branches’ coming off of the coll. duct in pictures). - Each collecting duct drains ‘collected’ urine into the renal pelvis for eventual expulsion from the body. - The collecting duct does not have the capillary network as close to it as the other nephron structures do. The material that it releases enter the ECF and contribute to the higher than normal osmotic pressure that exists in the renal medulla.