Document
advertisement

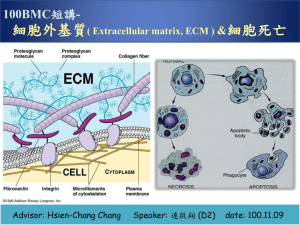
Clinical and Molecular Characterization of Collagen VI Myopathies Russell Butterfield MD/PhD University of Utah Departments of Neurology and Pediatrics August 15, 2010 Collagen VI myopathies Bethlem Myopathy Proximal muscle weakness and atrophy Dynamic contractures in distal joints (fingers, wrists, elbows, and ankles) Onset in first or second decade Slowly progressive in adult years Ullrich Congenital Muscular Dystrophy 2/3 of patients >50 years-old require assistance for ambulation Severe weakness/hypotonia in early infancy Proximal joint contractures Distal joint hyperlaxity Collagen VI myopathies likely represent spectrum of phenotypes defined by type and distribution of contractures Three genes of Collagen VI N1 TH C1 C2 a1(VI) C a2(VI) •C N10 N9 N8 N7 N6 N5 N4 N3 N2 N1 TH C1 C2 C3 C4 C5 a3(VI) C von Willebrand factor A domain Alternatively spliced vWF A Triple-helix Lysine/proline repeats Fibronectin type III motif Kunitz protease inhibitor motif COL6A1- 4246 base pairs gctctcactctggctgggagcagaaggcagcctcggtctctgggcggcggcggcggccca ctctgccctggccgcgctgtgtggtgaccgcaggccccagacatgagggcggcccgtgct ctgctgcccctgctgctgcaggcctgctggacagccgcgcaggatgagccggagaccccg agggccgtggccttccaggactgccccgtggacctgttctttgtgctggacacctctgag agcgtggccctgaggctgaagccctacggggccctcgtggacaaagtcaagtccttcacc aagcgcttcatcgacaacctgagggacaggtactaccgctgtgaccgaaacctggtgtgg aacgcaggcgcgctgcactacagtgacgaggtggagatcatccaaggcctcacgcgcatg cctggcggccgcgacgcactcaaaagcagcgtggacgcggtcaagtactttgggaagggc acctacaccgactgcgctatcaagaaggggctggagcagctcctcgtggggggctcccac ctgaaggagaataagtacctgattgtggtgaccgacgggcaccccctggagggctacaag gaaccctgtggggggctggaggatgctgtgaacgaggccaagcacctgggcgtcaaagtc ttctcggtggccatcacacccgaccacctggagccgcgtctgagcatcatcgccacggac cacacgtaccggcgcaacttcacggcggctgactggggccagagccgcgacgcagaggag gccatcagccagaccatcgacaccatcgtggacatgatcaaaaataacgtggagcaagtg tgctgctccttcgaatgccagcctgcaagaggacctccggggctccggggcgaccccggc tttgagggagaacgaggcaagccggggctcccaggagagaagggagaagccggagatcct ggaagacccggggacctcggacctgttgggtaccagggaatgaagggagaaaaagggagc cgtggggagaagggctccaggggacccaagggctacaagggagagaagggcaagcgtggc atcgacggggtggacggcgtgaagggggagatggggtacccaggcctgccaggctgcaag ggctcgcccgggtttgacggcattcaaggaccccctggccccaagggagaccccggtgcc tttggactgaaaggagaaaagggcgagcctggagctgacggggaggcggggagaccaggg agctcgggaccatctggagacgagggccagccgggagagcctgggccccccggagagaaa ggagaggcgggcgacgaggggaacccaggacctgacggtgcccccggggagcggggtggc cctggagagagaggaccacgggggaccccaggcacgcggggaccaagaggagaccctggt gaagctggcccgcagggtgatcagggaagagaaggccccgttggtgtccctggagacccg ggcgaggctggccctatcggacctaaaggctaccgaggcgatgagggtcccccagggtcc gagggtgccagaggagccccaggacctgccggaccccctggagacccggggctgatgggt gaaaggggagaagacggccccgctggaaatggcaccgagggcttccccggcttccccggg tatccgggcaacaggggcgctcccgggataaacggcacgaagggctaccccggcctcaag ggggacgagggagaagccggggaccccggagacgataacaacgacattgcaccccgagga gtcaaaggagcaaaggggtaccggggtcccgagggcccccagggacccccaggacaccaa ggaccgcctgggccggacgaatgcgagattttggacatcatcatgaaaatgtgctcttgc tgtgaatgcaagtgcggccccatcgacctcctgttcgtgctggacagctcagagagcatt ggcctgcagaacttcgagattgccaaggacttcgtcgtcaaggtcatcgaccggctgagc cgggacgagctggtcaagttcgagccagggcagtcgtacgcgggtgtggtgcagtacagc cacagccagatgcaggagcacgtgagcctgcgcagccccagcatccggaacgtgcaggag ctcaaggaagccatcaagagcctgcagtggatggcgggcggcaccttcacgggggaggcc ctgcagtacacgcgggaccagctgctgccgcccagcccgaacaaccgcatcgccctggtc atcactgacgggcgctcagacactcagagggacaccacaccgctcaacgtgctctgcagc cccggcatccaggtggtctccgtgggcatcaaagacgtgtttgacttcatcccaggctca gaccagctcaatgtcatttcttgccaaggcctggcaccatcccagggccggcccggcctc tcgctggtcaaggagaactatgcagagctgctggaggatgccttcctgaagaatgtcacc gcccagatctgcatagacaagaagtgtccagattacacctgccccatcacgttctcctcc ccggctgacatcaccatcctgctggacggctccgccagcgtgggcagccacaactttgac accaccaagcgcttcgccaagcgcctggccgagcgcttcctcacagcgggcaggacggac cccgcccacgacgtgcgggtggcggtggtgcagtacagcggcacgggccagcagcgccca gagcgggcgtcgctgcagttcctgcagaactacacggccctggccagtgccgtcgatgcc atggactttatcaacgacgccaccgacgtcaacgatgccctgggctatgtgacccgcttc taccgcgaggcctcgtccggcgctgccaagaagaggctgctgctcttctcagatggcaac tcgcagggcgccacgcccgctgccatcgagaaggccgtgcaggaagcccagcgggcaggc atcgagatcttcgtggtggtcgtgggccgccaggtgaatgagccccacatccgcgtcctg gtcaccggcaagacggccgagtacgacgtggcctacggcgagagccacctgttccgtgtc cccagctaccaggccctgctccgcggtgtcttccaccagacagtctccaggaaggtggcg ctgggctagcccaccctgcacgccggcaccaaaccctgtcctcccacccctccccactca tcactaaacagagtaaaatgtgatgcgaattttcccgaccaacctgattcgctagatttt ttttaaggaaaagcttggaaagccaggacacaacgctgctgcctgctttgtgcagggtcc tccggggctcagccctgagttggcatcacctgcgcagggccctctggggctcagccctga gctagtgtcacctgcacagggccctctgaggctcagccctgagctggcgtcacctgtgca gggccctctggggctcagccctgagctggcctcacctgggttccccaccccgggctctcc tgccctgccctcctgcccgccctccctcctgcctgcgcagctccttccctaggcacctct gtgctgcatcccaccagcctgagcaagacgccctctcggggcctgtgccgcactagcctc cctctcctctgtccccatagctggtttttcccaccaatcctcacctaacagttactttac aattaaactcaaagcaagctcttctcctcagcttggggcagccattggcctctgtctcgt tttgggaaaccaaggtcaggaggccgttgcagacataaatctcggcgactcggccccgtc tcctgagggtcctgctggtgaccggcctggaccttggccctacagccctggaggccgctg ctgaccagcactgaccccgacctcagagagtactcgcaggggcgctggctgcactcaaga ccctcgagattaacggtgctaaccccgtctgctcctccctcccgcagagactggggcctg gactggacatgagagccccttggtgccacagagggctgtgtcttactagaaacaacgcaa acctctccttcctcagaatagtgatgtgttcgacgttttatcaaaggccccctttctatg ttcatgttagttttgctccttctgtgtttttttctgaaccatatccatgttgctgacttt tccaaataaaggttttcactcctctaaaaaaaaaaaaaaaaaaaaa Where are we now in collagen VI myopathies? Collagen VI disorders are increasingly recognized Clinical spectrum expanding Progression/prognosis are not well defined No specific treatments Likely among the most common muscular dystrophies/myopathies Treatments in development based on correction of abnormal mitochondrial function Outcome measures for potential clinical studies are not well defined How do we measure success of a particular therapy? Where are we in genetics of Collagen VI Dominant and recessive inheritance has been described for both BM and UCMD Most mutations identified are specific to a single person/family Variant vs. mutation is often unclear Consistent genotype/phenotype correlations lacking Collagen VI at the University of Utah CLIA certified genetic testing has been available at the Utah Genome Center since 2006 To date, testing has been completed almost 400 patients. Since patient samples are sent without clinical data we do not know the clinical history of these patients Natural history and genotype/phenotype project Re-contacting all patients who have had genetic testing for collagen VI to collect detailed clinical data allowing correlation with the genotype data already obtained. United Dystrophinopathy Project Multi-centered natural history and genotype/phenotype study Now >1000 participants from 7 participating centers Children's Hospital of Philadelphia, Philadelphia, PA University of Minnesota, Minneapolis, MN Nationwide Children's Hospital, Columbus, OH University of Iowa, Iowa City, Iowa University of Utah, Salt Lake City, UT Washington University, St. Louis, MO University of California, Davis, Sacramento, California Patients are seen on yearly basis Confirmation of genetic diagnosis 390 clinical samples genotyped 86 Parent/sib carrier testing 39 positive 47 negative 304 Full sequencing of COL6A1,2,3 141 patients with no mutation detected 163 patients with variant detected Of 163 with variant detected: 91 probably pathogenic, 72 unknown significance Muscle Patient Genes COL6A Collagen VI myopathy study at Utah Catalog detailed clinical and genetic data in patients with Collagen VI myopathies Clarify breadth of potential phenotypes Detail natural history (progression over time) Improve accuracy of genetic diagnosis and prognosis Define genotype/phenotype relationships Stimulate development of potential therapies Provide a resource for investigators conducting clinical trials Well defined cohorts Appropriate outcome measures Improved understanding of molecular pathogenesis Facilitate collaboration among investigators, families, and others Integration with CMDIR Establishment of collaborations leaders in the field Patient Recruitment Primary recruitment from Utah Genome Center since Jan 2010 Goal is to re-contact patients for whom we have completed sequencing to collect clinical data Over 400 patients with genetic testing since 2006 with 50 enrolled thus far Primary contact is through referring physician Anticipated expansion of enrollment to include any patient with collagen VI myopathy diagnosis Summer 2010 Enrollment/Participation All patients with collagen VI myopathy phenotypes (ie. Bethlem myopathy or Ullrich CMD) are eligible to enroll A clinic visit is not required for participation Participants will fill out a short questionnaire detailing symptoms and physical findings We will request records from treating physicians including results of genetic testing (if done outside UGC) and other diagnostic tests In some cases, we may request a sample from skin or muscle biopsy if they are already in existence A couple areas of interest in our lab Mutation negative collagen VI patients 46% patients with no identifiable mutation Potential explanations: Deletion mutation not identifiable by sequencing from genomic DNA Mutation in non-coding regulatory region Allelic locus or secondary collagen VI defect Non-collagen VI disorder Defining pathogenicity (or non-pathogenicity) “variants” Some of these with decreased collagen VI on muscle or skin biopsy 163/304 samples with sequencing of all 3 COL6A genes identified variant 72 of these (44%) are of uncertain pathogenicity High throughput genomics—transcriptome, exome sequencing Acknowledgements Utah Genome Center, Robert Weiss, Director Kathryn Swoboda Weiss lab: Diane Dunn, Brett Duval Swoboda group: Lahdan Heidarian Funding: Muscular Dystrophy Association NIH-Loan Repayment Program Primary Children’ Foundation, CHRC Collaborators Kevin Flanigan-Nationwide Children’s Carsten Bönnemann-CHOP Thank you to CureCMD for the opportunity to participate in this conference.