SPECIAL REPORT
Dutch guidance for the treatment of
chronic hepatitis C virus infection in
a new therapeutic era
F.A.C. Berden1, W. Kievit2, L.C. Baak3, C.M. Bakker4, U. Beuers5, C.A.B. Boucher6, J.T. Brouwer7,
D.M. Burger8, K.J.L van Erpecum9, B. van Hoek10, A.I.M. Hoepelman11, P. Honkoop12,
M.J. Kerbert-Dreteler13, R.J de Knegt14, G.H. Koek15, C.M.J. van Nieuwkerk16, H. van Soest17,
A.C.I.T.L. Tan18, J.M. Vrolijk19, J.P.H. Drenth1*
Departments of 1Gastroenterology and Hepatology and 2Health Evidence, Radboud University
Medical Centre, Nijmegen, the Netherlands, 3Department of Gastroenterology and Hepatology,
Onze Lieve Vrouwe Gasthuis, the Netherlands, 4Department of Internal Medicine, Gastroenterology
and Hepatology, Atrium Medical Centre, the Netherlands, 5Department of Gastroenterology and
Hepatology, Academic Medical Centre Amsterdam, the Netherlands, 6Department of Virology, Erasmus
Medical Centre Rotterdam, the Netherlands, 7Department of Internal Medicine, Gastroenterology
and Hepatology, Reinier de Graaf Group, Delft, the Netherlands, 8Department of Pharmacy, Radboud
University Medical Centre, Nijmegen, the Netherlands, 9Department of Gastroenterology and
Hepatology, University Medical Centre Utrecht, the Netherlands, 10Department of Gastroenterology
and Hepatology, Leiden University Medical Centre, the Netherlands, 11Department of Internal Medicine
and Infectious Diseases, University Medical Center Utrecht, the Netherlands, on behalf of the Dutch
Society of Internal Medicine, 12Department of Gastroenterology and Hepatology, Albert Schweizer
Hospital, the Netherlands, 13Department of Gastroenterology and Hepatology, Medisch Spectrum
Twente, the Netherlands, 14Department of Gastroenterology and Hepatology, Erasmus Medical Centre
Rotterdam, the Netherlands, 15Department of Internal Medicine, division of Gastroenterology and
Hepatology, Maastricht University Medical Centre, the Netherlands, 16Department of Gastroenterology
and Hepatology, VU University Medical Centre, the Netherlands, 17Department of Gastroenterology
and Hepatology, Medical Centre Haaglanden, the Netherlands, 18Department of Gastroenterology and
Hepatology, Canisius Wilhelmina Hospital, the Netherlands, 19Department of Gastroenterology and
Hepatology, Rijnstate Hospital, the Netherlands, *corresponding author: tel.: +31 (0)24 3619190, e-mail:
joostphdrenth@cs.com or joost.drenth@radboudumc.nl
ABSTR ACT
Background: A new era for the treatment of chronic
hepatitis C is about to transpire. With the introduction
of the first-generation protease inhibitors the efficacy of
hepatitis C treatment improved significantly. Since then,
the therapeutic agenda has moved further forward with
the recent approval of sofosbuvir and the expected approval
of agents such as simeprevir and daclatasvir. This paper,
developed parallel to the approval of sofosbuvir, is to serve
as a guidance for the therapeutic management of chronic
hepatitis C.
Methods: We performed a formal search through PubMed,
Web of Science and ClinicalTrials.gov to identify all clinical
trials that have been conducted with EMA-approved
new agents in hepatitis C; for this version (April 2014)
we focused on sofosbuvir. For each disease category, the
evidence was reviewed and recommendations are based
on GRADE.
Results: We identified 11 clinical trials with sofosbuvir
and for each disease category recommendations for
treatment are made. Not all disease categories were studied
extensively and therefore in some cases we were unable to
provide recommendations.
Conclusion: The recent approval of sofosbuvir will most
likely change the therapeutic landscape of chronic hepatitis
© Van Zuiden Communications B.V. All rights reserved.
O C TOBER 2014, VOL . 7 2 , NO 8
388
C. The use of sofosbuvir-containing regimens can shorten
the duration of therapy, increase efficacy and result in less
side effects, compared with standard of care. The efficacy
relative to standard of care needs to be weighed against
the increased costs of sofosbuvir. With future approval of
the other direct-acting antivirals, the outcome of hepatitis
C treatment will likely improve further and this guidance
will be updated.
(NVMDL) or the Netherlands Association of Internal
Medicine (NIV).12
METHODS
We performed a formal search through the databases
PubMed, Web of Science and ClinicalTrials.gov to identify
all relevant clinical trials performed with sofosbuvir,
peginterferon and/or ribavirin for this version (April
2014). In addition we searched for future therapies and for
the product characteristics provided by the US Food and
Drug Administration (FDA) and the European Medicines
Agency (EMA). Opinions, letters, narrative reviews,
pre-clinical studies and articles in another language
than English, Dutch or German were excluded. The
search string is attached in supplementary file 1. We
limited the search for patients with HCV mono-infection.
For each disease category (treatment-naive, treatmentexperienced and cirrhotic patients) the evidence was
reviewed by the first and second author. The treatmentexperienced category consists of patients with a prior
relapse, prior partial response or prior null response.
Sustained virological response (SVR) is defined as an
HCV RNA below the lower limit of quantification at 12
weeks after the end of treatment. We listed the results
of all individual trials in tables according to disease
category. The level of evidence was formulated based on
the GRADE method with the quality of evidence and a
strength of recommendation (supplementary file 2).13 The
recommendations in this paper went through a formal
approval process and were vetted by individual experts and
all members of the NVMDL and representatives of the NIV.
K EY WOR DS
Direct-acting antivirals, guidance, hepatitis C, sofosbuvir
INTRODUCTION
The recent approval of sofosbuvir (NS5B polymerase
inhibitor) and the expected approval of other direct-acting
antivirals (DAAs) such as simeprevir (protease
inhibitor) and daclatasvir (NS5A inhibitor) will change
the therapeutic arena for chronic hepatitis C.1 Until
2012 the treatment of chronic hepatitis C consisted of
pegylated interferon with ribavirin (PR) for 24 to 48
weeks.2 As of April 2012 two first-generation protease
inhibitors, telaprevir and boceprevir, were approved for
reimbursement in the Netherlands for patients infected
with hepatitis C virus (HCV) genotype 1.3 These agents
improved efficacy 3 but their safety profile was poor,
especially in cirrhotic patients. 4-6
In the Netherlands, the estimated hepatitis C
seroprevalence is 0.1-0.4%, and the highest prevalence
is seen in first-generation migrants from HCV-endemic
countries.7-9 Approximately 50% of Dutch patients are
infected with genotype 1, 30% with genotype 3, 10% with
genotype 2 and 10% with genotype 4.10
Sofosbuvir can be regarded as a game changer;1 it is an
orally administered nucleotide polymerase inhibitor, has
pangenotypic activity in vivo, a high barrier to resistance
and an acceptable safety profile.11 Approval of other
drugs in different classes of DAAs may be expected,
first of all simeprevir (during revision approved) and
daclatasvir. Additional drugs belonging to the protease
inhibitor class (asunaprevir, ABT -450/r), the NS5A class
(ledipasvir, ombitasvir) and the non-nucleoside polymerase
inhibitor class (dasabuvir) are in later stages of clinical
development.1
This paper may serve as a current guidance for the
therapeutic management of chronic hepatitis C. This
update of the earlier guidance3 is necessary given the
wealth of new information that has become available since.
As a static version will become outdated, we encourage
to review the most current version on the websites of the
Netherlands Association of Hepato-gastroenterologists
R ESULTS
We formulated recommendations on the basis of the
available evidence and information from the label of
sofosbuvir. The recommendations are given for each
disease category. When no recommendation is given,
treatment can be deferred or we refer to the earlier
guideline.3 First, all currently approved agents and
expected agents are listed, followed by recommended
treatment options for the different HCV genotypes once
sofosbuvir is approved. Recommendations are valid for all
patients with an indication for treatment as stipulated by
the earlier guideline.3
List of currently approved drugs for treatment of chronic
HCV infection:
• Peginterferon: polyethylene glycol attached to
interferon-_
- Peginterferon _ -2a: 180 +g/week
Berden et al. Treatment of chronic hepatitis C virus infection.
O C TOBER 2014, VOL . 7 2 , NO 8
389
•
•
•
- Peginterferon _ -2b: 1.5 +g/kg/week
Ribavirin: nucleoside analogue, weight-based dose (< 75
kg 1000 mg/day and ≥ 75 kg 1200 mg/day, divided over
two doses)
Protease inhibitors (-previr):
- Simeprevir (during revision approved, will be
included in updated version)
- Telaprevir: 2250 mg/day, divided over two or three
doses
- Boceprevir: 2400 mg/day, divided over three doses
Nucleotide polymerase inhibitor (-buvir):
- Sofosbuvir: 400 mg/day, in one dose
No data in patients with renal impairment are
available (eGFR < 30 ml/min/m2)
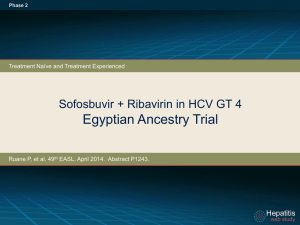
NEUTRINO trial was a single-group open-label trial that
achieved 89% SVR.14 Patients without cirrhosis obtained
90% SVR in the ATOMIC trial. There was no additional
benefit (i.e. no difference in SVR) for extension of treatment
to 24 weeks or by extension with sofosbuvir monotherapy or
sofosbuvir and ribavirin (n = 264).15 The dose of sofosbuvir
was determined on the basis of the PROTON study where
200 and 400 mg of sofosbuvir were compared. Here, the
SVR rate was irrespective of the dose of sofosbuvir; however,
three patients in the 200 mg group had a viral breakthrough,
hence the selection of 400 mg.16 Only one trial was of high
quality,16 the other trials were open-label trials of a low to
moderate quality.13
Genotype 1 treatment-experienced patients
Recommendation: No recommendation based on data
List of HCV drugs in development:
This list is not exhaustive and can be expanded; we aimed
to include drugs that are in phase III development.1
• Protease inhibitors (-previr):
- Asunaprevir
- Faldaprevir
- ABT-450/r (ritonavir-boosted)
- MK-5172
• NS5A inhibitors (-asvir):
- Daclatasvir
- Ledipasvir
- Ombitasvir (ABT-267)
- MK-8742
• Non-nucleoside polymerase inhibitors (-buvir):
- Dasabuvir (ABT-333)
The ELECTRON trial was the only trial that included
treatment-experienced genotype 1 patients; these patients
received sofosbuvir with ribavirin (12 weeks), only one
of ten patients achieved SVR.17 The label recommends
consideration of treatment with sofosbuvir, peginterferon
and ribavirin for 12 weeks or extension to 24 weeks,18 but
in our opinion more data are needed.
Genotype 1 cirrhotic patients
Recommendation: Watchful waiting (Level: C1)
Two clinical trials included patients with cirrhosis; the
NEUTRINO trial reached 80% SVR with sofosbuvir on top
of PR14 and three of six cirrhotic patients with unfavourable
characteristics achieved SVR with sofosbuvir and ribavirin
in a single-centre trial.19 The quality of evidence for
sofosbuvir is low, the toxicity of the previous standard of
care in cirrhotic patients is high 4 and future agents (e.g.
simeprevir) are promising, hence watchful waiting is
recommended.
Watchful waiting
Watchful waiting is a preferred strategy in patients who do
not have an urgent indication for treatment based on the
earlier guideline,3 in patients where no recommendation
is given or when the quality of evidence is low and the
strength of recommendation is weak (Level: C2). There
are several arguments in favour of this strategy: (A) not all
patient groups are represented in clinical trials, therefore
the evidence for recommendations is weak in certain
disease categories, (B) with the introduction of sofosbuvir
we still need pegylated interferon and ribavirin in many
patients and (C) improved efficacy and reduced toxicity is
expected from interferon-free combinations of DAAs likely
to be approved in the near future.1
Future perspective
For genotype 1 patients, multiple trials are currently
underway; promising agents are simeprevir,
asunaprevir, ABT-450/r (protease inhibitors), daclatasvir,
ledipasvir, ombitasvir (NS5A inhibitors) and dasabuvir
(non-nucleoside polymerase inhibitor). All oral treatment
is expected to become possible in the near future for both
treatment-naive and treatment-experienced patients.
Simeprevir and sofosbuvir with or without ribavirin were
studied in the COSMOS trial in two cohorts, in prior null
responders with F0-2 fibrosis (cohort 1) and in treatment
naive or prior null responders with F3-4 fibrosis (cohort
2). High SVR rates were seen in cohort 1 (91-100%)20 and
cohort 2 (94-96%).21,22 Therefore the combined treatment
of simeprevir and sofosbuvir can be a reasonable option for
these categories of patients in the near future. Simeprevir
with PR has been studied in the ASPIRE, PILLAR and
PROMISE studies and high SVR rates of 70-85% are seen
Recommendations by HCV genotype, disease stage and
treatment history
Genotype 1 treatment-naive patients
Recommendation: Sofosbuvir, peginterferon and
weight-based ribavirin for 12 weeks (Level: B1)
Several trials have been performed in genotype 1
treatment-naive patients (figure 1). The recommended therapy
was studied in two trials: NEUTRINO and ATOMIC. The
Berden et al. Treatment of chronic hepatitis C virus infection.
O C TOBER 2014, VOL . 7 2 , NO 8
390
Figure 1. Trials in HCV genotype 1 patients
Trial
Regime (weeks)
0
4
8
n
12
24
//
SVR
48
SVR (95% CI)
0
50
QoE
100
Genotype 1, treatment naive
PROTON
SOF(200)+PR
PR
PR
48
90%
A
SOF(400)+PR
PR
PR
47
91%
A
26
58%
A
placebo + PR
PR
NEUTRINO
SOF+PR
292
89%
C
ELECTRON
SOF(+RBV)
25
84%
C
SOF+PR
52
90%
B
109
93%
B
155
91%
B
SOF+RBV(wb)
10
90%
C
SOF+RBV(wb)
25
68%
C
SOF+RBV(600)
25
48%
C
SOF+RBV
10
10%
C
SOF+PR
54 †
80%
C
SOF+RBV(wb)
6†
50%
C
SOF+RBV(600)
7†
29%
C
ATOMIC
SOF+PR
SOF+PR
Osinusi et al. 0
SOF(+RBV)
Genotype 1, treatment experienced
ELECTRON
Genotype 1, cirrhosis
NEUTRINO
Osinusi et al.*0
PR = pegylated interferon with ribavirin; QoE = Quality of Evidence (A: high, B: moderate, C: low); RBV = ribavirin; SOF = sofosbuvir;
SVR = sustained virological response; wb: weight-based; *calculated 95% CI, 0 first cohort early-moderate fibrosis; second and third cohort
unfavourable characteristics. In cirrhotics: †treatment naive.
ION-1, ION-2 and ION-3 studies. The LONESTAR is a
single-centre open-label study in genotype 1 treatment-naive
patients and patients with virological failure on protease
inhibitors. An SVR of 95-100% (n = 100) with different
regimens (i.e. sofosbuvir/ledipasvir with or without
ribavirin, 8 or 12 weeks) was reached.28 In the ION-1
and ION-2 trials, SVR was reached in 94-98% of the
patients with 12 weeks of sofosbuvir/ledipasvir with or
without ribavirin.29,30 In the ION-3 trial treatment-naive
non-cirrhotic patients achieved 94% SVR with 8 weeks of
sofosbuvir/ledipasvir.31 Phase 2a trials have been performed
with daclatasvir and asunaprevir in combination with PR
or the non-nucleoside polymerase inhibitor BMS-791325 in
prior null responders and treatment-naive patients for 12-24
weeks. High SVR rates, 92-100%, were achieved.32-34 Three
in cirrhotic patients with prior relapse or prior partial
response.23-25 Clinical trials with simeprevir have shown
that a Q80K mutation in genotype 1a patients significantly
reduces the efficacy of the treatment.26
Sofosbuvir plus daclatasvir with or without ribavirin for
12 or 24 weeks was studied in the AI444040 study, 126
treatment-naive genotype 1 patients achieved 98% SVR.
Furthermore 41 patients who failed therapy with telaprevir
or boceprevir had 98% SVR with 24 weeks of sofosbuvir
and daclatasvir with or without ribavirin. Cirrhotic patients
were excluded.27 Currently a compassionate use program
of sofosbuvir and daclatasvir with or without ribavirin for
Child-Pugh C patients is available.
The combination of an NS5B polymerase inhibitor and an
NS5A inhibitor is also being studied in the LONESTAR,
Berden et al. Treatment of chronic hepatitis C virus infection.
O C TOBER 2014, VOL . 7 2 , NO 8
391
Genotype 2 cirrhotic patients
Recommendation: Sofosbuvir and weight-based ribavirin
for 12 weeks (Level: B1)
studies (n = 571, n = 297 and n = 473) evaluated multiple
regimens with ABT-450/r, dasabuvir and ombitasvir with or
without ribavirin in different combinations and durations.
High SVR rates (83-97%) were seen in treatment-naive
and treatment-experienced non-cirrhotic patients.35-37 The
TURQUOISE-II trial studied the same regimen (with
ribavirin) in compensated cirrhotic patients for 12 (n = 208)
and 24 (n = 172) weeks. SVR was achieved in 92% and 96%
of the patients, respectively.38
There are four trials that evaluated sofosbuvir and ribavirin
for 12 weeks in cirrhotic genotype 2 patients, mainly
treatment-naive patients were studied. The FISSION
demonstrated an SVR of 83% (n = 12), treatment with
peginterferon and ribavirin (800 mg) for 24 weeks led to
62% SVR (n = 13).14,18 The POSITRON trial showed an SVR
of 94%. In treatment-experienced patients with cirrhosis
an extension of duration of treatment from 12 to 16 weeks
led to an improvement in SVR from 60% (n = 10) to 78%
(n = 9) in the FUSION trial.11 The VALENCE trial shows
82% SVR in 11 cirrhotic patients with sofosbuvir and
ribavirin (12 weeks).18,44 All trials included only a small
number of patients, but implications for clinical practice
are high as treatment is warranted and toxicity is expected
to be less than with standard of care.
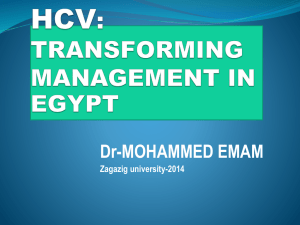
Genotype 2 treatment-naive patients
Recommendation: Sofosbuvir and weight-based ribavirin
for 12 weeks (Level: A1)
Patients with an HCV genotype 2 infection have an SVR
rate of 74-83% with PR for 24 weeks.3,39,40 Multiple trials
with sofosbuvir have been performed in treatment-naive
genotype 2 patients ( figure 2). Two trials of high quality
and one of low quality studied the recommended
interferon-free regimen (POSITRON, FISSION and
VALENCE) with consistent good results. The POSITRON
trial included patients for whom interferon was not an
option and reached 93% SVR irrespective of cirrhosis.11
In the FISSION trial SVR was reached in 97% of patients,
while in patients treated with peginterferon and ribavirin
(800 mg) for 24 weeks SVR was achieved in 78%.14 The
results of the VALENCE trial are similar to FISSION and
POSITRON for the recommended regimen. 41,42 Addition
of peginterferon showed no improved SVR rates.16,17 In
conclusion, sofosbuvir with ribavirin for 12 weeks in
genotype 2 patients was effective in high-quality trials
with implications for clinical practice because of an
interferon-free regimen with a shorter treatment duration
than the previous standard of care.3
Future perspective
For genotype 2 patients the regimen of sofosbuvir with
ribavirin leads to high SVR rates. Also, the AI444040
trial studied 26 treatment-naive genotype 2 patients; 24
(92%) achieved SVR with different regimens consisting of
sofosbuvir and daclatasvir with or without ribavirin for 24
weeks. Cirrhotic patients were excluded.27
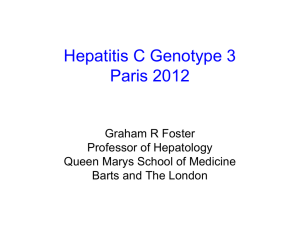
Genotype 3 treatment-naive patients
Recommendation:
•
•
•
•
Watchful waiting
Peginterferon and ribavirin (800 mg) for 24 weeks
Sofosbuvir and weight-based ribavirin for 24 weeks
Sofosbuvir, peginterferon and weight-based ribavirin for
12 weeks
(Level A2)
Genotype 2 treatment-experienced patients
Recommendation: Sofosbuvir and weight-based ribavirin
for 12 weeks (Level: B1)
For genotype 3 patients, several options for treatment are
available and the physician has to decide which strategy
is currently better for the individual patient. Historically
genotype 2 and genotype 3 patients achieve an SVR of
70-80% with peginterferon and ribavirin (800 mg) for
24 weeks.3
Different trials have been performed in genotype 3
patients; all trials with 12 weeks of sofosbuvir and
ribavirin fail to show superiority in comparison with
PR treatment ( figure 3).14 The addition of peginterferon
or extension of treatment to 24 weeks showed improved
results. In the ELECTRON trial, 25 patients received
12 weeks of sofosbuvir and ribavirin combined with
peginterferon for 0, 4, 8 or 12 weeks: all patients achieved
SVR.17 The VALENCE trial obtained 94% SVR in 105
patients with sofosbuvir with ribavirin for 24 weeks.18,42
Because of the above-mentioned results peginterferon
with ribavirin (800 mg) for 24 weeks remains an option
for therapy, ribavirin should be weight based in patients
In the FUSION trial, genotype 2 patients were treated with
either 12 or 16 weeks of sofosbuvir and ribavirin. Patients
in the 12-week arm received four weeks of placebo, they
reached 86% SVR and in the 16-week arm this was 94%.
For non-cirrhotic patients the FUSION trial failed to
demonstrate additional value of extending the treatment
to 16 weeks, hence the recommendation of 12 weeks.11
The POSITRON included 17 patients with unacceptable
side effects in prior treatment and they achieved an SVR
of 78% with sofosbuvir and ribavirin.11 The results of
the VALENCE trial demonstrated a 90% SVR with the
recommended regimen.18,42 In another trial there was no
additional value of peginterferon. 43 Again this treatment
has significant implications for clinical practice because
of the high SVR rates without interferon and shorter
treatment duration. The trials were of high11 and low
quality41,43 with consistent results.
Berden et al. Treatment of chronic hepatitis C virus infection.
O C TOBER 2014, VOL . 7 2 , NO 8
392
Figure 2. Trials in HCV genotype 2 patients
Trial
Regime (weeks)
0
4
8
n
12
24
//
SVR
48
SVR (95% CI)
0
50
QoE
100
Genotype 2, treatment naive
POSITRON
FISSION
SOF+RBV
109
93%
A
Placebo
34
0%
A
SOF+RBV
70
97%
A
67
78%
A
SOF+PR
25 #
92%
B
SOF+(P)R
40 #
100%
B
SOF+PR
10 #
100%
B
SOF
10 #
60%
B
SOF+RBV
32
97%
C
36
86%
A
32
94%
A
SOF+RBV
17 #
77%
A
Placebo
8#
0%
A
SOF+RBV
41
90%
C
SOF+PR
23
96%
C
SOF+RBV
17 †
94%
A
Placebo
13 †#
0%
A
SOF+RBV
49 †#
47%
A
50 †#
38%
A
SOF+RBV
2†
100%
C
SOF+RBV
9‡
78%
C
SOF+RBV
10 ‡
60%
A
SOF+RBV
9‡
78%
A
SOF+PR
14 ‡
93%
C
PR (RBV 800)
PROTON
ELECTRON
VALENCE
Genotype 2, treatment experienced
FUSION
SOF+RBV
SOF+RBV
POSITRON
VALENCE
LONESTAR-2*
Genotype 2, cirrhosis
POSITRON*
FISSION
PR (RBV 800)
VALENCE
FUSION
LONESTAR-2*
PR = pegylated interferon with ribavirin; QoE = Quality of Evidence (A: high, B: moderate, C: low); RBV = ribavirin; SOF = sofosbuvir;
SVR = sustained virological response; *calculated 95% CI, # data of genotype 2 and 3 combined. In cirrhotics: † treatment naive, ‡ treatment
experienced.
Berden et al. Treatment of chronic hepatitis C virus infection.
O C TOBER 2014, VOL . 7 2 , NO 8
393
with baseline characteristics associated with a poor
response.3 Other options are watchful waiting, sofosbuvir
with ribavirin for 24 weeks or sofosbuvir with PR for 12
weeks. The choice for one of the regimens is dependent on
the individual patient, bearing in mind the higher costs
of sofosbuvir.
weeks placebo with PR. SVR rates were 69% (12 weeks),
67% (16 weeks) and 59% (placebo). Treatment failure was
mainly due to relapse in cirrhotic patients in the 12-week
group. 45 The combination of sofosbuvir and daclatasvir
with or without ribavirin for 24 weeks does hold promise
for treatment-naive genotype 3 patients as SVR rates of
89% can be reached.27 Treatment-naive genotype 3 patients
received sofosbuvir/ledipasvir with or without ribavirin in
the ELECTRON-2 trial (12 weeks). Dual therapy reached
64% SVR (n=25) while triple therapy reached 100% SVR
(n=26). 46
Genotype 3 treatment-experienced patients
Recommendation: Watchful waiting
Alternative strategy: Sofosbuvir and weight-based
ribavirin for 24 weeks OR sofosbuvir, peginterferon and
weight-based ribavirin for 12 weeks (Level: B2)
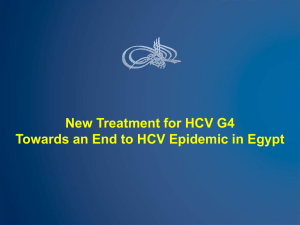
Genotype 4 treatment-naive patients
Recommendation: Sofosbuvir, peginterferon and
weight-based ribavirin for 12 weeks. (Level: C1)
Results of sofosbuvir for treatment-experienced genotype
3 patients are disappointing with high imprecision; only
the VALENCE and LONESTAR-2 trials show acceptable
results but are of low quality. The FUSION trial showed
that extension of treatment by 4 weeks led to improvement
of SVR.11 Extension to 24 weeks was done in the VALENCE
study and an SVR of 79% was achieved, while for the
non-cirrhotic patients the SVR rate was 87%.18,42 The
LONESTAR-2 trial showed an SVR of 83% in 24 patients
treated with sofosbuvir and PR for 12 weeks. 43 In the
near future more effective combinations of DAAs are
expected. Therefore, the general recommendation is
watchful waiting. As an alternative strategy sofosbuvir with
ribavirin for 24 weeks or sofosbuvir with PR for 12 weeks
may be considered.
The recommended regimen is being studied in the
NEUTRINO trial, 28 patients were treated with sofosbuvir
and PR for 12 weeks and reached 96% SVR.14 Extension
of therapy to 24 weeks did not show an improved effect.15
Egyptian patients (n = 28) received an interferon-free
regimen for 12 or 24 weeks and achieved 79% and 100%
SVR, respectively. 47 In general, data are scarce ( figure 4) but
in view of the high SVR rates sofosbuvir-based treatment
is recommended.
Genotype 3 cirrhotic patients
Recommendation: Watchful waiting
Alternative strategy: Sofosbuvir and weight-based
ribavirin for 16 weeks OR sofosbuvir and weight-based
ribavirin for 24 weeks (Level: B2)
There are no published data on sofosbuvir-based treatment
available for treatment-experienced genotype 4 patients.
The most recent data of the Egyptian study showed 59%
SVR (n = 17) with 12 weeks of sofosbuvir and ribavirin
and 87% SVR (n = 15) with 24 weeks of sofosbuvir and
ribavirin. 47,48 The label recommends sofosbuvir and PR for
12 weeks, but more data are needed.
Genotype 4 treatment-experienced patients
Recommendation: No recommendation based on data
Genotype 3 cirrhotic patients were treated with sofosbuvir
in five trials with moderate SVR rates.
The FUSION trial showed an SVR of 19% with 12 weeks of
sofosbuvir and ribavirin in treatment-experienced cirrhotic
patients; extension of treatment to 16 weeks showed an
SVR of 61%. The VALENCE trial studied 24 weeks of
sofosbuvir and ribavirin in 60 cirrhotic patients, with 92%
SVR in treatment-naive patients and 62% in treatmentexperienced patients.18
Based on the above results with small numbers of patients,
we advise watchful waiting as the recommended strategy
since SVR rates are rather low, mainly in treatmentexperienced patients and sofosbuvir is expensive.
Alternative regimens are sofosbuvir and ribavirin for 16
weeks or 24 weeks.
Genotype 4 cirrhotic patients
Recommendation: No recommendation based on data
Only a limited number of cirrhotic genotype 4 patients
have been studied. The NEUTRINO trial included two
cirrhotic genotype 4 patients of whom one achieved SVR
with sofosbuvir and PR for 12 weeks.14 In the Egyptian
study treatment-naive cirrhotic patients achieved 33%
(n = 3) and 100% (n = 3) SVR with 12 and 24 weeks of
sofosbuvir and ribavirin. The SVR rates in treatmentexperienced patients were 50% and 100% in both groups
(n = 8). 47
Future perspective
Simeprevir with PR (24 or 48 weeks) is studied in genotype
4 patients, overall 65% of the patients reached SVR with
higher SVR rates in treatment-naive and relapse patients
(83% and 86%). 49 Asunaprevir with PR has been studied
in 18 genotype 4 patients for 24 weeks and 89% reached
SVR, the control group consisted of seven patients of whom
Future perspective
Daclatasvir is one of the agents that are expected to be
approved in the near future. The COMMAND GT 2/3 study
included 151 genotype 2 and 3 patients and these patients
received either 12 or 16 weeks of daclatasvir with PR or 24
Berden et al. Treatment of chronic hepatitis C virus infection.
O C TOBER 2014, VOL . 7 2 , NO 8
394
Figure 3. Trials in HCV genotype 3 patients
Trial
Regime (weeks)
0
4
8
n
12
24
//
SVR
48
SVR (95% CI)
0
50
QoE
100
Genotype 3, treatment naive
POSITRON
FISSION
SOF+RBV
98
61%
A
Placebo
37
0%
A
SOF+RBV
183
56%
A
176
63%
A
SOF+PR
25 #
92%
B
SOF+(P)R
40 #
100%
B
10 #
100%
B
SOF
10 #
60%
B
SOF+RBV
11
27%
C
105
94%
C
64
30%
A
63
62%
A
SOF+RBV
17 #
77%
B
Placebo
8#
0%
B
145
79%
C
SOF+PR
24
83%
C
SOF+RBV
14 †
21%
A
Placebo
13 #†
0%
A
SOF+RBV
49 # †
47%
A
PR (RBV 800)
50 # †
38%
A
SOF+RBV
13 †
92%
C
SOF+RBV
47 ‡
62%
C
26 ‡
19%
A
SOF+RBV
23 ‡
61%
A
SOF+PR
12 ‡
83%
C
PR (RBV 800)
PROTON
ELECTRON
SOF+PR
VALENCE
SOF+RBV
Genotype 3, treatment experienced
FUSION
SOF+RBV
SOF+RBV
POSITRON
VALENCE
LONESTAR-2*
SOF+RBV
Genotype 3, cirrhosis
POSITRON*
FISSION
VALENCE
FUSION
LONESTAR-2*
SOF+RBV
PR = pegylated interferon with ribavirin; QoE = Quality of Evidence (A: high, B: moderate, C: low); RBV = ribavirin; SOF = sofosbuvir;
SVR = sustained virological response; *calculated 95% CI, # data of genotype 2 and 3 combined. In cirrhotics: † treatment naive, ‡ treatment
experienced.
Berden et al. Treatment of chronic hepatitis C virus infection.
O C TOBER 2014, VOL . 7 2 , NO 8
395
Genotype 5, 6
43% reached SVR with PR for 48 weeks.50 Furthermore
daclatasvir was studied in 24 treatment-naive genotype 4
patients, 67% achieved SVR with 20 mg daclatasvir and
100% achieved SVR with 60 mg daclatasvir with PR for
24 weeks.51 Daclatasvir with asunaprevir and BMS-791325
were studied in 12 patients, 11 achieved SVR and 1
patient is still in follow-up.52 The PEARL-I study included
86 treatment-naive genotype 4 patients who received
ABT-450/r plus ombitasvir with or without ribavirin (12
weeks), 91-100% SVR was achieved.53 Patient numbers are
limited but in view of the high SVR rates of future therapy,
watchful waiting can be considered in genotype 4 patients
until further data allow approval of newer DAAs.
Data from well-powered clinical comparative trials for
genotype 5 and 6 patients are lacking. We think it is
unlikely that such data will become available in the
near future for the novel DAAs. Therefore we consider
it acceptable to use treatment results for genotype 1 as a
template for treatment of genotype 5 and 6.
Genotype 5, 6 treatment-naive patients
Recommendation:
•
Genotype 5: No recommendation based on data, consider
genotype 1 treatment regimen as template (Level: C2)
Figure 4. Trials in HCV genotype 4, 5 and 6 patients
Trial
Regime (weeks)
0
4
8
n
12
24
//
SVR
48
SVR (95% CI)
0
50
QoE
100
Genotype 4, treatment naive
NEUTRINO*
SOF+PR
ATOMIC
Ruane et al.*
SOF+PR
SOF+RBV
SOF+RBV
28
96%
C
11
82%
C
14
79%
C
14
100%
C
17
59%
C
15
87%
C
Genotype 4, treatment experienced
Ruane et al.*
SOF+RBV
SOF+RBV
Genotype 4, cirrhosis
NEUTRINO*
SOF+PR
2†
50%
C
Ruane et al. *
SOF+RBV
3†
33%
C
SOF+RBV
4‡
50%
C
SOF+RBV
3†
100%
C
SOF+RBV
4‡
100%
C
7
100%
C
5
100%
C
Genotype 5 and 6, treatment naive
NEUTRINO*
ATOMIC
SOF+PR
SOF+PR
Genotype 5 and 6, treatment experienced
No available trials
PR = pegylated interferon with ribavirin; QoE = Quality of Evidence (A: high, B: moderate, C: low); RBV = ribavirin; SOF = sofosbuvir;
SVR = sustained virological response; *calculated 95% CI, if 100% SVR then no CI could be calculated. In cirrhotics: † treatment naive, ‡ treatment
experienced.
Berden et al. Treatment of chronic hepatitis C virus infection.
O C TOBER 2014, VOL . 7 2 , NO 8
396
Genotype 5, 6 cirrhotic patients
Recommendation: No recommendation based on data,
consider genotype 1 treatment regimen as template
(Level: C2)
•
Genotype 6: sofosbuvir, peginterferon and weight-based
ribavirin for 12 weeks (Level: C2)
Only 12 treatment-naive patients with genotype 5 or 6 have
been treated in two trials (NEUTRINO and ATOMIC).
In the NEUTRINO trial six genotype 6 patients and one
genotype 5 patient were treated with 12 weeks of sofosbuvir
and PR and all patients achieved SVR.14 In the ATOMIC
trial only five patients with genotype 6 received sofosbuvir
with PR for 24 weeks, all achieved SVR.15 More data
are needed, however, considering the high SVR rates a
sofosbuvir-based treatment is recommended for genotype 6.
The NEUTRINO trial included 20% cirrhotic patients but
it is unknown if cirrhotic genotype 5 or 6 patients were
included.14
Drug-drug interactions
Many of the DAAs are substrates of CYP450 and the
membrane transporter P-gp; they may both be the victim
of drug interactions or cause these interactions with other
agents.54,55 Sofosbuvir has a relatively mild drug interaction
profile as it is only a substrate of P-gp and does not
interfere with CYP450 enzymes. It is necessary to check
for interacting co-medications, including over the counter
drugs (e.g. St. John’s Wort), before starting DAA-based
HCV treatment (http://www.hep-druginteractions.org).
Genotype 5,6 treatment-experienced patients
Recommendation: No recommendation based on data,
consider genotype 1 treatment regimen as template
(Level: C2)
There are no data on sofosbuvir-based treatment available
for treatment-experienced genotype 5 or 6 patients.
Summary box of recommendations for HCV monoinfected patients
Genotype
Patient group
Recommendation
Future perspective
1
Treatment naive
Sofosbuvir, peginterferon and ribavirin for 12 weeks
Daclatasvir, simeprevir, ledipasvir,
asunaprevir, ABT-450/r, dasabuvir,
ombitasvir
2
3
4
5, 6
Treatment experienced
No recommendation based on data
Cirrhotic
Watchful waiting
Treatment naive
Sofosbuvir and ribavirin for 12 weeks
Treatment experienced
Sofosbuvir and ribavirin for 12 weeks
Cirrhotic
Sofosbuvir and ribavirin for 12 weeks
Treatment naive
Physician opinion to determine the strategy, options:
• Watchful waiting
• Peginterferon and ribavirin (800 mg) for 24 weeks
• Sofosbuvir and ribavirin for 24 weeks
• Sofosbuvir, peginterferon and ribavirin for 12 weeks
Treatment experienced
Watchful waiting
Alternative strategy:
• Sofosbuvir and ribavirin for 24 weeks OR
• Sofosbuvir, peginterferon and ribavirin for 12 weeks
Cirrhotic
Watchful waiting
Alternative strategy:
• Sofosbuvir and ribavirin for 16 weeks OR
• Sofosbuvir and ribavirin for 24 weeks
Treatment naïve
Sofosbuvir, peginterferon and ribavirin for 12 weeks
Treatment experienced
No recommendation based on data
Cirrhotic
No recommendation based on data
Treatment naive
Genotype 5: No recommendation based on data,
consider genotype 1 treatment regimen as template
Genotype 6: Sofosbuvir, peginterferon and ribavirin
for 12 weeks
Treatment experienced
No recommendation based on data, consider genotype
1 treatment regimen as template
Cirrhotic
No recommendation based on data, consider genotype
1 treatment regimen as template
Berden et al. Treatment of chronic hepatitis C virus infection.
O C TOBER 2014, VOL . 7 2 , NO 8
397
Daclatasvir
Daclatasvir, ledipasvir
Simeprevir, daclatasvir,
asunaprevir, ABT-450/r, ombitasvir
DISCUSSION
DISCLOSUR ES
The current guidance comes at a time when the landscape
of HCV treatment is undergoing a rapid change. There
are currently four comparable guidances, one was issued
by the American Association for the Study of Liver
Diseases (AASLD), one by European Association for the
Study of the Liver (EASL) and the other two are guidances
from Germany.56-59 Our guidance differs from the AASLD
and EASL guidances and we do not offer advice on the
use of simeprevir and daclatasvir in this version. The
main difference with the other guidances is that we offer
the clinician the option to defer treatment in genotype
3 and some subgroups of patients. The reason is that,
except for the VALENCE trial, the currently published
evidence has not proved efficacy beyond standard of care.
The proportion of cirrhotic patients in the various trials
is disappointingly low and recommendations cannot be
given for this category, with the exception of genotype
2. This contrasts with clinical practice where cirrhotic
patients have the most urgent treatment indication.3
For genotypes 5 and 6 the current evidence is poor.
The AASLD, EASL and German guidances recommend
sofosbuvir triple therapy for genotype 5 and 6. The
consensus in the Hepatology Committee was that the
evidence for sofosbuvir was acceptable for genotype 6
naive patients, while we recommend standard of care or
considering the genotype 1 regimen as template for other
disease categories in genotype 5 and 6. At odds with
other guidances we do not recommend sofosbuvir-based
treatment for genotype 1 and 4 treatment-experienced
patients given the lack of evidence. This guidance only
includes recommendations for HCV monoinfected
patients. Sofosbuvir and other DAAs are also being
studied in HIV/HCV patients; this will be updated in a
new version of this guidance.
The rapid pace of development of drugs to treat HCV
infection introduces not only great expectations but also
uncertainty about the optimal timing to initiate therapy.60
The key question here is which patients can benefit
from the DAAs that are now available. Sofosbuvir is
a first-generation polymerase inhibitor that is in the
vanguard of a wave of drugs that have the potential to
cure HCV. With the approval of the EMA, sofosbuvir will
be released on the Dutch market soon. As medication is
an important costdriver, the added efficacy of sofosbuvir
relative to standard of care should be weighed carefully.61
As the pipeline with new antiviral drugs is full and new
releases can be expected in 2014 and 2015, this paper
serves as a dynamic document and will be continually
edited and updated.12
Conflicts of interest
F.A.C. Berden: none
W. Kievit: none
L.C. Baak: was a member of the advisory board and/or
received speakers fees from Gilead, Janssen, AbbVie and
Bristol-Myers Squibb
C.M. Bakker: none
U.H.W. Beuers: consulting on behalf of Academic Medical
Centre: Intercept, Novartis; speaking and teaching: Falk
Foundation, Gilead, Intercept, Roche, Zambon
C.A. Boucher: received a research grant from MSD, is a
consultant on behalf of Erasmus MC for MSD and AbbVie,
received a travel grant from Gilead and is scientific director
of Virology Education
J.T. Brouwer: was a member of the advisory board of MSD,
Gilead, AbbVie, Janssen and Bristol-Myers Squibb; received
a travel grant from MSD and Gilead
D.M. Burger: received research grants from Janssen, Merck
and Roche; was a member of the advisory board of Janssen
and Merck and received speakers fees from Janssen,
Merck, AbbVie and Gilead
K.J.L. van Erpecum: served in the advisory boards of
AbbVie and Bristol-Myers Squibb and received previous
funding for research from BMS and MSD
B. van Hoek: was a member of the advisory board of
Gilead, Janssen and AbbVie; received a travel grant from
Gilead and was sponsored for post-academic education by
Dr. Falk, Gilead, Janssen, Abbvie, Roche and Astellas
A.I.M. Hoepelman: was a member of the advisory boards
of Janssen, Abbvie, MSD, Gilead and BMS; received
research grants from Gilead and ViiV
P. Honkoop: none
M.J. Kerbert-Dreteler: none
R.J de Knegt: received research grants from AbbVie,
Bristol-Myers Squibb, Gilead, Roche and Janssen-Cilag,
was a member of the advisory board of AbbVie,
Bristol-Myers Squibb, Merck, Gilead and Janssen-Cilag,
received speakers fees from Merck, Gilead, Norgine and
Janssen-Cilag
G.H. Koek: none
K.M.J. van Nieuwkerk: was a member of the advisory
boards of Gilead, Abbvie, MSD, Janssen
H. van Soest: was a member of the advisory board of
Bristol-Myers Squibb, AbbVie, Janssen and MSD
A.C.I.T.L. Tan: none
J.M. Vrolijk: none
J.P.H. Drenth: served on the advisory boards of AbbVie,
BMS and Gilead; served as a consultant for Gilead; his
department receives research funding from Dr. Falk,
AbbVie, Ipsen, Novartis and Zambon.
Berden et al. Treatment of chronic hepatitis C virus infection.
O C TOBER 2014, VOL . 7 2 , NO 8
398
Supplementary file 1. Search
An initial search was conducted on 25-Feb-2014 with the term:
‘2-((5-(2,4-dioxo-3,4-dihydro-2H-pyrimidin-1-yl)-4-fluoro3-hydroxy-4-methyltetrahydrofuran-2-ylmethoxy)phenoxyphosphorylamino) propionic acid isopropyl ester [Supplementary
Concept]’ as a MeSH term. Furthermore we included ‘sofosbuvir OR GS-7977 OR PSI 7977 OR PSI7977 OR PSI-7977
OR Sovaldi’ in our search. In total 98 articles were found in
PubMed. All were scanned on title and abstract for inclusion.
New results of the search were added until 8-Apr-14. For the
future perspectives we searched the agents in phase III of
clinical trials, including simeprevir (as MeSH combined with
‘simeprevir OR TMC 435350 OR TMC435350 OR TMC-435350
OR Olysio OR TMC 435 OR TMC435 OR TMC-435’, with the
limit of clinical trials). We did the same for daclatasvir, ledipasvir, asunaprevir and the ABT formulations in PubMed.
Clinicaltrials.gov was used to get more information about the
unpublished trials. Prior to submission, the abstracts of the
International Liver Congress 2014 (49th annual meeting of the
European Association for the Study of the Liver) were scanned
and relevant studies were included in the future perspectives of
the different genotypes.
8.
Vriend HJ, Van Veen MG, Prins M, Urbanus AT, Boot HJ, Op De Coul EL.
Hepatitis C virus prevalence in The Netherlands: migrants account for
most infections. Epidemiol Infect. 2013;141:1310-7.
9.
Slavenburg S, Verduyn-Lunel FM, Hermsen JT, Melchers WJ, te Morsche
RH, Drenth JP. Prevalence of hepatitis C in the general population in the
Netherlands. Neth J Med. 2008;66:13-7.
10. de Vries MJ, te Rijdt B, van Nieuwkerk CM. Genotype distribution
amongst hepatitis C patients in the Netherlands. Neth J Med.
2006;64:109-13.
11. Jacobson IM, Gordon SC, Kowdley KV, et al. Sofosbuvir for hepatitis C
genotype 2 or 3 in patients without treatment options. N Engl J Med.
2013;368:1867-77.
12. www.mdl.nl and www.internisten.nl.
13. Guyatt G, Oxman AD, Akl EA, et al. GRADE guidances: 1.
Introduction-GRADE evidence profiles and summary of findings tables. J
Clin Epidemiol. 2011;64:383-94.
14. Lawitz E, Mangia A, Wyles D, et al. Sofosbuvir for previously untreated
chronic hepatitis C infection. N Engl J Med. 2013;368:1878-87.
15. Kowdley KV, Lawitz E, Crespo I, et al. Sofosbuvir with pegylated interferon
alfa-2a and ribavirin for treatment-naive patients with hepatitis C
genotype-1 infection (ATOMIC): an open-label, randomised, multicentre
phase 2 trial. Lancet. 2013;381:2100-7.
16. Lawitz E, Lalezari JP, Hassanein T, et al. Sofosbuvir in combination with
peginterferon alfa-2a and ribavirin for non-cirrhotic, treatment-naive
patients with genotypes 1, 2, and 3 hepatitis C infection: a randomised,
double-blind, phase 2 trial. Lancet Infect Dis. 2013;13:401-8.
Supplementary file 2. Evidence grading (adapted from
the GRADE system)
17. Gane EJ, Stedman CA, Hyland RH, et al. Nucleotide polymerase inhibitor
sofosbuvir plus ribavirin for hepatitis C. N Engl J Med. 2013;368:34-44.
18. Summary of Product Characteristics Sovaldi EMA. 2014.
Level
Evidence quality
Strength of recommendation
A1
High
Strong
B1
Moderate
Strong
C1
Low
Strong
A2
High
Weak
B2
Moderate
Weak
C2
Low
Weak
19. Osinusi A, Meissner EG, Lee YJ, et al. Sofosbuvir and ribavirin for hepatitis
C genotype 1 in patients with unfavorable treatment characteristics: a
randomized clinical trial. JAMA. 2013;310:804-11.
20. Sulkowski M, Jacobson I, Ghalib RH, et al. Once-daily simeprevir (tmc435)
plus sofosbuvir (gs-7977) with or without ribavirin in hcv genotype 1 prior
null responders with metavir f0–2: cosmos study subgroup analysis. J
Hepatol. 2014;60:S4.
21. Lawitz E, Ghalib RH, Rodriguez-Torres M, et al. Simeprevir plus
sofosbuvir with/without ribavirin in hcv genotype 1 prior null-responder/
treatment-naive patients (cosmos study): primary endpoint (svr12) results
in patients with metavir f3–4 (cohort 2). J Hepatol. 2014;60:S524.
REFERENCES
22. Jacobson IM, Ghalib RH, Rodriguez-Torres M, et al. SVR results of a
once-daily regimen of simeprevir (TMC435) plus sofosbuvir (GS-7977)
with or without ribavirin in cirrhotic and non-cirrhotic HCV genotype 1
treatment-naive and prior null responder patients: The COSMOS study.
Hepatology. 2013;58:1379a-80a.
1.
23. Zeuzem S, Berg T, Gane E, et al. Simeprevir increases rate of sustained
virologic response among treatment-experienced patients with HCV
genotype-1 infection: a phase IIb trial. Gastroenterology. 2014;146:430-41.
2.
Marino Z, van Bommel F, Forns X, Berg T. New concepts of sofosbuvirbased treatment regimens in patients with hepatitis C. Gut.
2014;63:207-15.
24. Fried MW, Buti M, Dore GJ, et al. Once-daily simeprevir (TMC435) with
pegylated interferon and ribavirin in treatment-naive genotype 1 hepatitis
C: the randomized PILLAR study. Hepatology. 2013;58:1918-29.
Gevers TJ, Slavenburg S, van Oijen MG, Drenth JP. Treatment extension
benefits HCV genotype 1 patients without rapid virological response: a
systematic review. Neth J Med 2011;69:216-21.
3.
Lamers MH, Broekman MM, Boucher CA, et al. Treatment of hepatitis
C monoinfection in adults--Dutch national guidances. Neth J Med.
2013;71:377-85.
4.
Hezode C, Fontaine H, Dorival C, et al. Triple therapy in treatmentexperienced patients with HCV-cirrhosis in a multicentre cohort of the
French Early Access Programme (ANRS CO20-CUPIC) - NCT01514890.
J Hepatol. 2013;59:434-41.
25. Forns X, Lawitz E, Zeuzem S, et al. Simeprevir (tmc435) with
peginterferon/ribavirin for treatment of chronic hcv genotype 1 infection
in European patients who relapsed after previous interferon-based
therapy: the promise trial. J Hepatol. 2014;60:S6.
26. Schneider MD, Sarrazin C. Antiviral therapy of hepatitis C in 2014: do we
need resistance testing? Antiviral Res. 2014;105:64-71.
27. Sulkowski MS, Gardiner DF, Rodriguez-Torres M, et al. Daclatasvir plus
sofosbuvir for previously treated or untreated chronic HCV infection. N
Engl J Med. 2014;370:211-21.
5.
Bichoupan K, Schwartz JM, Martel-Laferriere V, et al. Effect of fibrosis on
adverse events in patients with hepatitis C treated with telaprevir. Aliment
Pharmacol Ther. 2014;39:209-16.
6.
Virlogeux V, Pradat P, Bailly F, et al. Boceprevir and telaprevir-based triple
therapy for chronic hepatitis C: virological efficacy and impact on kidney
function and model for end-stage liver disease score. J Viral Hepat.
2014;21:e98-e107.
29. Afdhal N, Zeuzem S, Kwo P, et al. Ledipasvir and Sofosbuvir for Untreated
HCV Genotype 1 Infection. N Engl J Med. 2014;370:1889-98.
Vriend HJ, Op de Coul EL, van de Laar TJ, Urbanus AT, van der Klis FR,
Boot HJ. Hepatitis C virus seroprevalence in the Netherlands. Eur J Public
Health. 2012;22:819-21.
30. Afdhal N, Reddy KR, Nelson DR, et al. Ledipasvir and Sofosbuvir
for Previously Treated HCV Genotype 1 Infection. N Engl J Med.
2014;370:1483-93.
7.
28. Lawitz E, Poordad FF, Pang PS, et al. Sofosbuvir and ledipasvir fixed-dose
combination with and without ribavirin in treatment-naive and previously
treated patients with genotype 1 hepatitis C virus infection (LONESTAR):
an open-label, randomised, phase 2 trial. Lancet. 2014;383:515-23.
Berden et al. Treatment of chronic hepatitis C virus infection.
O C TOBER 2014, VOL . 7 2 , NO 8
399
31. Kowdley KV, Gordon SC, Reddy KR, et al. Ledipasvir and Sofosbuvir
for 8 or 12 Weeks for Chronic HCV without Cirrhosis. N Engl J Med.
2014;370:1879-88.
51. Hezode C, Hirschfield GM, Ghesquiere W, et al. Daclatasvir, an NS5A
Replication Complex Inhibitor, Combined With Peginterferon Alfa-2a and
Ribavirin in Treatment-Naive HCV-Genotype 1 or 4 Subjects: Phase 2b
command-1 svr12 results. Hepatology. 2012;56:553a-4a.
32. Everson GT, Sims KD, Rodriguez-Torres M, et al. Efficacy of an
interferon- and ribavirin-free regimen of daclatasvir, asunaprevir, and
BMS-791325 in treatment-naive patients with HCV genotype 1 infection.
Gastroenterology. 2014;146:420-9.
52. Hassanein T, Sims K, Bennett M, et al. All-oral therapy with daclatasvir
in combination with asunaprevir and bms-791325 for treatment-naive
patients with chronic hcv genotype 4 infection J Hepatol. 2014;60:S472.
53. Hezode C, Marcellin P, Pol S, et al. Results from the phase 2 pearl-i study:
interferon-free regimens of abt-450/r + abt-267 with or without ribavirin in
patients with hcv genotype 4 infection. J Hepatol. 2014;60:S24.
33. Lok AS, Gardiner DF, Lawitz E, et al. Preliminary study of two antiviral
agents for hepatitis C genotype 1. N Engl J Med. 2012;366:216-24.
34. Lok AS, Gardiner DF, Hezode C, et al. Randomized trial of daclatasvir and
asunaprevir with or without PegIFN/RBV for hepatitis C virus genotype 1
null responders. J Hepatol. 2014;60:490-9.
54. Burger D, Back D, Buggisch P, et al. Clinical management of drug-drug
interactions in HCV therapy: challenges and solutions. J Hepatol.
2013;58:792-800.
35. Kowdley KV, Lawitz E, Poordad F, et al. Phase 2b trial of interferon-free
therapy for hepatitis C virus genotype 1. N Engl J Med. 2014;370:222-32.
55. http://www.hep-druginteractions.org University of Liverpool.
36. Zeuzem S, Jacobson IM, Baykal T, et al. Retreatment of HCV with
ABT-450/r-Ombitasvir and Dasabuvir with Ribavirin. N Engl J Med.
2014;370:1604-14.
56. Recommendations for Testing, Managing, and Treating Hepatitis C. 2014;
Available from: www.hcvguidances.org.
57. Sarrazin C, Buggisch P, Hinrichsen H, et al. Praxisempfehlung
zur Therapie der chronischen Hepatitis C nach Zulassung des
Polymerase-Inhibitors Sofosbuvir. Berufsverband Niedergelassener
Gastroenterologen Deutschlands e.V.; 2014; Available from: http://
www.gastromed-bng.de/tl_files/Aerzte%20News/140128EmpfehlungTherapieHCVnachZulassungSofosbuvir.pdf.
37. Feld JJ, Kowdley KV, Coakley E, et al. Treatment of HCV with
ABT-450/r-Ombitasvir and Dasabuvir with Ribavirin. N Engl J Med.
2014;370:1594-603.
38. Poordad F, Hezode C, Trinh R, et al. ABT-450/r-Ombitasvir and
Dasabuvir with Ribavirin for Hepatitis C with Cirrhosis. N Engl J Med.
2014;370:1973-82.
58. Sarrazin C, Berg T, Wedemeyer H, et al. Aktuelle Empfehlung der DGVS
zur Therapie der chronischen Hepatitis C. 2014.
39. Andriulli A, Mangia A, Iacobellis A, Ippolito A, Leandro G, Zeuzem S.
Meta-analysis: the outcome of anti-viral therapy in HCV genotype 2 and
genotype 3 infected patients with chronic hepatitis. Aliment Pharmacol
Ther. 2008;28:397-404.
59. Pawlotsky JM, Aghemo A, Dusheiko G, Forns X, Puoti M, Sarrazin C. EASL
Recommendations on Treatment of Hepatitis C 2014.
60. Drenth JP. HCV treatment--no more room for interferonologists? N Engl
J Med. 2013;368:1931-2.
40. Slavenburg S, Weggelaar I, van Oijen MG, Drenth JP. Optimal length of
antiviral therapy in patients with hepatitis C virus genotypes 2 and 3: a
meta-analysis. Antiviral Ther. 2009;14:1139-48.
61. Helsper CW, Hellinga HL, van Essen GA, et al. Real-life costs of hepatitis
C treatment. N Engl J Med. 2012;70:145-53.
41. Zeuzem S, Dusheiko GM, Salupere R, et al. Sofosbuvir plus Ribavirin for
12 or 24 Weeks for Patients with HCV Genotype 2 or 3: the VALENCE trial.
Hepatology. 2013;58:733a-4a.
42. Zeuzem S, Dusheiko GM, Salupere R, et al. Sofosbuvir and ribavirin in
HCV genotypes 2 and 3. N Engl J Med. 2014;370:1993-2001.
43. Lawitz E, Poordad F, Brainard DM, et al. Sofosbuvir in Combination
With PegIFN and Ribavirin for 12 Weeks Provides High SVR Rates in
HCV-Infected Genotype 2 or 3 Treatment-experienced patients with and
without Compensated Cirrhosis: Results from the LONESTAR-2 Study.
Hepatology. 2013;58(6):1380a-a.
44. Zeuzem S, Dusheiko GMD, Colombo M, et al. Early viral kinetics do
not predict treatment outcome with sofosbuvir + ribavirin for 12 or 24
weeks in HCV genotype 2/3 patients in the VALENCE trial. J Hepatol.
2014;60:S452.
45. Dore GJ, Lawitz E, Hezode C, et al. Twelve- or 16-Week Treatment With
Daclatasvir Combined With Peginterferon Alfa and Ribavirin for Hepatitis
C Virus Genotype 2 or 3 Infection: Command GT2/3 Study. Hepatology.
2012;56:558a-9a.
46. Gane E, Hyland RH, An D, al. Sofosbuvir/ledipasvir fixed dose
combination is safe and effective in difficult-to-treat populations
including genotype-3 patients, decompensated genotype-1 patients,
and genotype-1 patients with prior sofosbuvir treatment experience. J
Hepatol. 2014;60:S3.
47. Ruane PJ, Ain D, Meshrekey R, et al. Sofosbuvir plus ribavirin, an
interferon-free regimen, in the treatment of treatment-naive and
treatment-experienced patients with chronic genotype 4 hcv infection.
J Hepatol. 2014;60:S503.
48. Ruane PJ, Ain D, Riad J, et al. Sofosbuvir plus Ribavirin in the Treatment
of Chronic HCV Genotype 4 Infection in Patients of Egyptian Ancestry.
Hepatology. 2013;58:736a-a.
49. Moreno C, Hezode C, Marcellin P, et al. Once-daily simeprevir (tmc435)
with peginterferon/ribavirin in treatment-naive or treatment-experienced
chronic hcv genotype 4-infected patients: final results of a phase iii trial.
J Hepatol. 2014;60:S535.
50. Bronowicki JP, Ratziu V, Gadano A, et al. Asunaprevir with
Peginterferon-Alfa and Ribavirin in Treatment-Naive Patients with
Genotype-1 or-4 Chronic Hepatitis C: Svr24 Results from a Randomized
Phase 2b Study (Ai447016). J Hepatol. 2013;58:S571-S2.
Berden et al. Treatment of chronic hepatitis C virus infection.
O C TOBER 2014, VOL . 7 2 , NO 8
400