PAR LEC 6 HEM - neutralposture
advertisement

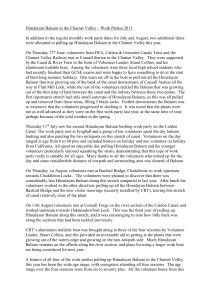
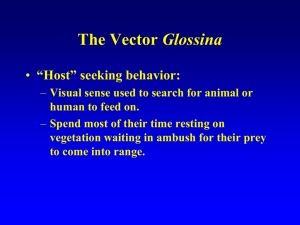
Trypanosomiasis Lecture with Dr. Balsam Mahdi Nasir MBBS/YEAR1/SEM2/2012 African trypanosomiasis (sleeping sickness) Definition: It is a vector-borne disease. Endemic to sub-Saharan Africa. It is caused by the single cell flagellate protozoan Trypanosoma brucei. Geographic distribution: Trypanasoma brucei gambiense (West African sleeping sickness or Gambian trypanasomiasis). • Trypanasoma brucei rhodesiense (East African sleeping sickness or Rhodesian trypanosomiasis). • 2 Dr. Balsam 4/13/2015 Geographic distribution 3 Dr. Balsam 4/13/2015 Mode of transmission Via the bite of an infected tsetse fly. • 4 Dr. Balsam 4/13/2015 Morphology In the vertebrate it exists as a TRYPOMASTIGOTE. Elongated rather flattened. Spindle shaped organism. Blunted posterior end. Finely pointed anterior end. Central large oval nucleus. Kinetoplast is small and is situated at the posterior end. Undulating membrane. Flagellum. 5 Dr. Balsam 4/13/2015 Blood forms 1. Trypomastigote (long slender)→ dividing form. 2.Trypomastigotes (short broad stumpy form with or without attenuated flagellum)→ non dividing form → infective to tsetse fly. 3. Intermediate form. 6 Dr. Balsam 4/13/2015 Tsetse fly procyclic trypomastigote Epimastigote Metacyclic trypomastigote Infective stage to human Human Trypomastigotes Short stumpy form Intermediate form Long slender form Infective stage to tsetse fly 7 4/13/2015 Life cycle 8 Dr. Balsam 4/13/2015 Life cycle Definitive host • Man, game and domestic animals. Intermediate host • Tsetse fly (both male & female flies) • Reservoir of infection • Man (Trypanosoma brucei gambiense)→West African trypanosomiasis. • Animals (Trypanosoma brucei rhodesience)→ East African trypanosomiasis. Infective stage to man • Metacyclic trypomastigotes 9 Dr. Balsam 4/13/2015 Pathogenesis and symptomatology Gambian disease of trypomastigotes. Bite of infected •• Inoculation Subcutaneous nodules→ 5-15 days → painless chancre→ resolve in 2-3 weeks. tsetse fly Incubation period Stage 1Blood dissemination Stage 1Lymphatics Stage 2 CNS invasion 10 • Asymptomatic • several weeks to months up to a year. • Intermittent fever pattern, chills, headache, myalgia, arthralgia..etc • Lymphadenopathy, especially in the posterior cervical nodes (on the back of the neck) →Winterbottom’s sign. • • Occur at the end of 1st year or the beginning of the 2nd year Daytime sleeping, mental dullness, apathy, tremors, convulsions and coma followed by death from asthenia during the 2nd or 3rd year Dr. .Balsam 4/13/2015 Winterbottoms sign 11 CDC DPDx Parasite Image Library Dr. Balsam 4/13/2015 RHODESIAN SLEEPING SICKNESS clinical features It is more acute than the Gambian form Incubation period 2-3 weeks 12 Fever, weakness, rapid loss of weight and myocarditis are the usual manifestation. Fatal within a year of onset before involvement of the CNS. Dr. Balsam Mania and delusion may occur but the typical sleeping sickness picture is seldom seen. 4/13/2015 A teenage girl in Uganda with sleeping sickness exhibiting the characteristic chancre on her leg at the site of tsetse fly inoculation (A), and a woman in Uganda with a partially healedchancre just above her elbow (B). Although (C) may look painful, chancres are generallypainless with some associated tenderness 13 Dr. Balsam 4/13/2015 A woman caring for her comatose husband who is dying of African trypanosomiasis, Uganda, 1990 14 Dr. Balsam 4/13/2015 Diagnosis Clinical Patient from endemic area, irregular fever, palpable lymph nodes (post. cervical). Chronic disease with somnolence, personality changes and neurological symptoms. Laboratory Direct microscopy of a wet smear of unstained blood or Geimsastained thick smear→ trypmastigote. Chancre, lymph node, bone marrow and CSF aspirate→ wet preparation. Culture methods The standard serologic assay to diagnose West African trypanosomiasis is the card agglutination test for trypanosomiasis (CATT). Serological tests ELISA. 15 Dr. Balsam 4/13/2015 Trypanosoma brucei 16 Dr. Balsam 4/13/2015 17 Dr. Balsam 4/13/2015 TREATMENT Haemo-lymphatic stage Suramine sodium→ Rhodesian disease. Suramine sodium or Pentamidine isethionate→ Gambian disease CNS involvement Melarsoprol → Rhodesian disease. Melarsoprol or DEMO (eflornithine) → Gambian disease. 18 Dr. Balsam 4/13/2015 PREVENTION AND CONTROL Elimination of the reservoir: Early Diagnosis and Treatment to reduce the reservoir of infection. Breaking the channel of transmission: Vector control. Protection of susceptible: Persons visiting endemic areas should wear protective clothing and apply repellents. 19 Dr. Balsam 4/13/2015 Chagas’ disease American trypanosomiasis Definition It is a vector-borne disease It is prevalent throughout South and Central America It is caused by the flagellate protozoan Trypanosoma cruzi. 20 Dr. Balsam 4/13/2015 Geographic distribution 21 Dr. Balsam 4/13/2015 • Mode of transmission Contamination of wound site, conjunctiva, or mucosa by infected feces of insect (reduviid bugs) 22 Dr. Balsam 4/13/2015 Morphology Trypomastigote The same as Trypanosoma brucei. Long thin form 2. Short stumpy form 3. In blood film they appear C or U or S shape. 1. Blood Amastigote form Oval bodies. Nucleus. Kinetoplast. Habitat: Striated muscle in heart, skeletal, neurological cells and cells of reticuloendothelial system. Tissue 23 Dr. Balsam 4/13/2015 Morphology 24 Dr. Balsam 4/13/2015 Trypomastigote Epimastigote Metacyclic trypomastigote Reduviid bug Human Trypomastigote 25 Amastigote Trypomastigote Dr. Balsam 4/13/2015 26 Dr. Balsam 4/13/2015 Life cycle Definitive host • Man, wild and domestic animals. Intermediate host • Triatomine bugs (reduviid bugs) Reservoir of infection Besides humans, the parasite infects a variety of wild and domestic animals. Infective stage to man • Metacyclic trypomastigotes 27 Dr. Balsam 4/13/2015 Clinical features Acute • In less than 50% of people bitten by a triatomine bug, characteristic first visible signs can be a skin lesion (chagoma ) or a purplish swelling of the lids of one eye (Romana sign) • After 1-2 weeks→ fever, headache, malaise, muscle pain, generalized lymphadenopathy and hepatosplenomegally. • Cardiac abnormalities followed by meningoencephalitis. 28 Chronic •The parasites are hidden mainly in the heart and digestive tract muscle. • Up to 30% of patients suffer from cardiac disorders. • Up to 10% suffer from digestive (megaesophagus or megacolon), neurological or mixed alterations. •In later years the infection can lead to sudden death or heart failure caused by progressive destruction of the heart muscle. 4/13/2015 Romana sign 29 Dr. Balsam 4/13/2015 Megacolon in patient with Chagas disease 30 Dr. Balsam 4/13/2015 Diagnosis Clinical may be suspected when general, cardiac or GIT symptoms are present in patients lived under low SES in endemic regions. Laboratory • Demonstration of the parasitic agent is the diagnostic procedure in acute Chagas'' disease. 1.Microscopic examination a) of fresh anticoagulated blood for detecting motile trypanosomes. b) of thin and thick blood smears stained with Giemsa for identification of parasites. 31 Dr. Balsam 4/13/2015 Trypanosoma cruzi amastigotes in heart tissue 32 Trypanosoma cruzi trypomastigote in a thin blood smear stained with Giemsa Dr. Balsam 4/13/2015 Laboratory diagnosis 2. If the parasites are scanty in blood Culture of the blood or suspected tissue specimen. xenodiagnosis, where clean lab-reared reduviid bugs are fed on the patient's blood, and their gut contents examined for parasites 4 weeks later. Demonstration of antibodies to T. cruzi are required to diagnose chronic Chagas disease by serology – complement-fixation, direct agglutination and indirect haemagglutinatin and ELISA. Treatment Nitrofurans and benzidazoles have been used in acute disease. Neither drug is expected to cure established chronic disease. It is unsatisfactory since the organisms are within cells in established infections. 34 Dr. Balsam 4/13/2015 Prevention and control Elimination of reservoirs: Control and elimination of domestic and peridomestic animals. Early diagnosis and treatment of infected cases. Vector control: Triatomine bugs are highly susceptible to chlorinated hydrocarbon insecticides which form the major weapon for their control. Protection of susceptible: Provision of better housing would prevent transmission because most human infections are transmitted by bugs living in cracks and crannies in the walls of ill kept tenement dwellings. 35 Dr. Balsam 4/13/2015