Food Fortification as
Public Health Policy
TH Tulchinsky MD MPH
Braun SPH
24 November 2013
1
2
WHO,
FAO
2006
3
Key Fortification issues
•
•
•
•
Iodine – cretinism, Iodine deficiency disorders (IDD)
Iron – iron deficincy and anemia
Vitamin B complex (B1, B2, B3, B6, B9, B12)
Vitamin D – rickets, osteoporosis, and linked with
many medical conditions
• Folic acid – pre pregnancy neural tube defects;
pregnancy macrocytic anemia
• Others – calcium, selenium, zinc
4
5
6
7
8
9
10
Essential Considerations
Micronutrient deficiency conditions widespread
Non mandatory enriched foods are costly and not
available to the poor e.g. bread, milk, yoghurts, salt
Public health and medical responsibility
WHO and best practices standards
Regulatory, monitoring and laboratory support are
governmental public health responsibilities
11
Public Health Nutrition Strategies
• Education
• Food based strategy
– Socio economic factors
– Food supply/costs
– Education
• Supplementation for target groups
– Women and children
– Elderly
• Fortification of basic foods
• Surveillance and monitoring
12
18-19th Century Breakthroughs
• James Lind and scurvy 1747
• Lemon juice mandatory in Royal Navy, 1796
• Humphrey Davy isolates sodium, potassium, calcium,
magnesium, sulphur, boron, 1807
• Chatin shows iodine prevents goiter, 1850
• Takaki and beriberi, Japanese Navy, 1885
• Eijkman publishes cause of beriberi, 1897 (Nobel
Prize 1929, anti-neuritic vitamin)
13
Vital Amines
• 1912, Funk defines vital amines
• Rickets, scurvy, goiter, beriberi common in
industrial countries
• Pellagra epidemic in southern US
• 1914, Goldberger of USPHS investigates
pellagra
• 1922, McCollum and vitamin D in cod liver
oil
14
Key Landmarks
• Iodized salt, 1924
• Louisiana - mandates vit B fortification of
flour to control pellagra epidemic, 1928
• US federal mandate - enrichment of flour with
vitamins B and iron, 1941
• Britain and colonies same during WWII
• Canada mandates fortification in 1979
• Folic acid found to prevent NTDs in 1990s
15
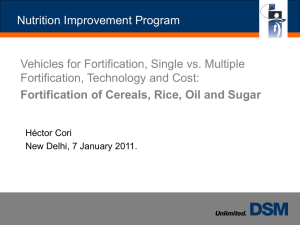
Low Cost Solutions to Eliminate
Micronutrient Malnutrition
U
.S
.Dollars
Annual Per Capita Cost of Interventions
Iron
Suppl.
Iron Fort.
Source: World Bank, 1994
Iodine
Suppl.
Iodine
Fort.
Vit A
Suppl.
World Bank 1994
Vit A
Fort.
16
Preventing Goiter and Iodine
Deficiency Disorders
• 1917 high % US draftees rejected - goiter
• 1922-27, goiter rates fall from 39% to 9% by
statewide prevention programs
• 1924 Morton’s Iodized Salt (N America)
• 1979 Iodization mandatory in Canada
• 1980s WHO - universal iodization of salt
• Most member countries achieved iodization
17
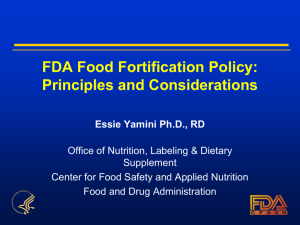
Percent
Iodine Fortification of Salt in the U.S.:
Trend in Goiter Prevalence in Michigan
Year
WHO Monograph
Series N. 44
18
Pellagra: The 4 Ds
• Diarrhea, dermatitis, dementia, death
• Thought to be of infectious origin
• Common in prisons, mental institutions,
sharecroppers in southern US
• Curable by dietary change (Goldberger)
• 1929, niacin found as essential factor
• 1906-1940, 3 million cases and 100,000 deaths
attributed to pellagra
19
Figure 2
20
Rickets Returns
• Past decade vast increase in publications
• Occurs in breast fed un-supplemented LBW
babies
• High risk for newborns of dark skinned or
totally covered women in northern latitudes, or
in winter-spring
• Low vitamin D levels found in all age groups in
Israel (KH Maccabee)
21
Osteoporosis
• Aging of the population, women> men
• Vitamin D production in skin
• Sun varies by season and latitude even in
sunny countries
• Indoor occupations children and adults
• Fortification of calcium popularized
• Vitamin D lacking in raw milk
• Calcium, vitamin D, fluoride co-factors
• Fortifying milk products with Vit D needed
22
Iron Deficiency
•
•
•
•
•
Commonest MND
Affects survival, health and productivity
Affects women in age of fertility
Affects pregnancy and newborn
Affects growth and cognitive development
of infants and children
• Interaction with vitamin C deficiency
23
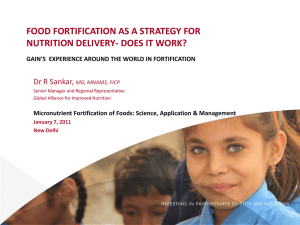
Trends in Prevalence of Anemia* in Low-income
U.S. Children, 12-17 Months Old
Program Enrollment
Percent
Follow-up
*Hgb <10.3 g/dL
Yip et al., JAMA, 1987
Birth Year
24
Preschool children
School age
children
and adolescents
Non-pregnant
women
Pregnant women
Adult men
1998
www.cdc.gov/mmwr
25
Canada 1979
•
•
•
•
National nutrition survey 1971
Geographic, social and ethnic deficiencies
Process of consultation
1979 federal regulations, mandatory
– Vitamin A and D in all milk products
– Iodine in salt
– Vitamins B and iron in flour
• Policy review 2005
• Folic acid mandatory since 1998
26
Folic Acid and NTDs
• Pre pregnancy folic acid supplements prevent neural
tube defects, 1980s
• Supplements to women in age of fertility achieves
<1/3 coverage, 1990s (US)
• FDA mandates fortification of “enriched” flour, 1998
• Canada, Chile also mandate folic acid fortification of
flour from 1998
• Preliminary reports of reduced NTD rates
• Policy renewed 1995
27
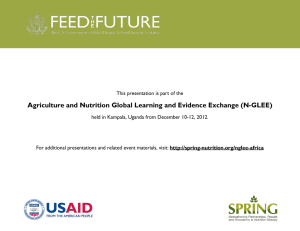
Trends in Wheat-Flour Fortification with
Folic
Return
to top.
Acid and Iron --- Worldwide, 2004 to 2007
MMWR, 2008;5:8-10
28
NTDs, Spina Bifida and Anencephaly
•
•
•
•
•
•
•
•
Serious birth defects
1 of 1,000 pregnancies
300,000 yearly worldwide
Increased consumption of folic acid
can prevent 50%-70%
Diet
Supplements
Fortification
All of the above
Mulinare J. CDC.
National Center on Birth Defects and
Developmental Disabilities, 2003
From NEJM 1999 29
NTDs In Newfoundland Pre and Post
FA Fortification
30
31
NEJM 2007
32
Fortification Status - June 2010
33
34
UK Food Standards Agency
FSA recommends mandatory fortification of bread or
flour with folic acid in order to reduce the risk of
neural tube defects in foetuses.
Currently being considered by UK health ministers,
following advice from the four Chief Medical
Officers in the UK.
If approved, the relevant UK health departments will
be responsible for producing implementation.
35
Prevalence. of low serum 25hydroxyvitamin D concentrations from
the NHANES 2000–2004
36
Yetley E A Am J Clin Nutr 2008;88:558S. American Society for Nutrition
37
Conclusion
•
•
•
•
•
•
Nutritional security - major public health issue
Affects MCH, infectious, non infectious disease
High priority – birth defects, IDA, IDD, CHD
Fortification has low sex appeal vs. clinical
Mandatory vs. voluntary – false dilemma
Requires concern, knowledge, advocacy and
leadership
• Public health role advocacy !!!
38
Reference/Sources
•
•
•
•
•
•
•
•
•
World Health Organization
UNICEF
Centers for Disease Control, Atlanta NHANES
American Academy of Pediatrics
Food and Drug Administration
GAIN
Health Canada
UK Food Standards Agency
New Public Health chapter 8
39