How does telehealth change healthcare delivery?
advertisement

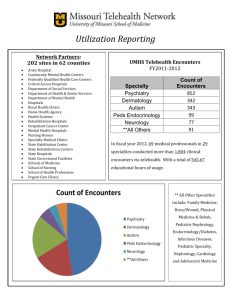
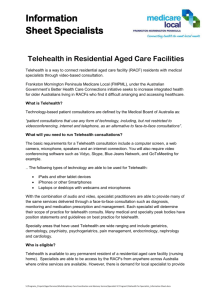
How does Telehealth change health care delivery? - a qualitative study Victoria Wade Discipline of Public Health The University of Adelaide Prof Janet Hiller, Dr Jaklin Eliott Prof Jon Karnon, Dr Adam Elshaug Telehealth is the delivery of health care at a distance, using information and communications technology electronic decision support telehealth e-health: all the uses of digital data in health care: transmission, storage, retrieval secure messaging sharable electronic health records Telehealth examples: • Real-time video: mental health assessment and treatment advice • Store-and-forward: sending photographs of burns, wounds or skin conditions to specialists for review • Tele-homecare: direct delivery of services to people at home: for example, those with cognitive impairment who live alone If telehealth is so terrific, why isn’t it everywhere? The reality of uptake is: • Slow and fragmented • Many pilot studies, feasibility tests and research trials: few ongoing services • Difficulty in integrating telehealth into routine care What is going on? Central Research Question: What are the barriers and enablers to telehealth delivering value to the routine operation of healthcare in Australia? Overall Approach: • Interviews with people who have developed and/or operated telehealth services Today’s question: • What impact does telehealth have on health services delivery? Interviewees 19 Clinicians: - 12 had multiple roles: 5 researchers, 4 telehealth coordinators (part-time), and 3 managers 11 Researchers 4 Managers 2 Telehealth coordinators (full-time) Data Analysis Directed content analysis, applying concepts from previous research to this data Work: work flow, work load and work roles Interaction: communication, cooperation and collaboration Structure: organisation and models of care Power: power relations and autonomy Impact on Work Flow • Major changes 15 • Minor changes 13 • No change 6 • Not classifiable 1 Impact on Work Flow Major Change to Work Flow: ‘The scheduling is really tricky … two rooms need to be scheduled, and the equipment … where you’ve got to have somebody locally with the patient … it’s two clinicians. So it really is quite a logistic exercise.’ No Change to Work Flow: ‘Switching [the equipment] on and having an extra clinician there made no difference at all to our usual practice of spending an hour a week talking about our patients.’ Impact on Workload • No change 15 • Increased workload 12 • Mixed impact 6 • Increased intensity of work 1 • Decreased workload 1 Impact on Workload Increased Workload: ‘Support for the initiative wasn’t really forthcoming from the unit manager at the time. So it was just seen as extra work which we didn’t have funding for.’ Decreased Workload: ‘It’s certainly more efficient than sitting in a motor car, driving to a meeting and coming back.’ Impact on Work Roles • No change 14 • New staff 12 • New roles existing staff 9 Impact on Work Roles No change to work roles: ‘I’ve tried as much as I can, to maintain it within the conventional operating systems…If I tried to introduce a change of role delineation as well, that would cause further obstacles to uptake.’ New staff: ‘We’ve appointed a chronic illness nurse…she really runs, helps to clinically coordinate those telehealth clinics now, so she sort of supervises the registrars.’ Impact on Interaction Amount of interaction • Increase 27 • No change 7 • Not classifiable 1 Impact on Interaction Increased communication ‘After the videoconference, the clinician would ring the GP and discuss the case.’ Improved cooperation ‘Occasionally, we get outraged comments…and these [video] meetings would smooth that over…it just does keep the whole relationship going.’ Impact on Organisational Structure • • • • • No change 25 New unit 4 New network 3 Minor change existing structure 2 Not classifiable 1 Impact on Model of Care • No change 15 • New model of care 13 • Minor changes 6 Types of Changes: • Increased and/or improved patient services • Upskilling and/or support for distant providers • Increased clinical governance Impact on Model of Care Patient care: ‘The health outcome for the patient was a lot better because we had immediate diagnosis of whatever the problem was.’ Health provider support: ‘He stayed there because he had people to talk to, I mean he had a circle of colleagues…which otherwise would have been totally missing.’ A New Model of Care ‘The telehealth side of things is the people in, wherever the patient is…(1) they go out to see the patient, (2) they take an image, and put in all the patient’s history and data; (3) they then send that image to a [specialist] consultant who may report on that image, yep, you’re doing great or (4) gee this person needs to have a review by the [specialist], or I’m going to send it off to our [allied health worker] who then, they may have a group of people who provide advice about this patient. (5) Might have a case conference, which will be either video case conference, or a telephone case conference with the images. And then the on-the-site carer; nurse, health worker, whoever, (6) will continue to provide the care, and then that person’s [condition] will be monitored.’ Impact on Power and Autonomy • No change 28 • Less power distant site 5 • More power nurses 1 • Not classifiable Impact on Power and Autonomy Less power for distant sites: ‘They don’t videoconference with us… they felt that they were being dictated to a little bit too much by the [city hospital specialists].’ More autonomy for nurses: ‘Previously when the doctor at [rural hospital] wanted to talk to the specialist , the doctor would go off into a little room, ring up the specialist, have a private conversation, come back and say…this is what we’ll do…Now basically the specialist has a conversation with the whole team…it does actually empower all the people in the room to speak to the specialist.’ In Summary: • Work: changes to work flow and new staff roles were common. Work load increases occurred in about one third of services • Interaction: increases were very common and positive, for patient care and for staff • Structure: more than half the services changed the model of care, far fewer changed the organisation • Power: mostly no changes. A minority of distant sites became less autonomous Conclusions: • Most telehealth services changed the organisation and delivery of health care • Telehealth can be a small, safe improvement • Or a complex, disruptive innovation Implications: • E-health and telehealth are coming • The likely impact on health services delivery should be taken into account • Health care providers, governments and the community should work together for the best results