")
Accessible infertility care - From dream to reality:
first pregnancies with a simplified IVF procedure
Willem Ombelet
Genk, Belgium
1st congress
Male infertility
750 participants
34 countries
Robert Edwards
2010 Nobel Prize winner
Howard Jones, US IVF pioneer
34 years
IVF
> 5.4 million IVF / ICSI babies worldwide
SUCCESS ???
www.nightearth.com
But what about …
www.nightearth.com
www.ivf-worldwide.com/ivf-directory/
5
1st priority
=
Prevention
Education
Family-planning
Developing
Countries
=
overpopulation
Limited budget
Limited Resources
Argument
More important priorities:
HIV, tbc, malaria,
vaccinations …
ART =
ethical issue
ART = expensive
Limited or no interest for infertility
in developing countries
Infection-related tubal block
Asia
Tubal factor : why ?
39 %
Latin America
44 %
Sexually transmitted diseases
Post-partum infections
Illegal abortions
Urbanisation - mobility
Polygamy
Resistant micro-organisms …
Africa
65 - 85 %
World community statements
1.“Men and woman of full age, without any limitation due to race, nationality or religion,
have the right to marry and to raise a family”. This statement was adopted 60 years
ago at the 1948 UN Universal Declaration of Human Rights and can’t be misunderstood:
it implies the right to access to fertility treatments when couples are unable to have children.
2. At the United Nations International Conference on Population and Development in Cairo
in 1994 the following statement was made “Reproductive health therefore implies that people
have the capability to reproduce and the freedom to decide if, when and how often to do so …
and to have the information and the means to do so …”
3. UN Millennium Declaration, signed in September 2000 : “Achieve, by 2015, universal access
to reproductive health”.
4. In 2001, on the occasion of a WHO meeting on "Medical, Ethical and Social Aspects of
Assisted Reproduction" in Geneva, a call for the integration of infertility into existing sexual
and reproductive health care programmes in developing countries was made.
5. In 2004 the World Health Assembly proposed five core statements, including “the provision
of high-quality services for family-planning, including infertility services”.
Why should we care ?
• Infertility not very prevalent in
developing countries
•
Infertility is not a serious problem for people in developing
countries
•
“Individual problem, not a public health problem, not a
problem of the nation…”
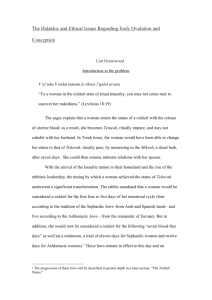
Prevalence of infertility
Prevalence of infertility
The estimate of the magnitude of the involuntary infertile
Demographic definition - 5 years of childlessness (2004)
(in developing countries minus China, data up to year 2000)
Total: 186 million women
168
millions
180
160
140
120
100
(Source: Rutstein and Shah,
DHS Comparative Reports, no. 9,
2004)
80
60
40
18
20
0
Primary infertile
Secundary infertile
Why should we care ?
•
Infertility not very prevalent in developing countries
• Infertility is not a serious problem for
people in developing countries
• “Individual problem, not a public health problem, not a
problem of the nation…”
Challenge: address infertility as an impairment of body
function which is affected by societal features
Level 6
Lost dignity in death
Level 5
Violence-induced suicide
Starvation / disease
Developing/ transitional societies
Severe economic deprivation
Level 4 Moderate / severe violence
Total loss social status
Level 3
Mild marital / social violence
Social isolation
Marital status
Level 2 Depression, helplessness
Level 1
Developed societies
Fear, guilt, self-blame
WHO Current Practices and Controversies in Assisted Reproduction "Infertility and social suffering,"
Daar & Merali, 2001, page 18, Figure 2.
Poverty, low education, gender inequality, high value of
children, limited health care
Transactional sex
•
•
•
•
STIs/HIV
Bad sexual
health,
obstetric and
neonatal care
Concurrent partners
•
Multiple unions
•
No condom use
Early age at first sex
Gender based violence
unintended
pregnancies
(unsafe
abortions)
INFERTILITY
AND
CHILDLESSNESS
Why should we care ?
•
Infertility not very prevalent in developing countries
• Infertility is not a serious problem for people in developing
countries
• “Individual problem, not a public health problem,
not a problem of the nation…”
Mother or nothing – the agony of infertility
Prof dr M Fathalla, WHO Bulletin, December 2010
“In a world that needs vigorous control of population
growth, concerns about infertility may seem odd, but
the adoption of a small family norm makes the issue
of involuntary infertility more pressing. If couples are
urged to postpone or widely space pregnancies, it is
imperative that they should be helped to achieve
pregnancy when they so decide, in the more limited
time they will have available.”
Social and psychological suffering
How to prevent suffering?
→ accept pronatalism and try to help people to have children
→ fight pronatalism : reduce the negative socio-cultural and
economic consequences of infertility
Best solution → combination of both strategies on the basis of
cost-effectiveness
Pennings, 2010
International organisations: no interest
International Planned Parenthood Federation
◦ Only family planning research and HIV prevention
The Population Council
◦ Leading role in development new contraceptives
Family Planning International
◦ Focus on family planning research and HIV prevention
World Health Organization
◦ Focus on family planning & prevention STD’s // HIV
Arusha (expert) meeting
One-day clinic
(diagnosis)
December 15-17, 2007
Make it
Ovarian stimulation
for IVF
IVF
Laboratory
SIMPLE
EFFICIENT
SAFE
AFFORDABLE
Convincing the scientific
community
Health Care Centres
Family planning
Mother care
Infertility care
Holistic model of reproductive healthcare
horizontal and infertility included
FP
HIV
ANC
Infertility
care
Arusha meeting 2007
One day clinic
(diagnosis)
Make it
IVF ovarian
stimulation
IVF
laboratory
SIMPLE
EFFICIENT
SAFE
AFFORDABLE
HIGH COST IVF Lab
Expected price
→1.5 - 3 Million €
t WE
lab - a simplified IVF procedure
Simplified Culturing System
Two glass tubes connected by needles and tubing
tube 1 = CO2 generator
Citric acid + sodium bicarbonate -> CO2
tube 2 = medium equilibration / IVF
Fertilisation and culturing in separate glass tubes
CO2 incubator not needed
Prof. Dr. Jonathan van Blerkom
University of Colorado, Denver
Prof. Dr. Willem Ombelet and
Prof. Dr. Carin Huyser
Step 1: Set-up and equilibration
6.3 - 7.1 % CO2
12 - 13% O2
Citric acid + sodium bicarbonate + water
produces carbondioxide to equilibrate
culture medium to pH 7.25- 7.35
Step 1: Set-up and equilibration
Step 2: Insemination
QuickTi
me™
een
QuickTi
me™
enen
een
-decompressor
-decompressor
n vereist
deze
afbeeldi
weer
geven.
zijzij
n vereist
omom
deze
afbeeldi
ngngweer
te te
geven.
Day 0
Insertion of oocytes and sperm cells: 1 oocyte per
tube with 1000-5000 good motile sperm cells
Step 3: Fertilisation check
Fertilisation check through
the glass tube wall
Day 1
Step 4: Embryo visualisation
Day 2
Day 2
Day 3
Day 3
Embryo transfer
Couple selected for first IVF trial
♀ < 36 years
♂ IMC> 1 million
IMC < 1 mill
ICSI
Ovarium Stimulation
(Rec FSH-antagonist)
Oocyte retrieval (OR)
≥ 8 oocytes
Regular Culturing (RC)
< 8 oocytes
Excluded
Simplified Culturing (SC)
If 1 top embryo
SET day 3
Regular culturing
Randomisation
1st TRIAL
If no top embryo
Cryo surplus embryos
SET: RC embryo
+
SET
+
If ≥ 2 top embryos
SET: SC embryo
Serum HCG 9 – 11 days after OR
If no fertilisation
If no good quality embryo
No transfer
Excluded
Negative
Positive
Ultrasound 5-6 weeks after OR
Interim report
Age < 36yrs, min 8 oocytes, SET
n= 28
ET
17/28 t WE lab (60,7%)
4 excluded
11/28 RCS (39,3%)
FR t WE lab : 60.8%
HCG+
7/17 t WE lab (41,2%)
2/11 RCS (18,2%)
1 BC
IR
6/17 t WE lab (35,3%)
2/11 RCS (18,2%)
first pregnancy from Frozen ET
FR SCS: 58.2%
Simplified culturing system
Until 31-12-12
12 ongoing pregnancies
First delivery 07-11-12 – healthy boy – 3500 gr
Day 3
t WE
lab - a simplified IVF procedure
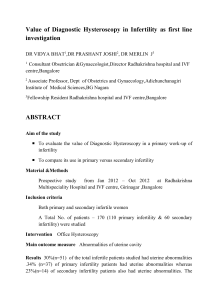
Direct costs IVF Laboratory
10 – 15 %
Cost per IVF cycle
(medication excluded)
2500 € → < 200 €
Doctor Fees
29%
Clinic Fees
8%
IVF
Laboratory
Fees
35%
Laboratory
Fees
48%
Medication
28%
Cost analysis per procedure
in a private practice in South Africa
C Huyser 2012
Doctor Fees
23%
Clinic Fees
6%
ICSI
Medication
23%
Price
Medication
Belgium per
cycle
Price
Medication
25 - 120
Euro
Modified IVF protocol
1075 Euro !!
Clomiphene 100 mg
hCG 5000 U
MENSES
35 h
3 4
D1
5
6 7 8 9
X
Day 0
>= 17 mm
Pick-up
US OVARIES
Day 3
US OVARIES
Menopur 75 or Puregon 75
Low dose hCG
ET
Current / future developments
• Studies with low stimulation protocols (CC-low dose hCG) in t WE lab setting
• Studies on sperm number needed for IVF in t WE lab setting
• Cost – analysis …
tWE
training centre
tWE
2013
Solar energy
IVF centre
Compton Foundation
What about funding ??
http://nnadofoundation.webs.com/
www.thewalkingegg.com
Mumbai
Lima
Nairobi
Pretoria
Numbered
Signed
Registrated
Partners
WHO
ESHRE
IFFS
ESGE
ISMAAR
The Walking Egg
Project
Gynetics
Storz
Esaote
…
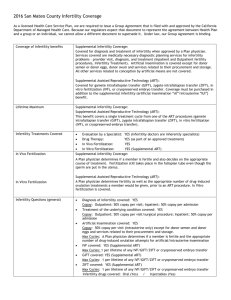
Packages
Level 2 (up to IVF)
Study Genk
Level 3 (cryo/ICSI)
TWE
Manual diagn. Phase
ManualTraining
Business-Plan
Registration system
Partners-Industry
Level 1 (up to IUI)
Support Socio-cultural
Study Group ESHRE
Select pilot-centres
India, Kenia, Peru …
Building
Personel
Fixed costs
Running costs
Search for funding
When a thing was new, people said,
“It is not true“
Later when the truth became obvious, people said,
“Anyway, it is not important“
And when its importance could not be denied, people said,
“Anyway, it is not new“
William James, 1842 - 1910
")