Clinical Leads Meeting
advertisement

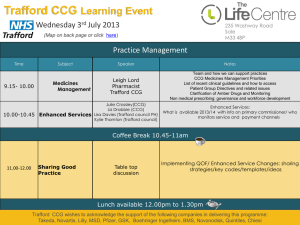
QOF Quality & Productivity Indicators Dr Steve Jenkins & Chris Valchero 11th July 2012 QOF Q&P indicators • Congratulations!- Most practices achieved maximum QP 6-11 points available in Yr 1 • Year 2 – Building on successes from year 1 and some amendments based on our learning – Trafford CCG continue to facilitate process – Overseen by NHS Greater Manchester Cluster • Some National revisions to Q&P indicators – Removal of Prescribing Indicators QP1 – 5 – Same Outpatient and Unscheduled Admission Indicators QP 6 – 11 but new areas – Addition of A&E Indicators QP 12 – 14 QP 6 – 8 GP outpatient referrals • Dyspepsia • Trafford rate of gastroscopies relatively high compared to other PCTs (Atlas of Variation) • Continue with Dyspepsia • Aiming to localise pathway following feedback / discussions from External Peer Review • Childhood Eczema • Dermatology - one of highest outpatient specialties • Availability of Community Children’s Nursing Teams to support patients with known diagnoses of eczema • Developed localised pathway from Trafford Dermatology Guidance • Rhinitis • ENT – another of highest outpatient specialities • Consultant advised an area of common inappropriate referral • Localised pathway developed by multidisciplinary team QP 6 What do we need to do? • • • • • • • • Practice Internal Review of outpatient referrals If no referrals – consider in-house management Speciality data available within Actuate by mid July Clinical system search (referral / in-house ) or get secretary to keep record for specific diagnoses Compare variance against Map of Medicines Pathways for each area Document outcome of Internal Review meeting on QP6 template QP 6 template now more specific and one template for all 3 areas Submit to CCG by 28 Sept 2012 QP 7 What do we need to do? • QP 6 template must be submitted before External Peer Review Meeting • TCCG to facilitate a specific QOF Q&P External Peer Review Meeting – Oct 12 (date tba) • Practice GP representative to attend • Practice feedback will inform further localisation of pathways • Outcomes / completed QP 7 template submitted to TCCG shortly after meeting QOF Quality and Outcomes Framework 2012-13 Template QP 6 Notes of internal Meeting to Review the Data on Outpatient Referrals Note: Internal review must be carried out prior to external review. Practice Name Date of meeting Present: ( Full range of clinicians to be represented including Nurse representation) Confirmation of Review of Actuate Data at speciality level and/or practice clinical data. (Minimum of 3 patients per speciality) ie Gastrology,ENT and Dermatology Summary of Referrals received indictating degree of compliance. Fully, Mostly,Partially or Non-compliant) ( Minimum 3 patients per speciality) Dyspepsia Rhinitis Ezcema Dyspepsia Rhinitis Ezcema Referral anomalies identified. Give details of where each speciality is non compliant with the pathway, where the referrals are appropriate and non compliant. Details of changes needed to improve compliance. This completed template must be forwarded electronically to Sarah Gunshon. TCC Business Manager no later than 28th September 2012.Templates received after this date will not achieve QOF Points. QOF Quality and Outcomes Framework 2011/12 Template QP7 Notes of External Peer Review Meeting to Compare Data on Secondary Care Outpatient Referrals Practice Name Date of meeting Present: (Name of GP representing the practice) Details of other practices present. Reflections on referral behaviour and variances amongst practices. Dyspepsia: Rhinitis; Ezcema: What have clinicians learnt to alter their referral patterns. Dyspepsia: Rhinitis: Ezcema: How has this discussion changed their referral behaviour. Dyspepsia: Rhinitis: Ideas from discussion to reduce unnecessary hospital attendances e.g Following a new pathway. Recommendations to CCG for service design improvements for areas of commissioning improvement that would enable more effective management of patients in the community. Ezcema: Dyspepsia: Rhinitis; Ezcema: Dyspepsia: Rhinitis: Ezcema: This completed template must be forwarded electronically to Sarah Gunshon. TCC Business Manager. sarah.gunshon@trafford.nhs.uk. The date will be advised at the External Review. Templates received after the specified date will not achieve QOF Points. QP 9 – 11 Unscheduled Admissions • COPD • Local best practice Trafford guidelines based on NICE guidance • Continue high emergency admissions for respiratory conditions • Build on work undertaken last year • Asthma • Trafford PCT ranks high for asthma admissions • 14th highest diagnosis for which patients admitted in Trafford • Evidence structured primary care improves symptom control • TIA • Evidence timely management of TIA reduces stroke risk (NICE 2008) • Greater Manchester Cardiac and Stroke Network assessment pathway with referral to TIA clinics • Assessment via ABCD2 tool – training DVD & in info pack • Key priorities for implementation (NICE 2008) • Rapid recognition of symptoms and diagnosis • People who have had a suspected TIA who are at high risk of stroke (that is, with an ABCD2 score of 4 or above) should have: – aspirin (300 mg daily) started immediately – specialist assessment and investigation within 24 hours of onset of symptoms QP 9 What do we need to do? • • • • • • • • • • Practice Internal Review of unscheduled admissions If no unscheduled admissions, consider in-house mgt Data available within Actuate by mid July (incl diagnoses) Keep copies of discharge letters / clinical system search Proforma for practices to undertake and document review for each area Document outcome of Internal Review meeting on QP9 template QP 9 template now more specific & one template for all areas Attach 3 “patient anonymised” proforma to QP 9 template Submit to CCG by 28 Sept 2012 External Peer Review (QP 10) as per outpatients process QP 12- 14 Accident & Emergency QP 12 What do we need to do? • Practice Internal Review of top 10 A&E attendances • Over 65s • Under 15s • Frequent Flyers • Quarter 4 patient level data available within Actuate by mid July (as report) • Document on proforma - consider day / time / reason for attendance / management in house • ? Discharge info for UHSM attendances • QP12 – one template for all 3 areas with attached proforma • Submit to CCG by 28 Sept 2012 for use at External Peer Review Meeting QP 13-14 What do we need to do? • QP 13 • Agree Improvement Plan • Proposals for improved access • Arrangements in practice • Service re-design via CCG • Submit QP 13 template to CCG shortly after External Peer review Meeting • QP 14 • Implement Practice Improvement Plan • Aim to reduce avoidable A&E emergency attendances • Quarterly A&E reports will be updated on Actuate (Qtr 1 & 2 data available) • Produce report of action take on QP 14 • Submit QP 14 template to CCG by end Feb 2013 Contacts • TCCG Actuate & QOF Q&P Lead – Sarah.gunshon@trafford.nhs.uk – 0161 873 9515 • TCCG Map of Medicine – Matthew.preece@trafford.nhs.uk – 0161 873 9511 • QOF Lead – Gail.sampson@trafford.nhs.uk What Next? • Pathways are being finalised • Complete packs available 3rd week in July • Data available on Actuate 3rd week in July • Practice secretary keep log of referrals • Keep log of unscheduled admission discharges • Re-familiarise with Actuate…. • ANY QUESTIONS? Process • Target is to review management plans for minimum of 3 high risk COPD patients per 2000 registered list • Review last year’s emergency admissions (in pack) • If needed, review those with more than 3 exacerbations requiring antibiotics • Ensure optimum management • Review use of management plans, rescue therapies (advice, deferred script for steroids and abx) & referral to pulmonary rehab (if appropriate) • Documents in pack – more available from TCC • Review data and complete audit proforma, discuss at internal review in practice and return by mid Nov to TCC