The Case for Medical Homes and Community
Networks
“NC’s Approach to Healthcare”
Webinar – National Partnership for Women &
Families
Denise Levis Hewson, RN, BSN, MSPH
July 13th, 2010
Community Care of North Carolina
Joins other community providers (hospitals, health
departments and departments of social services) with
primary care physicians
Designated primary care medical home
Creates community networks that assume responsibility
for managing recipient care in concert with the PCP
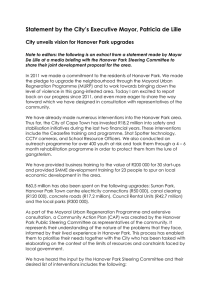
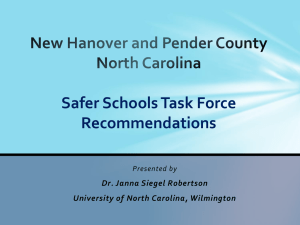
Community Care of North Carolina
AccessCare Network Sites
AccessCare Network Counties
Access II Care of Western NC
Access III of Lower Cape Fear
Community Health Partners
Northern Piedmont Community Care
Carolina Collaborative Comm. Care
Carolina Community Health Partnership
Partnership for Health Management
Central Piedmont Access II
Comm. Care Partners of Gtr. Mecklenburg
Southern Piedmont Community Care Plan
Community Care of Wake and Johnston Counties
Community Care Plan of Eastern NC
Central Care Health Network
Sandhills Community Care Network
Community Care Networks
Are Non-profit organizations
Seek to incorporate all providers, including safety net providers
Have Medical Management Committee oversight
Receive $3.00 pm/pm from the State for most enrollees
$8.00 pm/pm for the Aged, Blind and Disabled enrollees
Hire care management staff to work with enrollees and PCPs
Participating PCPs receive $2.50 pm/pm to provide a medical home
and participate in Disease Management and Quality Improvement
$5.00 pm/pm for Aged, Blind and Disabled
NC Medicaid also pays the PCP “Fee For Service” @ 95% of Medicare
Each CCNC Network Has:
A Clinical Director
A part-time physician who is well known in the community
Meets with physicians to encourage CCNC participation
Provides oversight for quality improvement in practices
Serves on the Sate Clinical Directors Committee
A Network Director who manages daily operations
Care Managers to coordinate services for enrollees
A PharmD to assist with Med Mgt. of high cost patients
Psychiatrist to assist in mental health integration (summer 2010)
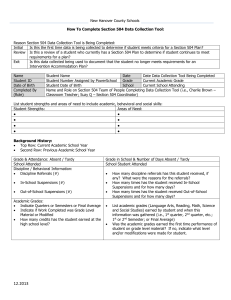
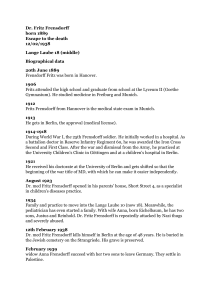
Access III of the Lower Cape Fear, Inc.
Organizational Chart
Lydia Newman, MPP
Executive Director
Jim Jones, MD
Medical Director
Don Collins, CAE
Chief Operating
Officer
Susan Martin
HR & Technology
Manager
Angela Ives, RN
Case Management
Coordinator
Program Director for
Diabetes & GMV
Randy Barrington,
MBA
Quality Improvement
Coordinator
Megan Rose,
PharmD
Pharmacy
Coordinator
Program Assistants
Megan Marshall
Melanie Melton
Annamarie Atwood
Office Coordinator
Joelle Eddy
Administrative
Assistant
Ada Atkinson, RN, BS
Chronic Care
Coordinator
Aimee Donaton,
MPH, RD, LDN, CDE
Case Managers
Regina Pool, RN
Ruth Huggins, RN, BSN
Fran Harris, RN, CCM
Barbara Stern, RN, CDE
Tina McPherson, RN
Val Southern, RN, CCM
Connie McMurray, RN, BS
Mary Stephens, SW
Kathy Reese, RN
Marry Jarosz
Bladen & Columbus
Bladen County
Brunswick County
Brunswick County
Columbus County
Columbus County
New Hanover County
New Hanover County
Onslow County
Health Check Coordinator
New Hanover County
Case Managers
Beverly Newton, RN, CCM
Linda Dougherty, RN
Elissa Hanson, MSW, LCSW
Bobbi Kuhn, RN,
Heather Lippincott, MSW,LCAS
Roxanne Noble, RN, CCRC
Pender County
New Hanover County
New Hanover County
New Hanover County
New Hanover County
New Hanover County
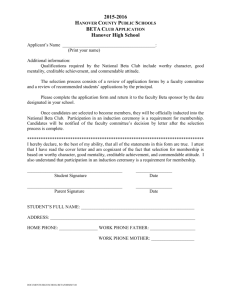
Community Care’s Chronic Care Program
Managing Clinical Care
(Spreading Best Practice)
Clinical Directors Group
I
• Select targeted diseases/care processes
• Review evidenced-based practice guidelines
• Define the program
• Establish program measures
Local Medical Management Committee
II
III
• Implement state-level initiatives
• Develop local improvement initiatives
PRACTICE A
PRACTICE B
PRACTICE C
Care Managers and CCNC quality improvement staff support clinical management activities
Current State-wide
Disease & Care Management Initiatives
Asthma
Diabetes
Pharmacy Management (PAL, Nursing Home Polypharmacy)
Dental Screening and Fluoride Varnish
Emergency Department Utilization Management
Case Management of High Cost-High Risk
Congestive Heart Failure
Chronic Care Program – including Aged, Blind and Disabled
Rapid Cycle Quality Improvement
Chronic Care Program Components
Enrollment/Outreach
Screening/Assessment/Care Plan
Risk Stratification/ Identify Target Population
Patient Centered Medical Home
Transitional Support
Pharmacy Home – Medication Reconciliation, Polypharmacy & PolyPrescribing
Care Management
Mental Health Integration
Informatics Center
Self Management of Chronic Disease
Program Components & Interventions
Patient Centered Medical Home
- Every enrollee has a patient centered medical home
- Evidence based care is provided
- Ensuring disease management of chronic illness(e) occur
(diabetes, CHF, COPD, HTN, depression, etc.)
- Participating actively in clinical performance improvement activities
- Patient tracking and referrals
- E-prescribing
- Electronic health information
Program Components & Interventions
Transitional Support
• Across providers and delivery settings
• Partner with hospitals
• Obtain real time data
• Participate in discharge planning
• Coordinate community resources and services
• Face-to-face care management contact with high risk patients within 3
business days from discharge
• Medication reconciliation
• Follow-up visit with PCP and/or specialists
Program Components & Interventions
Pharmacy Home
• Pharmacists integrated into networks to target high risk population
• Focus on adherence, clinical alerts, therapeutic equivalents, and
medication reconciliation at transitions of care
• Feedback to care manager and PCP
• Poly-pharmacy related – poor self- management of daily regimen
and competing or interacting daily
• Poly-prescriber related – prescriber often operating in an
information vacuum
Program Components & Interventions
Care Management
- Incorporating a standardized approach to care coordination and
management priorities
- Integrating targeted case management of high risk patients
- Ensuring disease management
- Generalist vs. Specialist Approach
- Targeting interventions where they will have the greatest impact
- Support patient self management
Program Components & Interventions
Mental Health Integration
•
•
•
•
•
•
•
Develop relationships and communication processes/tools
Screening for and management of Depression
Management of Depression
Partner with Behavior Health
Collaborate on Quadrant IV patient
Co-location opportunities
Psychiatrists at central office and at networks (summer 2010)
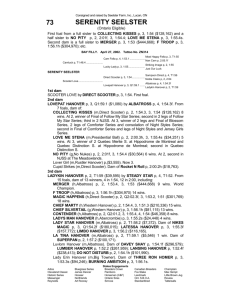
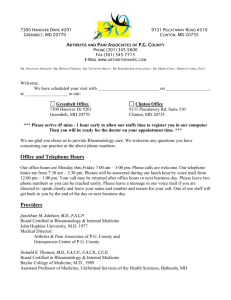
646 Demonstration Project
646 Counties
Ashe Alleghany
Surry
Rockingham
Stokes
Caswell
Warren
Granville
Vance
Person
Northampton
Gates
Hertford
Halifax
Watauga Wilkes Yadkin
Bertie
Orange
Mitchell
Franklin
Forsyth Guilford Alamance
Avery
Caldwell
Durham
Nash Edgecombe
Alexander
Washington
Dare
Davie
Madison Yancey
Martin
Tyrrell
Davidson
Iredell
Wake
Randolph
Burke
Wilson
Buncombe McDowell
Catawba
Chatham
Pitt
Beaufort
Rowan
Hyde
Haywood
Johnston
Greene
Swain
Rutherford
Lincoln
Lee
Cabarrus
Graham
Montgomery
Jackson
Henderson
Gaston
Harnett
Lenoir
Polk
Cleveland
Stanly
Wayne
Craven
Moore
Pamlico
Mecklenburg
Cherokee
Macon
Transylvania
Cumberland
Clay
Jones
Richmond Hoke
Sampson
Union
Anson
Duplin
Onslow
Scotland
Carteret
Robeson
Exempt
Intervention
Bladen
Pender
Columbus
Holdouts
Brunswick
Updated: October 1, 2009
New
Hanover
KEY ELEMENTS OF NCCCN’s DEMONSTRATION
During years one and two, NCCCN will manage
approximately 30,000 dually-eligible beneficiaries who
receive care from 198 practices in 26 counties.
At the beginning of year three, an estimated 150,000
Medicare-only beneficiaries who will receive care from those
practices will be added to the demonstration.
During years three to five, NCCCN will manage an estimated
180,000 Medicare and dually-eligible beneficiaries.
Payment to Support 646
Use the “one touch” rule – if a dual is touched by a
participating practice, then CMS counts that person a
“enrolled”
Practices and networks will get the PMPM from the state
for the enrolled duals
Enrollment is voluntary, so practices and networks will still
be managing those that have touched a practice but are
not enrolled
Straight Medicare not included until year 3 and goal for
shared savings to fund the PMPM
Shared Savings
Finalizing methodology with CMS
Will have a threshold savings, then 80/20
Details still being finalized
Must achieve a percentage of improvement in
quality metrics to receive financial savings
Data/Informatics
Use of claims-derived data for population management and care
coordination
Quality measurement with claims data and chart review data
(Examples to follow)
Chronic Care/ 646 Patient Database
80 data elements reported quarterly on ALL ABD recipients:
Demographics
Spending by category
Utilization
Diagnoses
Use of ancillary services
Priority scoring
Provider Portal Patient Record: Care Team Summary Page
Want to know more:
www.communitycarenc.org
Questions:
 0
0