Click Here To - Cancer Center Business Summit
advertisement

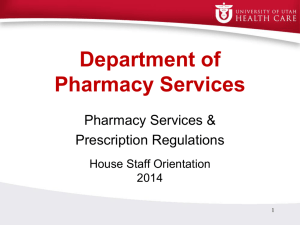
Future of Drug Delivery and Formulary Melissa Grimes Ayles, Director of Partner Relations & Business Development, Patient Services, Inc. Mike Ellis, Corporate VP, Specialty Pharmacy & Infusion, Walgreens Surya Singh M.D., Corporate Vice-President, Head of Medical Benefit Management, CVS Caremark Burt Zweigenhaft, Vice Chairman, Onco360 Oncology Pharmacy Future of Drug Delivery and Formulary Melissa Ayles, MBA Director, Partner Relations and Business Development Patient Services, Inc. Cancer Patient Challenges • Affordability and Accessibility of Medication – Specialty Tier Medications – 24% annual income for drug alone – ACA = AACA “Almost Affordable Care Act” • Advanced Diagnostics – Individualized medicine • Value-Based Therapy – Ancillary medications and treatments PSI the Missing Link • Copay Assistance – Affordability of medicinal copay needs – Deductible, out of pocket costs – Formulary of therapy treatment meds • Premium Assistance – Provision of reimbursement vehicle • Ancillary Services – Incidental Expenses (wheelchair, oxygen, transportation) • Network of Specialty Pharmacies – Focused on Value-Based Cancer Care Office of Inspector General SPECIAL ADVISORY BULLETIN, MAY 21, 2014 HTTPS://OIG.HHS.GOV/FRAUD/DOCS/ALERTSANDBULLETINS/2014/INDEPENDENT-CHARITY-BULLETIN.PDF Compliance is a High Priority (New Office of Inspector General Special Advisory Bulletin, May 21, 2014) 1. Disease Funds will… a. Be legitimately defined in accordance with “widely recognized clinical standards” (e.g. FDA, CMS???) b. Be defined “in a manner that covers within each fund a broad spectrum of products wherever possible including generics”. c. “Not be defined by reference of specific symptoms, severity of symptoms, method of administration, stages of particular disease, type of drug treatment, or any other way of narrowing” d. Not be defined as “high cost or specialty drug funds” and must consider other financial variables beyond income (e.g. costs of living, debt) Compliance is a High Priority (New Office of Inspector General Special Advisory Bulletin, May 21, 2014) 2. No single-drug funds… a. Providing copayment for only one drug or only one manufacturer. b. Unless fund is legitimately defined, includes combining two or more related disease funds, covers any drugs needed by patient, covers all copayments for items and services needed by patients and is submitted for consideration to OIG on a case by case basis. Compliance is a High Priority (New Office of Inspector General Special Advisory Bulletin, May 21, 2014) 3. Diluting Funds May Be Acceptable… a. According to legal counsel discussions with OIG, OIG may consider single drug funds if they are “diluted”. (1). Dilution means: Premium , Copayment, Travel Expenses, and Ancillary Expenses (Nursing, labs, diagnostic test, physician copays, infusion costs, etc.) 4. Reporting must be OIG compliant and not correlate donation amount with patient usage Consequences to Patients and Manufacturers Patients • No access to rare and orphan drugs • Barrier to assistance: adverse health; life/death • Most vulnerable populations (Medicare beneficiaries); establishes a class medical society Manufacturers • Add more drugs to the “fund” including generics –supporting other drugs • Add premium assistance if a “copayment” program • Provide “copayment” assistance for only private patients • If single donor program; dilute with copay, premium, travel expense, ancillary services PSI Solutions • Created and defends model – Passion and motivation to help patients afford and gain access to care they need, not just copay assistance • Broaden Disease State Funds – Formulary expansion to include generics, and value based therapies – Funds include • Premium Assistance • Copay Assistance (Deductibles as well as copays) • Ancillary Services Assistance Melissa Ayles Director, Partner Relations and Business Development Patient Services, Inc. 972.890.2162 mayles@uneedpsi.org http://www.patientservicesinc.org/ http://www.cancersupportcommunity.org/General-DocumentsCategory/Elevating-the-Patient-Voice.pdf Future of Drug Delivery and Formulary Mike Ellis, Corporate VP, Specialty Pharmacy & Infusion, Walgreens Future of Drug Delivery and Formulary Surya Singh M.D., Corporate Vice-President, Head of Medical Benefit Management, CVS Caremark Generics and Biosimilars in Oncology • Increasing availability of generics in oncology creating opportunities for inclusion in specialty tier(s) and potential exclusions • Biosimilars – several questions remain, but they are coming and development activity is increasing – Sandoz has largest current global biosimilar sales (mainly in EU) at $500M with an estimated annual growth rate of 20% and active pipeline – Amgen developing portfolio of six biosimilars – Several other manufacturers (Teva, Hospira) active in biosimilars globally but have not publicly declared plans in US 1 2 1. “No biotech copycat drug lift off before 2017 - Novartis CEO.” Reuters, August 25, 2014. Accessed September 3, 2014 at http://www.reuters.com/article/2014/08/25/novartis-biosimilars-idUSL5N0QV25X20140825 2. “Amgen makes room for biosimilars despite cutting manufacturing 23%.” BioPharmareporter.com July 30, 2014. Accessed September 3, 2014 at http://www.biopharma-reporter.com/Markets-Regulations/Amgen-makes-room-for-biosimilars-despite-cuttingmanufacturing Trastuzumab claims: Substantial Variation in Allowed Amounts Source : 2013 CVSC Book of Business This slide contains references to brand-name prescription drugs that are trademarks or registered trademarks of pharmaceutical manufacturers not affiliated with CVS Caremark. Role of Home & Ambulatory Care in Oncology • Current role in administration of selected supportive care agents • Potential role in administration of longer term therapies (not cytoxic chemotherapy) • Partnerships with provider organizations & cancer centers Future of Drug Delivery and Formulary Burt Zweigenhaft, Vice Chairman, Onco360 Oncology Pharmacy