AUDIT ON THE USE OF ORAL
BACLOFEN IN CHILDREN WITH
CEREBRAL PALSY ATTENDING
WARRINGTON CDC
Dr B George
AIM
To identify various factors affecting usage.
To identify existing regimes of prescription.
To document benefits and side effects.
To identify existing or prevalent guidelines on
oral prescription.
METHODS
List of all children registered as ICD-10 (G80-83)
codes as having cerebral palsy under the
Warrington CDC. Obtained from IT (medical
records) at Warrington CSU.
Notes retrieved and children currently or
previously on Baclofen identified.
Data collated on above sub-set.
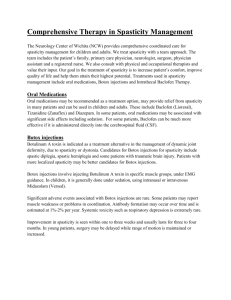
Total children registered with CP
Total notes obtained
Children with CP on analysis
Children currently on Baclofen
Children previously on Baclofen
78
43
42
09
02
‘n’ total no
11
% of children with CP on
Baclofen is 11/42 =
26.2%
Avg age of our sub group
Avg age at diagnoses
Males
Females
10y 1m
30 m
8
3
BODY PATTERN INVOLVEMENT
Diplegia
Quad/tetraplegia
Hemiparesis/plegia
Undiagnosed syndrome
CP -unspecified
3
3
1
2
2
ETIOLOGY
Asphyxia
Syndrome (Undiagnosed)
Unspecified
8
2
1
MOVT PROBLEMS
Spasticity
10
Dystonia
1
CO-MORBIDITIES
THERAPIES
Physiotherapy
Occupational therapy
Speech & language
OTHER MEDICATIONS
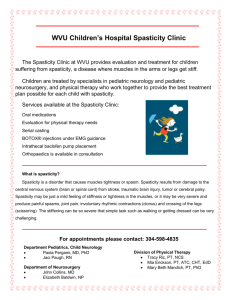
BACLOFEN – DATA
Freq
ODS
BDS
TDS
QDS
1
3
6
1
BNF
BNF advises 0.75 mg – 2 mg/kg daily or 2.5 mg
q.d.s increased gradually to maintainence.
Child 1–2 years 10–20 mg daily in divided doses,
Child 2–6 years 20–30 mg daily in divided doses,
Child 6–10 years 30–60 mg daily in divided doses
Child 10–18 years 5 mg 3 times daily increased
gradually; max. 2.5 mg/kg or 100 mg daily
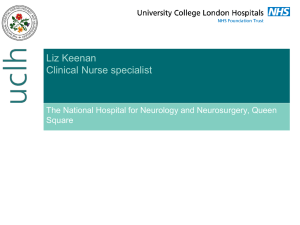
MOVT
Baclofen
Mg/kg/d
months
when
started
By grade
spasticity
yes
20 od
?
55
SG
2.5 od
1
6y9m
spasticity
yes
5,5,5
0.88
19
C
1 mg tds
4
8 y 10 m
spasticity
yes
10,10,15
1.4
?
?
10 y 7 m
spasticity
yes
5,5,5
0.86
18
C
2.5 mg bd
3
10 y 2 m
spasticity
yes
10,10,10
1
19
C
2.5 mg bd
2
12 y 2 m
spasticity
trialled
nil
nil
79
C
2.5 mg tds
upto 5 bd
4
6y
dystonia
yes
4,4,4,4
0.8
18
C
2.5 mg tds
5
9y7m
spasticity
trialled
nil
nil
45
C
2.5 mg tds
upto 5 bds
5
6 y 10 m
spasticity
yes
5,5,5
1.5
14
?
3 mg tds
5
14 y 10 m
spasticity
yes
5,5
0.25
107
C
2.5 bd
upto 5 tds
4
5y9m
spasticity
yes
20,15,15
1.85
58
C
2.5 bd
upto 5 tds
3
AGE
DOSE
PT
TB
JC
13 y 5 m
Dose At
Starting
mg
GMFCS
NOW
4
RF
GC
SDC
KK
DM
MW
EW
VR
LT
BNF
BNF advises 0.75 mg – 2 mg/kg daily or 2.5 mg
q.d.s increased gradually to maintainence.
Child 1–2 years 10–20 mg daily in divided doses,
Child 2–6 years 20–30 mg daily in divided doses,
Child 6–10 years 30–60 mg daily in divided doses
Child 10–18 years 5 mg 3 times daily increased
gradually; max. 2.5 mg/kg or 100 mg daily
SIDE EFFECTS
Nil 7
KK- stopped as no response(no s.e.)
MW - stopped as worsening reflux
DM – vomiting,
JC -- decreased appetite
VR-Increasing spasticity, stopped walking
unaided, swallowing diff---dose reduced
CONCLUSIONS
All patients prescribed for increasing hypertonia.
No standardised regime of prescription
identified-i.e. starting regime, increasing dosage,
frequency.
All mg/kg dosages were within BNF limits.
Some side-effects noted, mainly increasing
feeding problems and reflux. ?statistical
significance due to small numbers.
No guidelines identified in literature search
specifically for oral Baclofen prescription.
RECOMMENDATIONS
To propose a regional standardised regime for
prescription.
To generate information/advice sheet on Baclofen
for prescribers in the hospitals and community.
To generate clinic sheet for prescribers to
document information on Baclofen on the first
and then on each clinic visit.
THANK YOU
 0
0