Drug misuse, its complications
and management
Dr Susi Harris
Clinical Lead, City and South
Community Drug and Alcohol team
Summary of talk
• Drug misuse
–
–
–
–
Diagnosing substance dependence
Types of substance and prevalence
Individual drugs and their harms
Administration routes
• Brief history of Drug Misuse management
• Where we are today – typical patients
• Management of concomitant pain
– Particular problems
– Common pitfalls
What is substance dependence?
ICD-10 defines dependence as:
• a cluster of physiological, behavioural, and
cognitive phenomena in which
• the use of a substance takes on a much higher
priority for a given individual than other
behaviours that once had greater value.
• The desire to take the psychoactive drugs,
alcohol, or tobacco is strong or overpowering
and
• relapse after a period of abstinence leads to a
more rapid reappearance of other features of the
syndrome than occurs with nondependent
individuals.
Making a diagnosis
A diagnosis of dependence would be made if three or more of the
following criteria have been present together at some time during
the previous year:
1. A strong desire or sense of compulsion to take the substance;
2. Difficulties in controlling substance-taking behaviour in terms of its
onset, termination, or levels of use;
3. A physiological withdrawal state when substance use has ceased or
has been reduced, as evidenced by: the characteristic withdrawal
syndrome for the substance; or use of the same (or closely related)
substance with the intention of relieving or avoiding withdrawal
symptoms;
4. Evidence of tolerance, such that increased doses of the
psychoactive substance are required in order to achieve effects
originally produced by lower doses.
5. Progressive neglect of alternative pleasures or interests because of
psychoactive substance use, increased amount of time necessary to
obtain or take the substance or to recover from its effects;
6. Persisting with substance use despite clear evidence of overtly
harmful consequences, such as liver damage through excessive
drinking, drug-related impairment of cognitive functioning, and
damage to relationships.
What drugs are we talking about?
•
•
•
•
•
•
•
•
Heroin
Cocaine/crack
Amphetamines
Benzodiazepines
Cannabis
Alcohol
‘Club drugs’
OTC/prescribed drugs
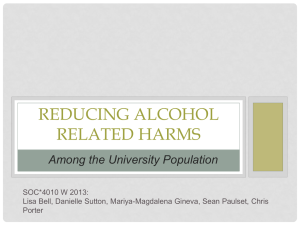
Drug misuse prevalence – Class A
Prevalence – non-class A
Treatment population is getting
older….
http://www.nta.nhs.uk/uploads/statisticsfromndtms201112vol1thenumbersfinal.pdf
Heroin “Brown” “B”
• Brownish powder, about 30% pure
• Smoked on foil using a tube to inhale
• Dissolved in water with citric acid
• Drawn up through a filter
• Injected – often using femoral vein in groin
Harms:
• Heroin itself not very harmful
• Main harms due to injecting and lifestyle
Cocaine
Cocaine:
• White powder –purity much less and now
much cheaper
• Usually snorted via tube
Harms
• Paranoid psychosis
• Hypertension
• Cardiac: 25% MI’s in under 45’s
• Liver damage if mixed with alcohol due
formation of hepatotoxic cocaethylene
Crack “White” “W”
•
•
•
•
Pale waxy crystals
Smoked via pipe – many home made
Injected, often with heroin – “speedballing”
Strong compulsion to continue – users can spend many
£100’s in a binge
• Lasts 25 mins – 1 hour
• Unpleasant withdrawals within 3 hours
• Associated with alcohol/bz use to ameliorate ‘comedown’
Harms
• Crack lung – allergic alveolitis, (plastic/aluminium fumes)
• Emphysema/COPD
• Associated with higher risk DVT in groin injectors
Benzodiazepines
Pattern of use varies
• Bingeing common – eg 3-10 x 10mg diazepam
• To ameliorate crack withdrawals
• As a hypnotic
• Inadvertent use – common adulterant of H
Harms
• Risk taking behaviour
• Retrograde amnesia
• Withdrawal fits
• Associated high proportion fatal overdoses
Cannabis “Weed” “Puff”
• Smoked rolled with tobacco: “spliff”
• Smoked alone with a pipe
Harms
• Apathy
• Depression
• Psychosis
• Withdrawal insomnia
Amphetamine “Speed” “Whizz”
•
•
•
•
•
•
White/off white powder
Traditionally highly impure
Ingested wrapped in cigarette paper
Rubbed into gums
Snorted
injected
Club Drugs
• Numbers small but steady increase (in contrast to
other drug prevalence in UK)
• Different cohort – young, gay scene
• Usually oral, some injecting
–
–
–
–
Ecstasy/MDMA – hyperthermia, rarely death
Ketamine – interstitial cystitis, psychosis
Mephedrone (M-CAT, Miaowmiaow)
GHB/GBL (‘G’) – overdose, physiological withdrawals
• New club drug clinics – treatment:
– Detox for ‘G’ – v high dose bzs needed
– Psychological support - all get low mood
– Outcomes good
OTC/prescribed drugs
•
•
•
•
•
Codeine/dihydrocodeine
Tramadol
MST/oramorph/fentanyl
Benzodiazepines/z’s
Gabapentin/pregabalin
Prescribed medication abuse
Primary prescription opioid addiction
• Escape from reality
• US - oxycodone now commonest drug prescribed
• Legal, available OTC
Secondary to illicit drug use
• Opioid withdrawal
• Enhance effects of illicit drugs
• Saves money in a tight corner
Particular circumstances in prisons:
• Boredom
• Currency
• Status
EFFECTS OF DEPENDENT DRUG USE [1]
Physical:
►Dependence
► Effects of poverty
► Poor pregnancy outcomes
► Side effects of Opioids (constipation, low
salivary flow affects dentition)
► Side effects of Cocaine (vasoconstriction,
local anaesthesia)
►Complications of injecting
•
•
•
•
•
•
DVT and post-phlebitic syndrome
Leg ulcers
abscesses
overdose
SBE
Blood borne virus transmission – up to
50% prevalence Hep C in IVDUs (HIV and
Hep B much rarer
“Shooting up” - HPA
•
One in six people who inject drugs had ever been
infected with the hepatitis B virus in 2011.
•
Hepatitis B infection among people who inject drugs
has declined over the last decade.
•
This decline most probably reflects the marked
increase in the uptake of the hepatitis B vaccine
among people who inject drugs.
Among people who inject drugs in the UK:
•
Around half have been infected with hepatitis C
•
Around one in every 100 has HIV.
•
Almost one-third report a symptom of a bacterial
infection (such as a sore or abscess) at an injecting
site in the past year.
•
Around one-sixth of people who inject drugs continue
to share needles and syringes. (Far < 10 yrs ago)
EFFECTS OF DEPENDENT DRUG USE [2]
Social:
► Effects on families
► Drive to criminality
► Imprisonment
► Social exclusion
Psychological:
► Fear of withdrawal
► Craving
► Guilt (all temporarily alleviated by drug use)
Mental Health
► ‘Self Medication’
► Depression, Psychosis,
Dual Diagnosis
AIMS OF TREATMENT
To reduce harm to user, family, community and society
To improve health and prevent death
To stabilise physically and psychologically
To improve quality of life and social functioning
To address all issues and reduce harm associated with substance
misuse
To reduce crime
Substitute prescribing by doctors and non-medical prescribers is
only one part of treatment and can only succeed in conjunction
with adequate key worker and psychosocial support during and
after an individual being on substitute medication
HOW DO I DO A QUICK ASSESSMENT?
Which drugs ?
► Which ones?
► How much?
► Don’t forget – Alcohol, Cannabis, Tobacco
Route of administration ?
► Oral
► Inhaled/smoked
► Injected
How long had a problem with drugs?
► Any previous treatment episode/s?
Examination and Investigations
► Examination for injection sites etc
► Urine screen for Opioids and other drugs
Harm Reduction Advice
► Essential – polydrug (use of more than one drug +/- Alcohol)
use now normal
BASIC HARM REDUCTION
National Guidelines state all practitioners should be able to provide the
following:
Retaining patients in high quality treatment is protective against overdose
► not injecting, injecting more safely, not using drugs alone
► reducing amount taken after intervals where
tolerance is lost
► training drug users and their families in risks of overdose and how to
respond in an emergency
Action to prevent blood borne virus transmission
► not sharing needles etc
► safer sex (condoms)
► provision of Hepatitis A and B vaccination
► blood borne virus screening including Hepatitis C
Referral where appropriate
► specialist drug services
► voluntary sector services
► infectious diseases services
The ‘British System’
• 1920’s heroin prescribed; sanctioned in UK (1) as
addiction treatment (in contrast to USA)
• 1956 USA banned all medicinal use of heroin
• 1959 only 4 countries still prescribing H, ban had
spread worldwide
• 1950s -60s – ‘the British system’: compassion and
clinical freedom - some Drs prescribing heroin
privately to addicts (2)
• 1967s – mandatory licensing for heroin prescribing only awarded to doctors in specialist clinics (3)
• 1980s -massive waiting lists in clinics
• 1988 - AIDS - ACMD recommends expansion of
methadone prescribing as harm minimisation (4)
1990s typical patient
• Largely male (5/6), mid to late 20’s
• Waiting many months for treatment
• Usually injecting and sharing, mostly heroin, some
crack
• Committing daily acquisitive crimes, around
£100/day
• Lottery of treatment philosophy & availability
• Poor engagement in treatment – very unstable
• Frequent diversion of substitute medication
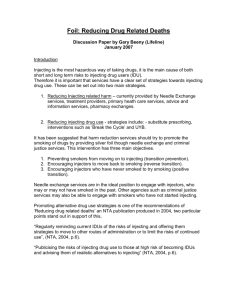
Impact on on Crime
CRIME
NTORS
10 year drugs strategy
AIDS
Harm minimisation agenda
Increase numbers in treatment
Money
Pooled Treatment Budget
Targets
Coercive treatment
Policy
National Treatment Agency
Crime and disorder Act
2000’s – The NTA
• ‘Models of Care’
– Consistency of treatment policy
– Ending postcode lottery
•
•
•
•
Emphasis on harm minimisation
Recruitment of GPs
Supervised consumption in pharmacies
Detox and rehab out of favour
Harm minimisation gains
• Targets achieved
– Treatment number doubled early
– Waiting times dramatically reduced
– DRDs almost halved
• NICE and DH 2007 – evidence is for high
dose maintenance, minimum 12 weeks
• New targets to Retain in Treatment
• Monitoring of doses
2007 – typical patient
•
•
•
•
•
•
•
•
Mostly male (4/5) mid to late 30’s
Alcohol rare, usually problematic if drinking
Methadone 60 -120mg (4/5)
Buprenorphine 8 -16mg (1/5)
Stopped injecting
Some still using C+H smoked
Never tried detox or rehab
Stable pattern for 2-7 years
2010 – The Recovery Agenda
•
•
•
•
•
•
•
•
Patient and advocate complaints
Conspiracy theories
Opposition perceives lack of progress
2010 – new party in power
New targets on treatment EXIT
Emphasis on dose reduction and detox
Increased support for detox, rehab facilities
Promotion of recovery groups/networks
Current themes
• Alcohol is cheap, widely available
• Fewer young people starting to use heroin
• Recession
– Less housing
– Fewer jobs
– Benefits about to be cut
• Health and Social Care Bill:
– NTA disappears into Public Health
– Drug Treatment budget disappears into LAs
2013 – typical patient
•
•
•
•
•
•
•
•
•
Predominantly male (3/5) early to mid 40’s
Using alcohol, often problematically
Methadone 40 - 80mg (4/5) and reducing
Buprenorphine 4 - 8 mg (1/5), reducing
Stopped injecting
Some still using C + H smoked (but fewer)
Associated Benzo use is common
Had a go at detox/rehab/recovery group
Chronic diseases starting to manifest – eg:
Hep C, venous ulcers, COPD, cancers
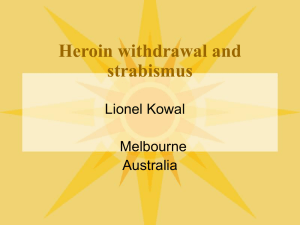
Treatment journey: Drugs services in Leeds
Untreated
drug use
Social
exclusion
Community
treatment
Criminal
Justice
City
And
Sh care South
Recovery
and
reintegration
Sh care
IDTS
(HMPArmley)
Needle
exchange
DRR
Recovery
Groups
Sh care
Sh care
Leeds
Community
Drugs
Partnership
Sh care
Multiple
Choice
Aftercare
WNW
Sh care
Detox
Sh care
Harm
reduction
York
Street
(homeless)
Rapid
Access/
Arrest
referral
Platform
Young
people
ENE
Sh care
Rehab
Sh care
Leeds
Addiction Unit
Preganacy
Dual diagnosis
Highly complex physical
The
Space
Single Point of Access
• In all but name!
Citywide Harm Reduction Service
0113 242 1161
Pain – Technical problems of
treating in opioid misuse
– Opioid tolerance
– Lowered pain threshold
– Most analgesics CNS depressants> risk OD
– Buprenorphine blockade
Pain – difficulties with rationale of
treating in opioid misuse
– No tests to diagnose pain or its extent
– Pain is common, and often long term
– Most analgesics are abusable
– Risk of diversion (selling on black
market)
Further information
Information on individual drugs:
http://www.drugscope.org.uk/resources/drugsearch/drugsearch
Prevalence data:
• British Crime Survey
• National Treatment Agency
Club drugs:
http://www.nta.nhs.uk/uploads/clubdrugsreport2012[0].pdf
Blood borne viruses:
http://www.hpa.org.uk/Publications/InfectiousDiseases/BloodBorneInfecti
ons/ShootingUp/1211Shootingup2012/
Thank you!
susi.harris@nhs.net