LF Achievements -2013
advertisement

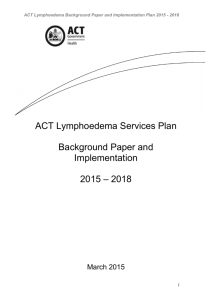
Elimination of Lymphatic Filariasis Country Scenario - India Directorate of National Vector Borne Disease Control Programme Directorate General of Health Services Ministry of Health & Family Welfare, Delhi (India) Elimination of Lymphatic Filariasis in India India – Population at Risk of LF JAMMU & KASHMIR HIMACHAL PRADESH PUNJAB UTTARAKHAND HARYANA DELHI ARUNACHAL PR. SIKKIM RAJASTHAN UTTAR PRADESH BIHAR GUJARAT MADHYA PRADESH ASSAM NAGALAND MEGHALAYA MANIPUR WEST BENGAL JHARKHAND TRIPURA MIZORAM CHHATTISGARH ORISSA DAMAN & DIU D&N HAVELI MAHARASHTRA ANDHRA PRADESH Endemic Districts Non-Endemic Districts GOA KARNATAKA A&N ISLANDS PONDICHERRY TAMIL NADU KERALA LAKSHADWEEP N W E S Endemic districts – 254 (in 21 States/UTs) Population at risk:600 million ELIMINATION OF LYMPHATIC FILARIASIS Elimination of LF : LF ceases to be a public health problem, when the number of microfilaria carriers is less than 1% and the children born after initiation of ELF are free from circulating antigenaemia Goal: The National Health Policy (2002) has set the goal of Elimination of Lymphatic Filariasis in India by 2015. Global goal to eliminate Lymphatic Filariasis (LF) as public health problem by 2020 through World Health Assembly resolution WHA 50.29. 3 GPELF overall framework Mapping MDA Post-MDA surveillance TAS M&E Situation 2. MMDP analysis Plan Minimum package of MMDP care Verification 1. MDA Dossier development VC/IVM MMDP and rehabilitation integrated into health services Lymphatic Filariasis Strategies for Elimination & Impact 2.00 90.00 86.69 87.92 86.42 86.07 1.50 84.50 83.09 8 2.91 81.86 80.00 Mf Rate (%) 100.00 Covg.% 1. Interruption of transmission by Annual MDA with DEC + Albendazole for 5 years or more to the population except: children below 2 years pregnant women seriously ill persons 2. Home based management of lymphoedema cases and upscaling of hydrocele operations in the identified CHCs / District hospitals/ medical colleges. 1.2 76.23 72.42 1.0 1.0 1.00 70.00 60.00 0.7 0.6 0.5 0.50 0.4 0.4 0.4 0.3 50.00 0.00 2004200520062007200820092010201120122013 Coverage% Impact of MDA 250 203 Number of Districts 200 142 150 100 76 50 30 19 6 1 0 2004 <1% 21 2013 1-5% >5% Not Done Scaling Down MDA • MDA to be stopped after minimum 5 rounds of MDA with >65% compliance against total population at risk and districts reporting less than 1% mf prevalence • WHO – 2011 guidelines simplified and capacity building initiated • 4 core trainers at Puducherry during July’12 • 139 state/district trainers during June-Oct’13 • 59 from 14 districts of UP trained in June’14 • 90 proposed in 2014-15 • 28 districts cleared TAS • 50 out of 62 completed Pre-TAS activity. TAS Plan for MDA Stoppage Number of Distt 150 102 100 90 50 40 14 4 0 2012-13 Achievement 4 2013-14 14 2014-15 2015-16 2016-17 10 Anticipated to stop MDA after Nov-Dec 2015 and finish TAS by June 2016 Lymphoedema Management demonstration- Andhra Pradesh Washing Demonstration Providing Morbidity management Kits Lymphoedema Management demonstration- Odisha Washing Demonstration Foot Exercise Lymphoedema Management demonstration- Tamil Nadu Training & Providing Kits of Soap, Mug, Towel 1 – 100 Cases 101 – 500 Cases 501 – 1000 Cases 1001 – 2000 Cases 2000 & above Cases Lymphoedema Management demonstration - Madhya Pradesh Training & Providing Kits of Soap, Mug, Towel Lymphoedema Management demonstration – Daman & Diu Providing Kits of Soap, Mug, Towel Hydrocelectomy • Hydrocelectomy is usually done in CHCs, district hospitals or medical colleges free of cost. • Programme emphasises to intensify the hydrocele operations in camp mode for more operations • The incentives to promote such activities are provided @ Rs.750 per case (US$ 12) • Rs. 250 to Surgeon, • Rs.50 to staff Nurse, • Rs.50 to Ward Boy/Attendant, • Rs.300 for medicine/dressing • Rs.100 to the patient towards travel expenses. • Some states pay more out of state resources but it varies from state to state Incentivized morbidity management 1. Incentives for Morbidity Management • Rs 750 per hydrocelectomy (camp approach) • Rs. 150 per Ly. Management Kit • Rs.200/- one time for line listing of lymphoedema and hydrocele cases 2. Financial Resources increased from Rs 250 cr (XI Plan) to Rs 400 Cr (XII Plan) for total ELF including MDA, MM, TAS. Hydrocelectomy Camp in Satna Distt of Madhya Pradesh Patient being operated Two patients being operated GUIDELINES Experiences • Tamil Nadu Model: • Tamil Nadu initiated by providing morbidity management kit from state resources. • Recently, Tamil Nadu has also approved to provide a monthly pension of Rs. 400 to grade-IV of lymphoedema patients. • CASA model in Odisha: • In Khurda district of Odisha, CASA – a NGO has taken 3 blocks and linelisted all the lymphoedema cases. • Engaged volunteers named as Task Force (1 per 20 patients). CASA engaged 15 health workers (1 per 20 Task Force/Volunteers) at the rate of Rs.3000 per month. • To monitor these health workers, four supervisors and one coordinator were engaged. • Provided the morbidity management services to each and every lymphoedema patients and maintained a card to monitor the improvement in their suffering. • CASA also helped during MDA programme of the district especially in IEC/BCC activities. Experiences • Madhya Pradesh Model: • The state provided morbidity management kit out of their own resources to the Lymphoedema patients. • They also organised hydrocele camps in district hospitals with lot of social mobilization and awareness generation. • Gujarat Model: • Gujarat has very strictly observed the activity of updating linelisting the lymphoedema and hydrocele cases for 15-30 days in preceding months of MDA in each district. • Mapped the prevalence of these cases village-wise. The morbidity management are provided to these patients and resources are mobilized according to the number of patients. Experiences • Kerala Model: • Kerala is known for presence of both W.bancrofti and B.malayi. • Prof. Shenoy group has been providing home based morbidity management services to the patients and keeping their records for regular monitoring and assessing the impact. • Dr.Narhari’s group at Institute of Applied Dermatology, Kasargode, Kerala is using Ayurvedic medicines combined with Yoga and getting the impact as per their reports. • In addition, state is following the national guidelines of morbidity management but its monitoring needs strengthening at ground level. Experiences • There are some groups working on surgical repair, sculpturing etc. in Tamil Nadu which includes: • Dr. Manoharan’s group at Chennai • Dr. Sivasubramaniyan’s group at Tamil Nadu, India. Settiarpatti, Rajapalayam, • Lepra India: working on Lymphoedema Management - In two districts of Andhra Pradesh and Bihar each. - After Line listing of Lymphoedema cases, they are classified and the Morbidity Management training are provided. - Shoes are also providing from their project. Major Achievements 877,594 Lymphoedema cases line listed. 407,307 Hydrocele cases line listed 110,842 Hydrocele operated 350 non endemic districts line listing initiated Involvement of CASA is appreciated and being expanded. Priority actions • Social Mobilization for improved drug compliance and morbidity management. • Supporting MDA and management of adverse reactions. • Involvement of faculties from medical colleges, Research Institutions and Regional Directors (GoI) for monitoring and independent assessment • Morbidity surveys and morbidity management for all patients individually and also at community level. • Motivating people suffering from Hydrocele to go for surgical intervention. • Involvement of NGOs/Voluntary organizations Partnership • State Governments • Other Government Departments • NGOs like CASA, Lepra India, IADKasargod • Medical Colleges • ICMR-VCRC Puducherry; RMRC Bhubneswar; RMRC Dibrugarh; CRME, Madurai • NCDC • Drug donors • WHO Joint Monitoring Mission Action Points (1) a) b) c) d) The Impact of last decade massive intervention is clearly visible in 2012 as follows: Coverage generally improved (73% in 2004, 86% in 2012), Microfilaria (mf) rate overall declined (1.24% in 2004, 0.45% in 2012), The program is on right track except in few districts with sub-optimal coverage, Phasing out MDA has started in 50 districts, 7 districts has cleared and 43 are in pre-TAS phase in 2014. • States preparing for next round of MDA • Completed 4 TAS workshops with WHO support • Planned 6 more TAS workshops for district level officials • 14 districts (IUs) and 21 IUs have successfully completed TAS JMM Action Points (2) • Districts >1% mf: MDA compliance should focus on poor-performing PHCs within the district for improvement and supplement vector control on IVM strategy with MDA • Districts <1% mf: TAS to be performed to stop MDA with technical support by ICMR / WHO • Efforts are on to improve compliance especially in poorperforming areas • IVM is already in vogue and providing co-lateral benefits • 96 districts are planned for TAS in 2014-15 out of which 55 have validated mf prevalence <1% JMM Action Points (3) • Provision of Lymphoedema management services at PHCs • expansion of hydrocele operations at CHCs/ District Hospitals to be established under NHM. • IEC/BCC to be strengthened to raise awareness • Morbidity management to continue even after stoppage MDA – continued support is required • Already emphasized in PIP guidelines • Hydrocele operation at District Hospitals is regular phenomenon. Incentives are provided for camp approach. • To strengthen IEC/BCC, flexibility for use of funds is provided. • Yes it will continue JMM Action Points(4) • Post MDA surveillance to be performed as per guidelines – at least two TAS after every 2-3 years. • Support to assess new (ICT) /additional (i.e. antifilarial antibody) diagnostic tools for surveillance and alternative surveillance strategies (i.e. xenomonitoring) to ensure the interruption of transmission. • The “hot-spots” (with persistent high case burden) to be under intensive surveillance for treatment and interventions • Post MDA surveillance draft National guidelines circulated Second TAS as per guidelines will be followed • Still under multi-centric trial phase. • The “hot-spots” are being covered under treatment and interventions. However, Independent Appraisal of ELF programme is also going on in 12 districts of 6 states and detail recommendations will be available in August. Independent Appraisal • • • • Independent Appraisal through ICMR (VCRC) 1st briefing meeting on 20th June,2014 1st phase field visit for secondary data from 1-3 July, 2014 2nd Phase field visit for primary data from 14-26 July, 2014 S.No. Name of state Name of District 1 Bihar Muzaffarpur, Khagria 2 Gujarat Valsad, Surat 3 Madhya Pradesh Damoh, Panna 4 Odisha Ganjam, Khurda 5 Telangana Karim Nagar, Nalgonda 6 West Bengal West Medinipur, Bankura Update on Independent Appraisal • Bihar : Governance at state/distt level is crucial but grass root workers are aware and can improve • Gujarat : showing impact but coordination in corporation and state Directorate needs attention for monitoring to tackle migratory population • MP : Mf rate in certain blocks is high due to suboptimal performance • Odisha : Priority affects performance in some areas (malaria is main priority) • Telangana : high Mf rate in certain blocks reflects suboptimal performance • West Bengal : Progressed well video conferencing from Director NVBDCP & MD to DC followed by letters has given priority in districts 4/13/2015 ELF - PKS 30 Hard core Districts State District Assam Bihar Dibrugarh, Sibsagar Begusarai, Buxar, Jahanabad, Khagaria, Munger, Muzaffarpur, Saharsha, Shekhpura, Sheohar, Sitamarhi, Vaishali Surat Dumka, Goda, Lohardaga Gulbarga Gadchiroli, Nagpur Nalgonda Ganjam Banda, Barabanki, Faizabad, Gorakhpur, Kheri, Sohanbadra Bankura, Burdwan, Purulia ELF - PKS Total Gujarat Jharkhand Karnataka Maharashtra Telangana Orissa Uttar Pradesh West Bengal 4/13/2015 No. 2 11 1 3 1 2 1 1 6 3 31 31 Hot Spot Areas identified for focused attention • Assam –Tinsukhia, Karbi Anglong, Naugaon, Sonitpur (Tea estates & patchy population) • Odisha – Sambalpur, Bolangir, Bargarh, Keonjhar, Kandhamal • Madhya Pradesh – Narsinghpur, Shivpuri, Panna • Gujarat – Surat migratory poulation Way Forward 1. Tackling Hard core Distt, Hot spot Areas & Migratory Population ( Expert Panel) 2. National TAS & Post TAS Guidelines draft ready and to be printed for circulation 3. Phasing out MDA • Transmission Assessment Survey using ICT in all districts (WHO to be requested for facilitating ICT supply) 4. Morbidity Management - Intensification 5. Programme Appraisal 6. Sustaining Achievement through Post MDA Surveillance 7. Validation of Achievement 8. Elimination Certification Thank You