Primary Health Care Nurse Practitioners
advertisement

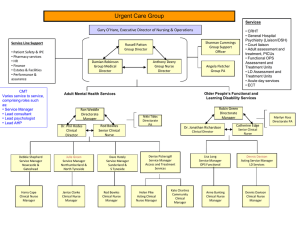
Georgina Nurse Practitioner-Led Clinic Cliniques dirigées par du personnel infirmier praticien Georgina The Georgina NPLC: Part of the South Simcoe and Northern York Region Health Link Beth Cowper-Fung NP-PHC, BScN, MN Clinic Director January 24, 2013 Objectives • • • • • • Introduction to the NP role The Georgina NPLC Caring for seniors Complex Case Load Management Challenges Advantages for and with Health Links Primary Health Care Nurse Practitioners • A nurse practitioner (NP) is a registered nurse with advanced university education who provides personalized, quality health care to patients. • Education and certification process includes a 4 year undergraduate in nursing, an average of 5 years clinical experience, a 2 year post degree certificate program (many PHC-NPs are also Masters Prepared), an additional registration exam into the RN Extended Class • We are registered and governed by the College of Nurses of Ontario and are held to a higher standard and Quality Assurance process than other nurses Primary Health Care Nurse Practitioners • Ontario nurse practitioners provide a full range of health care services to individuals, families and communities • NPs work in collaborative partnerships with physicians, Nurses, Dieticians, Social Workers, Midwives, Mental health professionals, Pharmacists and more. • NP’s provide full primary care for all ages and can assess, diagnose illness, order laboratory tests, order most diagnostic tests and write prescriptions (non-federally regulated meds) • If a clinical situation is beyond the knowledge, skill and experience of the NP they have a collaborative relationship with a physician for support The Georgina NPLC: The Model of Care Vision :Bridging the gap through collaborative care. Nurse Practitioner-Led Clinics are a model in which nurse practitioners are the lead providers of primary health care and work within an interdisciplinary health care team to provide comprehensive, accessible, and coordinated family health care services to populations who did not previously have access to a primary care provider. The focus is to improve quality of care through enhanced health promotion, disease prevention and chronic disease management, as well as improve care co-ordination and navigation of the health care system at the local level. The Georgina NPLC: The Model of Care • • Patients registered to the clinic have access to: • Primary Care Nurse Practitioners – all ages • Sr. Social Worker (counsellor) • Registered Dietitian • Registered Practical Nurse (lab, foot care, spirometry) • Pharmacist • **New next month Ontario Telemedicine Network Additional Services provided on site • DEC from Southlake • Ultrasound • Counsellor (Catholic Community Services of York Region) Georgina Nurse Practitioner-Led Clinic Southlake Regional health Centre Pre and post hospital care York region Public Health Sexual health outreach to local high schools Sunnybrook Home for Specialized Care Primary health care outreach, Skills workshop Cliniques dirigées par du personnel infirmier praticien Georgina Chippewas of Georgina Island Primary health care outreach to Georgina Island health center Georgina Nurse PractitionerLed Clinic Sandgate Women’s Shelter Primary health care outreach, Skills Workshop Lakeview Diagnostic Cervices On site Ultrasound Sutton Youth Multiservice Centre Primary health care outreach Catholic Community Services of York Region Shared space within clinic Diabetes Education Center Diabetes management and outreach Caring for Seniors • • • • Our building has been a clinic for almost 50 years When the clinic changed over to the GNPLC in July 2011 most of 800 patients previously cared for by a senior physician stayed with the clinic and transferred care to an NP. Many of these persons are over 65 Our average number of visits is 2.3 visits per quarter (9.2 visits per year) Data restriction: Nightingale does not have extractable data by age without much manual manipulation Caring for Seniors • • • • NPs have longer appointment times that allow for seniors to discuss their health concerns The NPs focus on health promotion and disease prevention supports patients in making healthy choices There are several studies that identify NPs as having excellent outcomes with chronic disease management and patient satisfaction The team based interdisciplinary model of care provides an excellent environment for coordination of a care plan Complex Case Load Management • • • • • Many seniors have registered with the clinic who have not been seen by a PCP in several years They present with a list of concerns and unclear, irretrievable histories It takes several visits to address all of the chronic diseases and begin to manage them effectively Several seniors with mental health diagnoses that have been poorly or not managed Several female patients felt that after children they did not need to be seen by a provider - multiple unmanaged illnesses (breast cancer, pelvic masses) Challenges • • • • • Patients present with multiple concerns on each visit – managing expectations and time Polypharmacy with specialists and from ED visits Referrals to specialists can take up to a year depending on the specialty Lack of secondary specialist reports (if a specialist transfers to another specialist the reports are often not forwarded to the Primary Care Provider) Lack of electronic data transfer from our local hospital (we are working together on this goal) or from specialist offices (still on fax service) and often do not inform the clinic of appointments Advantages with Health Links • • • • • Coordinated, efficient, timely access to hospital reports Faster access to specialists (hopefully also electronic) and their consultation notes in a timely fashion Care plan information sharing with the local hospital so that pre admission status is available for the hospital and post d/c information and instructions are available for primary care Improved data collection – NP data is invisible at this time Consistent data collection to provide for analysis and care plan modification as demonstrated by the findings Thank You • For your Time and Attention Resources • • • • • Nurse Practitioners’ Association of Ontario www.npao.org College of Nurses of Ontario www.cno.org (look for Extended Class Present and Future) Canadian Nurse Practitioner Initiative www.cnpi.ca or through CNA website Health Regulatory Professions Advisory Council www.hprac.org Visit our web site at : www.gnplc.ca Nurse Practitioners – Government Reviews/Reports Federal Romanow Report (2002) –Theresa Agnew spoke for NPAO; members encouraged to present Kirby Report (2002) – Linda Jones presented; NPAO submission; CNPI Initiative (2003-2006) – NPAO members actively involved Provincial Report to the MOHLTC on the Review of the Scope of Practice for RN(EC)s – HPRAC; Pam Pogue presented and members actively participated Report of the Task Team on PHC Integration – co-chaired by Dr. Alba DiCenso and Dr. Sue Matthews (2008); Theresa Agnew committee member; members chaired/participated in working groups and members participated Report on the Integration of PHC Nurse Practitioners in Ontario (aka IBM Report) – co-chaired by Dr. Alba DiCenso and Nursing Secretariat (2004); Theresa Agnew and Sharon Goodwin represented NPAO; members participated Panel on Health Professional Human Resources (aka George Report) - Sharon Goodwin appointed to Steering Committee (2001) Nursing Task Force Report (1999) and JPNC Progress Report (2001) Health Services Restructuring Committee, Primary Care Strategy (1999) Report of the Fact Finder on Physician Resources in Ontario (aka McKendry Report) (1999) NDP government Nurse Practitioner Initiative - Utilization of Nurse Practitioners in Ontario (1993); The Clinical Nurse Specialist, Clinical Nurse Specialist/Nurse Practitioner and Other Titled Nurse in Ontario (1994), Assessment of the Need for Nurse Practitioners in Ontario (1994) Additional References Supporting NP Care for Chronic Disease Management Horrocks,S. Anderson E, Salisbury,C. Systematic review of whether nurse practitioners working in primary care provide can provide equivalent care to doctors. BMJ. 2002 Apr 6: 324(7341): 819-923. Laurant, M, Reeves, D, Hermens R, Braspenning J, Grol, R, Sibbald, B Substitution of doctors by nurses in primary care (Review). Cochrane database of systematic reviews (online) 2009; art no. cd001271 DOI: 10.1002/14651858.cd001271.pub 2(4): 1-40. Lenz, ER, Mundinger, MO, Kane, RL, Hopkins, Lin, SX Primary care outcomes in patients treated by nurse practitioners or physicians: two year follow-up. Med Care Res Rev 2004 Sept, 61 (3) 332-351 Lenz ER, Mundinger MO, Hopkins, SC, Lin, SX, Smolowitz, JL. Diabetes care processes and outcomes in patients treated by nurse practitioners or physicians. The Diabetes Educator. 2002: 28 (4) 590-598. Litaker D, Mion, LC, Planavsky, L, Kippes, C, Mehta N, Frolikis, J. Physician-Nurse Practitioner teams in chronic disease management: The impact of costs, clinical effectiveness, and patients’ perception of care. Journal of Interprofessional Care 2003; 17(3) 223-237 Murchie, P Campbell NC, Ritchie,LD, Simpson, JA and Thain, J. Secondary prevention clincs for coronary heart disease: Four year follow-up of a randomized controlled trial in primary care British Medical Journal, 2003: 326 (7380) 84-87. Mundinger, MO, Kane, RL, Lenz ER, Totten, AM, Tsai W-Y, Cleary, PD et al, Primary care outcomes in patients treated by nurse practitioners or physicians: A randomized trial. JAMA 2000: 283(1) 59-68. Newhouse RP, Stanik-Hutt, J, White, KM, Johantgen,M, Bass EB, Zangaro, G et al. Advanced practice nurse outcomes 1990-2008: a systematic review. Nurs Econ 2011 Sept; 29(5): 230-250.