Atrial Myxoma

A lady with acute SOB
Sammi Pe
Case Presentation
• 54/F
• Cat II
• BP 129/69mmHg P 128
• Temp 36.9
• SpO2 78% ( 100% O2)
• Triage : SOB since afternoon, cough with sputum, mild chest discomfort
What will you do ?
What further history need?
What further Hx
• Good Past Health
• Domestic helper
• SOB since ~2 hrs ago
• Mild cough with yellowish sputum xdays become blood stained on AED
• No fever
• Chest discomfort today ( tightness)
• Palpitation +ve
More hx from employer
• Mild exertional SOB x several days
• Need resting after her work
• No fever all along
• No Travel hx
• Work in HK x ~17yrs
• No GI upset/ abd pain
• Not on regular medication
• Non-smoker, non-drinker
P/E
• Alert GCS 15/15
• BP 139/78 P 120
• RR 48
• Sit up for breathing
• SpO2 80% on 100% O2
• Recheck Temp 37.2
• H ’ stix 13.2
P/E
• Chest: AE fair with bilateral basal crep, occ wheeze
• Abd soft
• HS dual, no murmur
• No ankle edema
What will you do next ?
• ABC
• 100% O2 mask
• HB set
• Blood x CBC, L/RFT, Trop I , Clotting
• ECG
• i stat ( arterial)
• CXR
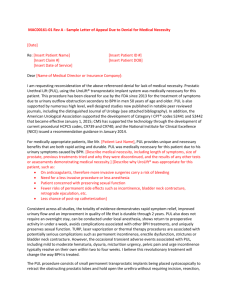
ECG x 2
i stat (arterial, on 100%O2)
• pH 7.398
• pCO2 5.39 kPa
• pO2 5.8 kPa
• BE 0
• HCO3 24.9 mmol/L
• SO2 79%
• Na 141 K 3.5 i Ca 1.21 Hb 14.6
Our Patient
Problem:
Sudden onset SOB
Desaturation even on 100% O2
Type I Resp Failure
What is yr DDx?
Type I Resp Failure
Typically due to V/Q mismatch
PaO2 low (< 60 mmHg(8.0 kPa))
PaCO2 normal or low
PA-aO2 increased
• Parenchymal disease ( V/Q mismatch)
• Diseases of vasculature and shunts: right-to-left shunt , pulmonary embolism
• interstitial lung diseases: ARDS , pneumonia , emphysema .
Patient was still in distress even on 100% O2
What will you do then?
• Patient was put on CPAP
• Lasix 40mg iv
• BP 110/70
• Clinically improved
• CXR film A/V … .
What is yr
Diagnosis?
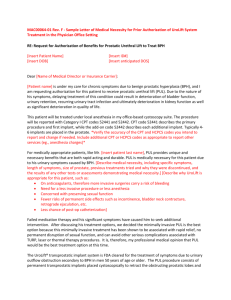
CXR
APO
…
.
? Other drug(s) to be considered
? Underlying cause
CCU was consulted
Medications…
• Nitrates
– Vasodilation
– Reduced preload and afterload
– Improved CO
– Rapid effect
– Not prescribed likely due to BP on low side
• Diuretics
– Reduced plasma volume / preload
– Pulmonary vasodilatation
• ACEI
– Reduced afterload
– Improved CO
Underlying Causes
• ACS
• HT
• Aortic/mitral valve disease
• Arrhythmias
• VSD
• Cardiomyopathy
• Acute myocarditis
• Pericardial disease
• Atrial myxoma
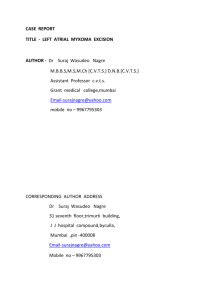
• Echo was performed…
What is show in the
Echocardiogram?
Our case
CCU input
• ECHO:
• LA mass ~4cm
• Likely atrial myxoma
• Trivial MR/AR
• Normal LV size and
EF
Our Patient
APO secondary to large atrial myxoma
• Transfer to CCU then CTSU for further
Mx.
Progress
• Emergency excision of atrial myxoma
– 6x5cm encapsulated LA tumour attached to inter-atrial septum.
– Causing obstruction & pul edema
– Bi-atrial exploration + excision of tumour
• Extubated on D1
• Post-op echo: EF 70%
• no PE
Day 0 Day 1
Day 2
Day 3 Day 4
Day 20
Patient was discharge on D8 and SOPD FU
On Day 20
Good Recovery, Class I II , ET 3-4 FOS
Atrial Myxoma
Background
Most common 1 ° Heart tumour (40-50%)
90% solitarty and pedunculated
– Multiple tumours occur in 50% of familial case
10% familial ( autosomal dominant)
75-85% occur in LA ~25% RA
Attach to fossa ovalis
Symptomatic ~ 70g 140g
• Myxoma-
– polypoid, round, oval in shape
– Smooth / lobulated surface
– White/ yellow/ brown
– Produce numberus growth factors and cytokines e.g. interleukin-6
Histology
• lipidic cells embedded in a vascular myxoid stroma
• In a series of 37 cases,
• 74% of tumors showed immunohistochemical expression of interleukin-6 while
• 17% had abnormal DNA content
Epidemiology
• US ~ 75 case / million autopsies
• 75% sporadic – Female
• Mean age – 56
• 15% present as sudden death
– tumour embolism, HF, mechanical obstruction
History
Asymptomatic (20%) symptomatic sudden death (15%)
Mechanical interference with cardiac fx embolization
LHF RHF systematic (L) Pulmonary (R)
Exertional SOB fatigue infarct / haemorrhage PE
Orthopnea peripheral edema of viscera Pul infarction
PND ascites e.g. CVA
Pul edema visual loss
Pul HT
Postural dizziness
Constitutional symptoms : fever, Wt loss, arthralgias, Raynaud ~ 50% of patient due to interleukin-6 overporduction
Physical
• ↑ JVP
• Loud S1
( delay mitral valve closure)
• Early diastolic sound (Tumor plop) tumor hit against the endocardial wall
• Diastolic atrial rumble
( obstruction in MV)
• MR/ TR
( valvar damage/ prolapse)
DDX
• Mitral Regurgitation
• Mitral Stenosis
• Pul Embolism
• Pul HT , primary
• Tricuspid Regurgitation
• Tricuspid Stenosis
Ix
• Lab: ESR, CRP, CBC, serum interleukin-6
• CXR
• ECHO
• need to differentiate thrombus from myxoma
– Thrombus ( in posterior portion, in layers)
– Myxoma ( presence of stalk and mobility)
• MRI
(point of attachment )
• CT scan
Treatment
• Medical treatment for CHF and arrhythmia
• Surgical excision is the definitive tx
• Safe and curative
• Recurrence is possible if incomplete excision